Blepharoconjunctivitis
Reading File
Finding Sources
Finding Sources
Searching PubMed
blepharoconjunctivitis
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive content from two major ophthalmology textbooks. Let me compile the full answer.
Blepharoconjunctivitis
Blepharoconjunctivitis refers to combined inflammation of the eyelid margins (blepharitis) and the conjunctiva occurring together. It is not a single disease entity but rather a descriptive term for the overlap of these two anatomically adjacent inflammatory processes.
Classification / Types
1. Staphylococcal (Anterior) Blepharoconjunctivitis
The most common infective form. Staphylococcus aureus plays a central role - an abnormal cell-mediated immune response to components of the S. aureus cell wall drives both the lid margin inflammation and secondary conjunctival involvement. It is more common and more marked in patients with atopic dermatitis.
2. Seborrhoeic Blepharoconjunctivitis
Associated with generalized seborrhoeic dermatitis (scalp, nasolabial folds, skin behind the ears, sternum). Eyelid involvement accompanies the systemic seborrhoeic state.
3. Posterior Blepharitis (Meibomian Gland Dysfunction) with Secondary Conjunctivitis
Meibomian gland dysfunction alters secretion quality. Bacterial lipases generate free fatty acids, increasing the melting point of meibum and destabilizing the tear film. This leads to tear evaporation, hyperosmolarity, and conjunctival inflammation. Strongly associated with acne rosacea.
4. Contact Allergic Blepharoconjunctivitis
A T-cell-mediated delayed (Type IV) hypersensitivity reaction. Common causes include eye drop constituents (e.g., preservatives, antibiotics), contact lens solutions, and occasionally mascara. Signs predominantly affect the eyelid skin (erythema, thickening, induration, fissuring) with variable conjunctival involvement.
5. Demodex-Associated Blepharoconjunctivitis
Demodex folliculorum longus (anterior form) and D. folliculorum brevis (posterior form) are mites found in hair follicles and sebaceous glands. Overpopulation or hypersensitivity to a carried bacillus may drive symptoms. Collarettes (cylindrical collections of partially digested epithelial cells, keratin, mite eggs) around lash bases are considered pathognomonic.
6. HSV Blepharoconjunctivitis
Herpes simplex virus can cause simultaneous eyelid skin vesicles and conjunctival inflammation. Treatment is antiviral - systemic (acyclovir 400 mg 5x/day, valacyclovir 500 mg twice daily, or famciclovir 250 mg twice daily for 7-10 days) or topical (ganciclovir 0.15% ophthalmic gel or trifluridine 1% for 7-10 days).
7. Drug-Induced Blepharoconjunctivitis
Isotretinoin and other retinoids can cause blepharoconjunctivitis, xerosis, and corneal changes as side effects, reversible on stopping the medication. Topical carbonic anhydrase inhibitors (e.g., dorzolamide) may rarely cause allergic blepharoconjunctivitis.
Symptoms
Symptoms are similar across forms and include:
- Itching, burning, mild pain
- Foreign body sensation
- Tearing
- Erythema and crusting of eyelid margins (worse upon awakening - in contrast to dry eye, which worsens later in the day)
- Mild mucous discharge
- Conjunctival injection and redness
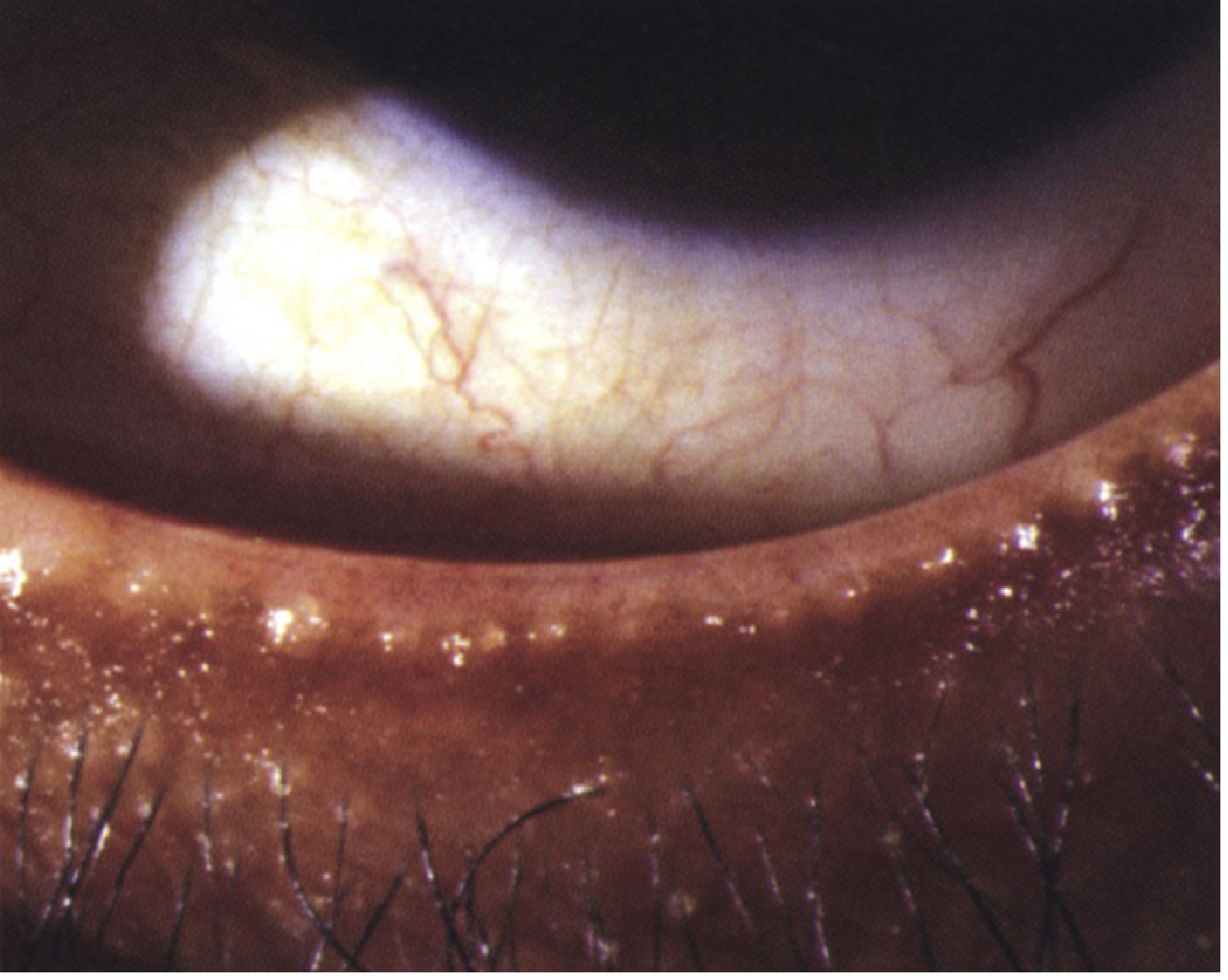
Signs
Critical signs:
- Crusty, red, thickened eyelid margins with prominent blood vessels
- Inspissated (blocked) meibomian gland orifices at the lid margin
- Collarettes and/or cylindrical sleeves around lashes (pathognomonic of Demodex)
- Hard scales and crusting around lash bases (staphylococcal)
- Greasy scales (seborrhoeic)

Other signs:
- Conjunctival injection and papillary reaction
- Swollen eyelids
- Superficial punctate keratopathy (SPK)
- Peripheral corneal infiltrates (staphylococcal hypersensitivity)
- Phlyctenules, pannus (in chronic cases)
- Rosacea facial signs may be present
Bilateral and symmetrical involvement is typical. Visual disturbance is uncommon.
Differential Diagnosis
| Condition | Distinguishing feature |
|---|---|
| Demodicosis | Cylindrical sleeves on lashes; confirm by microscopic examination of epilated lash |
| Pediculosis (lice) | Visible nits/lice on lashes |
| Ocular rosacea | Facial rosacea, telangiectasia |
| Contact allergic reaction | History of new topical agent; predominantly lid skin signs |
| Sebaceous carcinoma | Refractory, unilateral blepharoconjunctivitis in older patients - must always be excluded |
| Thyroid eye disease | Early symptoms may mimic blepharoconjunctivitis; upper eyelid retraction develops |
Important: Intractable, unilateral, or asymmetric blepharoconjunctivitis (particularly upper vs. lower eyelid asymmetry) is rarely a manifestation of sebaceous carcinoma of the eyelid and always warrants appropriate clinical workup. - Wills Eye Manual
Treatment
Treatment is stepwise and guided by severity and underlying type.
1. Eyelid Hygiene (all types, first-line)
- Scrub eyelid margins twice daily with a commercial eyelid scrub or mild baby shampoo on a washcloth
- Warm compresses for 5-10 minutes, 2-4 times per day
2. Tear Supplementation
- If associated dry eyes: preservative-free artificial tears 4-8 times per day
3. Topical Antibiotics (moderate severity)
- Erythromycin ointment or azithromycin gel-drop to eyelids at bedtime
- Staphylococcal blepharitis: erythromycin or bacitracin-polymyxin ointment 1-3x/day for 7 days
4. Anti-inflammatory Agents
- Cyclosporine 0.05%, cyclosporine 0.09%, or lifitegrast 5% drops twice daily
- Omega-3 fatty acid oral supplementation
5. Unresponsive Meibomitis / Posterior Blepharitis
- Topical antibiotic/steroid ointment (e.g., tobramycin 0.3%/dexamethasone 0.1% twice to three times daily)
- Oral doxycycline 100 mg once daily for 1-2 weeks, then taper to 25 mg/day and maintain for 3-6 months
- Azithromycin 500 mg/day x 3 days for 3 cycles with 7-day intervals as an alternative
- Note: Tetracyclines are contraindicated in pregnant women, nursing mothers, and children ≤8 years - use erythromycin 200 mg twice daily in these groups
6. Demodex-Specific Treatment
- Tea-tree oil eyelid scrubs or hypochlorous acid-based eyelid cleansing agents once or twice daily for a minimum of 6 weeks (if collarettes present and first-line treatment has failed)
7. Contact Allergic Type
- Discontinue the precipitant (eye drops, contact lens solutions)
- Mild topical steroid ointment can be helpful
8. HSV Blepharoconjunctivitis
- Systemic or topical antiviral therapy as described above (self-limited but treatment shortens course)
9. Advanced/Refractory Meibomitis
- Thermal treatment with meibomian gland expression
- Intense pulsed light (IPL) laser therapy
- Microblepharoexfoliation
- Meibomian gland probing
Follow-Up
- Review at 2-4 weeks depending on severity
- Eyelid scrubs and warm compresses can be reduced to once daily as the condition improves but may need to be continued indefinitely - blepharoconjunctivitis is a chronic, relapsing condition
Sources:
- Kanski's Clinical Ophthalmology: A Systematic Approach, 10th Ed., pp. 70, 189
- The Wills Eye Manual, Office and Emergency Room Diagnosis and Treatment of Eye Disease, pp. 348-351, 367
This is a shared conversation. Sign in to Orris to start your own chat.