Circle pf willis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Loading Image
Here is a complete overview of the Circle of Willis, drawn from authoritative medical textbooks:
Circle of Willis
Anatomy
The Circle of Willis (circulus arteriosus cerebri) is an anastomotic ring of arteries located at the base of the brain, on the ventral surface, surrounding the optic chiasm and pituitary stalk. It connects the anterior circulation (internal carotid arteries) with the posterior circulation (vertebrobasilar system).
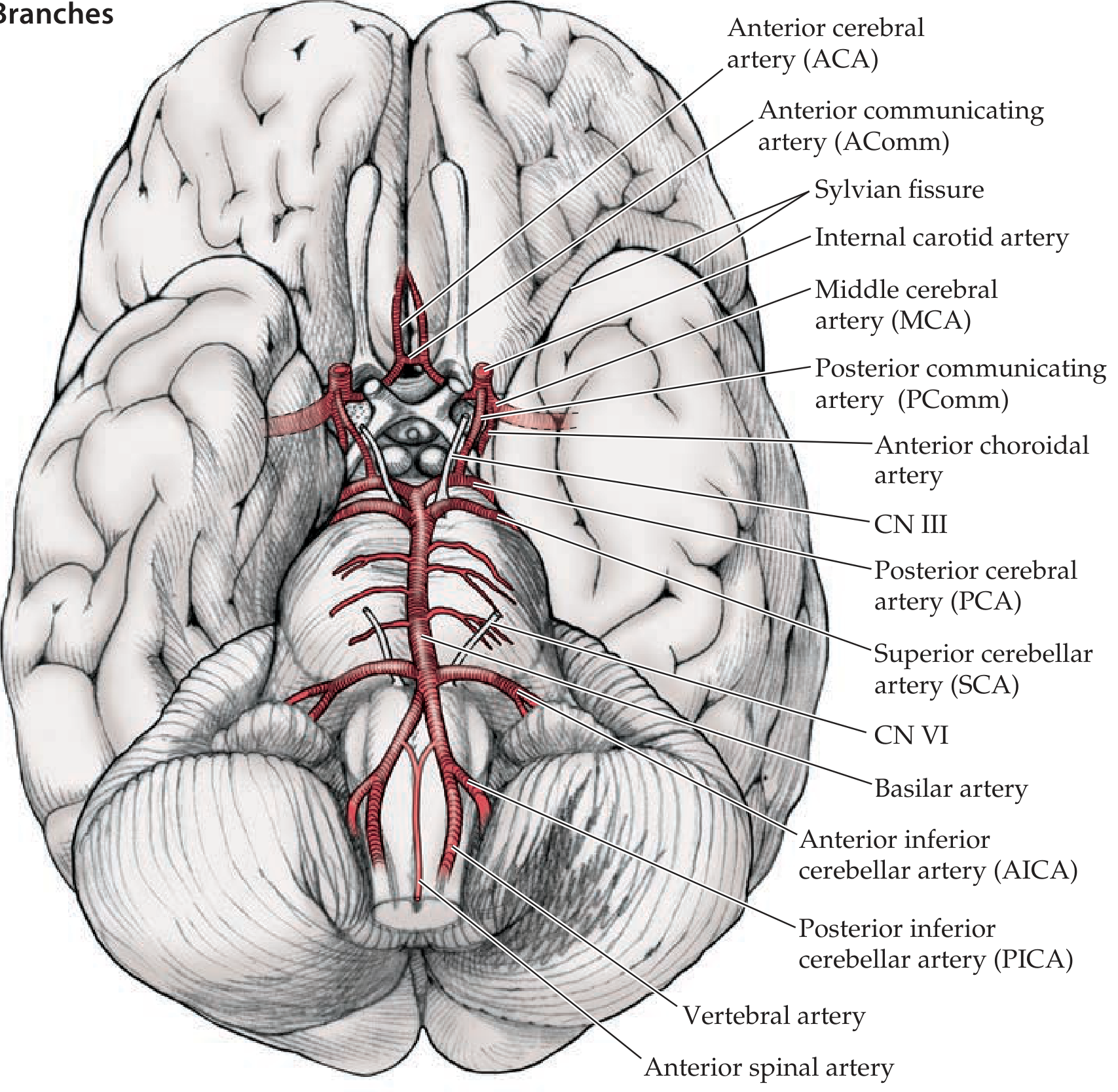
Circle of Willis and its main branches, viewed from the base of the brain - Neuroanatomy through Clinical Cases, 3rd Ed.
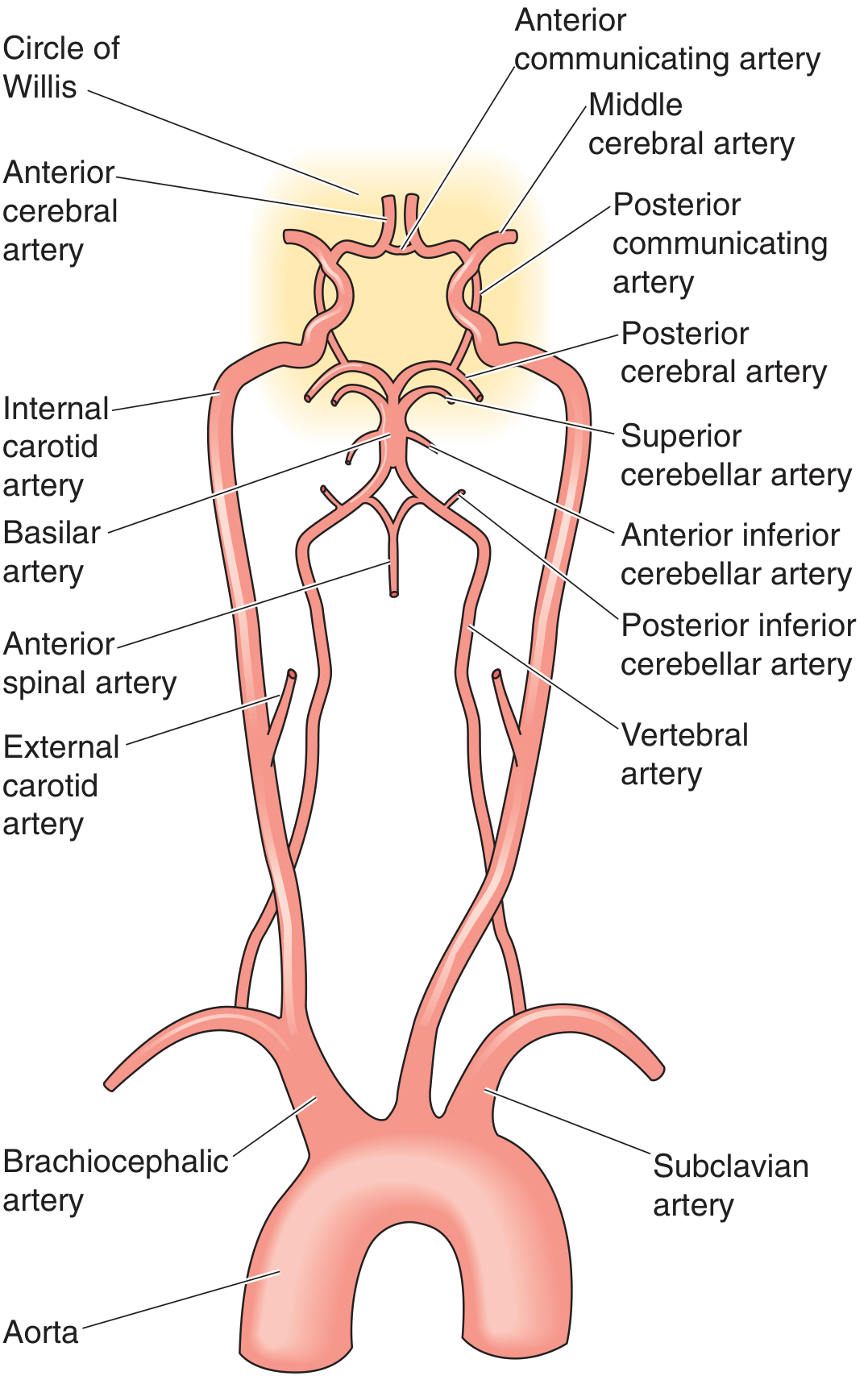
Full arterial supply from aorta to the Circle of Willis - Medical Physiology
Feeding Vessels
| Circulation | Origin | Vessels |
|---|---|---|
| Anterior | Internal carotid arteries (from common carotids) | ACA, MCA, AComm, PComm |
| Posterior | Vertebral arteries (from subclavian arteries) - merge to form basilar artery | PCA, SCA, AICA, PICA |
Component Vessels
The ring itself is formed by 7 named arteries:
- Anterior communicating artery (AComm) - bridges the two ACAs anteriorly
- Anterior cerebral artery x2 (ACA, A1 segment) - terminal branches of ICA; supply medial frontal and parietal cortex
- Internal carotid artery x2 (ICA) - the main inflow vessels from the anterior circulation
- Posterior communicating artery x2 (PComm) - link ICAs to the PCAs, joining anterior and posterior circulations
- Posterior cerebral artery x2 (PCA, P1 segment) - arise from the top of the basilar artery; supply occipital lobes and medial temporal structures
The Middle cerebral artery (MCA) arises from the ICA but is not technically part of the ring itself - it exits laterally into the Sylvian fissure.
Branches from the ICA (mnemonic: OPAAM)
The supraclinoid ICA gives rise to:
- O - Ophthalmic artery
- P - Posterior communicating artery
- A - Anterior choroidal artery
- A - Anterior cerebral artery
- M - Middle cerebral artery
(Neuroanatomy through Clinical Cases, 3rd Ed.)
Vascular Territories of Major Branches
| Artery | Territory Supplied |
|---|---|
| ACA | Medial frontal and parietal cortex, medial sensorimotor strip (leg area), corpus callosum |
| MCA | Lateral cortex (frontal, parietal, temporal), internal capsule, basal ganglia |
| PCA | Occipital lobe, medial temporal lobe (including hippocampus), thalamus |
| Deep perforators | Basal ganglia, thalamus, internal capsule (arise near the circle itself) |
Collateral Function
The Circle of Willis provides abundant collateral flow if one vessel is occluded. It connects:
- Right and left carotid systems (via the AComm)
- Anterior and posterior circulations (via the PComm)
Three main sources of brain collateral circulation exist:
- The Circle of Willis itself
- Extracranial-intracranial anastomoses (ECA-ICA connections)
- Leptomeningeal collaterals
(Localization in Clinical Neurology, 8e; Grainger & Allison's Diagnostic Radiology)
Anatomical Variants (Clinically Important)
A complete, full-caliber Circle of Willis is present in only ~34-40% of individuals. Common variants include:
- Absent or hypoplastic A1 segment (one side)
- Absent or hypoplastic PComm (one or both sides) - very common
- Fetal PCA - PCA arises directly from the ICA rather than the basilar artery (occurs in 20-30% of individuals); in this variant the P1 segment is absent/hypoplastic
- Persistent trigeminal artery - a fetal connection between the ICA and basilar artery that normally regresses; found in <1% of adults
Variants significantly reduce the effectiveness of collateral flow during occlusion. (Grainger & Allison's Diagnostic Radiology; Barash Clinical Anesthesia, 9e)
Clinical Relevance
1. Berry (Saccular) Aneurysms
The most common type of intracranial aneurysm. They form at arterial branch points within or near the Circle of Willis, where there is turbulent flow and structural stress.
Common sites (in decreasing order of frequency):
- Anterior communicating artery (AComm) - most common site overall
- Posterior communicating artery (PComm) - ICA-PComm junction
- Middle cerebral artery (MCA) bifurcation
- Basilar apex
- PICA origin
A PComm aneurysm classically compresses CN III (oculomotor nerve), causing a painful third nerve palsy with a dilated, unreactive pupil ("blown pupil").
Rupture causes subarachnoid hemorrhage (SAH) - sudden "thunderclap headache."
(Robbins & Cotran Pathologic Basis of Disease; Rosen's Emergency Medicine)
2. Ischemic Stroke
The competency of the Circle of Willis determines clinical outcome when a major vessel (e.g., ICA) occludes. A complete circle may allow enough collateral perfusion to prevent infarction; an incomplete circle worsens outcomes. (Schwartz's Principles of Surgery, 11e)
3. Surgical / Anesthetic Relevance
During carotid endarterectomy, the brain's blood supply depends entirely on collateral flow through the Circle of Willis when the carotid is clamped. Intraoperative neurophysiologic monitoring is used to assess adequacy of collateral perfusion. (Barash Clinical Anesthesia, 9e)
Sources: Neuroanatomy through Clinical Cases 3rd Ed. | Medical Physiology (Boron & Boulpaep) | Robbins & Cotran Pathologic Basis of Disease | Grainger & Allison's Diagnostic Radiology | Barash Clinical Anesthesia 9e | Localization in Clinical Neurology 8e | Schwartz's Principles of Surgery 11e
This is a shared conversation. Sign in to Orris to start your own chat.