Skin tb
Reading File
Finding Sources
Finding Sources
Searching PubMed
cutaneous tuberculosis
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive material. Let me compile the full answer.
Cutaneous Tuberculosis (Skin TB)
Cutaneous TB accounts for approximately 1-2% of extrapulmonary manifestations of tuberculosis. Its clinical presentation is remarkably varied, determined primarily by two factors: the route of infection (exogenous vs. endogenous) and the immune status of the host.
Causative Organisms
- Mycobacterium tuberculosis (predominant)
- Occasionally M. bovis and BCG (attenuated M. bovis) can produce skin lesions
- M. tuberculosis is an acid- and alcohol-fast bacillus with a waxy, high-lipid coat that resists degradation after phagocytosis
Classification
The classification is based on host immunity and source of infection:
| Route | Immunity | Clinical Form |
|---|---|---|
| Exogenous inoculation | No prior sensitization (low immunity) | Tuberculous chancre (primary inoculation TB) |
| Exogenous inoculation | Previously sensitized (high immunity) | TB verrucosa cutis |
| Endogenous spread | High immunity | Lupus vulgaris |
| Endogenous - contiguous spread | Low immunity | Scrofuloderma |
| Endogenous hematogenous | Low immunity | Acute miliary TB, tuberculous gumma |
| Endogenous hematogenous | Low immunity | Orificial TB |
| Immune reaction | High immunity | Tuberculids |
Clinical Forms
1. Tuberculous Chancre (Primary Inoculation TB)
- Occurs in non-sensitized (previously unexposed) individuals
- Develops at the site of direct inoculation - a painless, firm, red-brown papule or nodule that may ulcerate ("chancriform" appearance)
- Associated with regional lymphadenopathy (together forming the "primary complex")
- TST is initially negative, becomes positive within 4-8 weeks
- Self-healing but can disseminate
- DDx: sporotrichosis, blastomycosis, syphilis, tularemia, leishmaniasis, cat-scratch disease, atypical mycobacterial infection
2. Tuberculosis Verrucosa Cutis (Prosector's Wart)
- Exogenous inoculation in a previously sensitized person with strong immunity
- The classic "prosector's wart" from autopsy inoculation
- Begins as a small papule becoming hyperkeratotic and wart-like, enlarging by peripheral expansion with or without central clearing
- Surface may fissure with purulent discharge; lesions are almost always solitary
- Commonly on dorsum of fingers/hands (adults) and ankles/buttocks (children)
- TST strongly positive
- Histology: pseudoepitheliomatous hyperplasia, hyperkeratosis, suppurative and granulomatous inflammation; caseation rare; AFB scant
- Culture positive in ~50% of cases

3. Lupus Vulgaris (Most Common Form)
- Most common form of cutaneous post-primary TB
- Follows inoculation, scrofuloderma scars, or hematogenous/lymphatic spread
- ~50% have evidence of TB elsewhere - full systemic evaluation is mandatory
- Moderately high immunity; TST positive
- Classic appearance: single plaque of grouped red-brown papules with characteristic "apple jelly" color on diascopy (blanching with glass slide pressure)
- Dermoscopy: yellowish-orange patches indicating dermal granulomas
- Lesions are destructive and scarring, especially on the face (nose, cheeks); can result in disfigurement
- Slowly progressive, may develop squamous cell carcinoma in chronic lesions
- DDx: sarcoidosis, discoid lupus erythematosus, rosacea, lymphoma
- Histology: tuberculoid granulomas with or without caseation; AFB are few
4. Scrofuloderma
- Results from direct extension of underlying TB to the skin - usually from infected lymph nodes (cervical most common), bones, or joints
- Presents as firm subcutaneous nodules that soften, break down, and form sinus tracts with collar-stud abscesses and undermined ulcers
- Discharges thin, watery pus
- Heals with irregular, cord-like "bridge" scars
- Most common in children and elderly; cervical/submandibular region favored
- TST positive; AFB may be found; histology shows granulomatous inflammation with caseation
5. Orificial Tuberculosis
- Occurs in patients with advanced systemic TB (lungs, intestinal, urogenital)
- M. tuberculosis auto-inoculates onto mucocutaneous orifices from adjacent infected secretions
- Painful ulcers with undermined edges around mouth, anus, genitalia, or nares
- Indicates severe immunosuppression and poor prognosis
- AFB abundant on smear; TST often negative (anergy)
6. Acute Miliary TB of the Skin
- Due to hematogenous dissemination - a sign of overwhelming TB
- Pinhead-sized bluish-red papules capped by minute vesicles, developing central umbilication and crusting
- Heal leaving white scars with brownish rim
- Primary focus often in lungs
7. Tuberculous Gumma
- Also due to hematogenous spread (mycobacteremia with cutaneous seeding)
- Firm subcutaneous nodule that softens to form a fluctuant swelling
- Overlying skin breaks down to form an undermined ulcer with sinus tract formation
- Extremities more commonly affected than trunk
Tuberculids (Immune Reactions)
Tuberculids are skin eruptions representing immune reactions to hematogenous dissemination of M. tuberculosis or its antigens in patients with strong anti-TB cell-mediated immunity (CMI). The key features:
- TST/IGRA positive
- AFB usually NOT found in lesions (rapid immune destruction)
- Bilateral and symmetric distribution (hematogenous spread)
- Respond to anti-TB therapy
Papulonecrotic Tuberculid
- Asymptomatic, chronic, recurring crops of papules that undergo central necrosis
- Symmetrically distributed on extensor extremities (elbows, knees), dorsal hands/feet, buttocks, face, glans penis
- Most frequent in children and young adults
- Heals leaving varioliform scars
- Histology: wedge-shaped necrosis, vasculitis, granulomatous inflammation
Lichen Scrofulosorum
- Small, lichenoid follicular papules grouped in discoid clusters
- Usually on trunk; associated with lymph node or bone TB
- Asymptomatic; mainly in children and young adults
Erythema Induratum (Bazin Disease)
- Deep, tender nodules on the posterior calves that ulcerate
- Predominantly in women; associated with cold weather
- Histology: lobular panniculitis with granulomatous inflammation and vasculitis
- M. tuberculosis DNA demonstrable by PCR
Histopathology
- Early lesions: mixed infiltrate of lymphocytes, neutrophils, and plasma cells; AFB abundant
- Established lesions: tuberculoid granulomas - epithelioid macrophages, Langhans giant cells, lymphocytic cuffing, ± central caseation necrosis; AFB difficult to find
- The degree of caseation and AFB load inversely correlates with host immunity
Diagnosis
| Investigation | Details |
|---|---|
| TST (Mantoux/PPD) | Positive in most forms (may be negative in miliary/orificial TB due to anergy) |
| IGRA (QuantiFERON-TB Gold, T-SPOT.TB) | Measures IFN-γ response to ESAT-6 and CFP-10 antigens; more specific than TST |
| Skin biopsy + AFB stain | Look for acid-fast bacilli; often negative in paucibacillary forms |
| Culture (Lowenstein-Jensen medium) | Gold standard; slow (4-8 weeks); positive in ~50% of TB verrucosa |
| PCR | Can detect M. tuberculosis DNA in tissue; useful in paucibacillary forms and tuberculids |
| Chest X-ray / systemic workup | Essential in all confirmed cases |
Treatment
Standard regimens follow WHO guidelines for TB:
Initial/Intensive Phase (2 months):
- HRZE = Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E)
Continuation Phase (4 months):
- HR = Isoniazid + Rifampicin
Total duration = 6 months for most forms of cutaneous TB (same as pulmonary TB).
Key drugs:
| Drug | Class | Notes |
|---|---|---|
| Rifampicin | Rifamycin antibiotic | Broad spectrum; induces hepatic enzymes |
| Isoniazid | Synthetic | Specific for tubercle bacilli; pyridoxine supplementation needed |
| Pyrazinamide | Synthetic | Active in acidic intracellular environment |
| Ethambutol | Synthetic | Monitor for optic neuritis |
MDR-TB (resistant to at least H + R): requires second-line agents (fluoroquinolones, aminoglycosides, bedaquiline, delamanid, pretomanid).
Tuberculids also respond to standard anti-TB therapy; response to treatment helps confirm diagnosis.
Special Considerations
- HIV co-infection: ~20-37x higher risk of developing TB; more likely to present atypically; IRIS (immune reconstitution inflammatory syndrome) may worsen skin lesions after starting ART
- TNF inhibitors (biologics like infliximab, adalimumab): major risk factor for reactivation; screen with TST/IGRA before starting
- BCG vaccination: rare complications include local ulceration, lupus vulgaris-like lesions, and disseminated BCG infection (especially in immunocompromised infants)
- Long-standing lupus vulgaris can undergo malignant transformation to squamous cell carcinoma
Sources: Dermatology 2-Volume Set 5e (Bolognia), Chapter 75; Andrews' Diseases of the Skin, Chapter 16; Fitzpatrick's Dermatology, Chapter 157
Neck swelling sugery viva question and different diagnosis
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive information from multiple surgical textbooks. Let me compile the complete, well-structured surgery viva answer.
Neck Swelling - Surgery Viva
APPROACH TO A NECK SWELLING
The classic surgical approach to any lump applies here - the 7 S's of a swelling:
- Site - Midline vs. Lateral; which triangle of neck?
- Size - Dimensions in cm
- Shape - Ovoid, spherical, irregular
- Surface - Smooth, nodular
- Consistency - Soft, firm, hard (stony hard), cystic, fluctuant
- Skin over swelling - Normal, inflamed, fixed
- Special tests - Pulsatility, compressibility, transillumination, bruit, movement with swallowing, movement with tongue protrusion (thyroglossal)
CLASSIFICATION BY SITE
MIDLINE NECK SWELLINGS
(from above downwards)
| Level | Swelling |
|---|---|
| Submental | Ludwig's angina, submental lymph nodes, sublingual dermoid, lipoma |
| Hyoid bone level | Thyroglossal cyst, subhyoid bursitis |
| Thyroid region | Goitre (isthmus, pyramidal lobe), enlarged lymph nodes, lipoma |
| Suprasternal | Lipoma in space of Burns, retrosternal goitre, thymic swelling |
| Anywhere midline | Dermoid cyst |
LATERAL NECK SWELLINGS by Triangle
| Triangle | Swellings |
|---|---|
| Submandibular | Lymph nodes, enlarged submandibular salivary gland, deep/plunging ranula, jaw growth extension |
| Carotid triangle | Carotid aneurysm, carotid body tumour, branchial cyst, branchiogenic carcinoma; thyroid swellings (deep to SCM), sternomastoid tumour (neonate) |
| Posterior triangle | Enlarged supraclavicular lymph nodes (including Virchow's node on left), cystic hygroma, pharyngeal pouch, subclavian aneurysm, aberrant thyroid, cervical rib, lipoma |
CLASSIFICATION BY CHARACTER
Acute Swellings
- Cellulitis, Ludwig's angina
- Boil, carbuncle
- Acute lymphadenitis
Chronic Swellings
| Type | Examples |
|---|---|
| Cystic | Branchial cyst, thyroglossal cyst, dermoid cyst, cystic hygroma, sebaceous cyst, cystic adenoma of thyroid, cold abscess |
| Solid | Thyroid swelling, branchiogenic carcinoma, sternomastoid tumour, lymph nodes |
| Pulsatile | Carotid/subclavian aneurysm, carotid body tumour, lymph node with transmitted pulsation, primary toxic goitre |
DIFFERENTIAL DIAGNOSIS (COMPREHENSIVE)
1. Inflammatory / Infective
| Cause | Key Features |
|---|---|
| Reactive lymphadenitis | Tender, firm, mobile nodes; URTI/tonsillitis history |
| Tuberculous cervical lymphadenitis | Most common cause of cervical LN in Indian subcontinent; matted nodes, "cold abscess", "collar stud abscess", sinus tract formation; no pain/fever early |
| Bacterial adenitis | Streptococcus, Staphylococcus; tender, hot, may suppurate |
| Viral | EBV (infectious mononucleosis), HIV, CMV - bilateral, multiple nodes |
| Cat scratch disease | Bartonella henselae; unilateral nodes, history of cat scratch |
| Sialadenitis | Submandibular/parotid swelling; related to meals (submandibular duct stone) |
| Ludwig's angina | Diffuse, bilateral, floor of mouth + submental; life-threatening; oedema glottis risk |
| Thyroiditis | Tender thyroid, fever, may have transient thyrotoxicosis |
2. Congenital / Developmental
Thyroglossal Cyst (most important midline swelling)
- Origin: Persistence of thyroglossal duct (thyroid descends from foramen caecum to neck)
- Age: Mainly children, but any age
- Site: Midline, just below the hyoid bone (most common); can be at any level from foramen caecum to isthmus
- Pathognomonic sign: Moves upwards on swallowing AND on tongue protrusion (tethered to base of tongue via the tract)
- Character: Cystic, smooth, non-tender, fluctuant
- Complications: Infection, abscess, fistula, malignancy (papillary carcinoma in 1%)
- Investigation: Ultrasound to confirm (must confirm normal thyroid inferiorly); CT scan
- Treatment: Sistrunk operation - excision of cyst + central portion of hyoid bone + tract up to base of tongue (prevents recurrence)
Branchial Cyst
- Origin: Remnants of second branchial cleft (most common); lined by squamous epithelium
- Age: Young adults (does not manifest in childhood despite being congenital)
- Site: Junction of upper 1/3 and middle 1/3 of sternomastoid, at its anterior border (half in front, half behind SCM); upper/lateral neck
- Character: Soft, ovoid, fluctuant; surface smooth; long axis runs forwards and downwards
- Transillumination: Usually NEGATIVE (content is thick, turbid white fluid containing cholesterol crystals and desquamated epithelial cells)
- Diagnostic test: FNA shows cholesterol crystals - pathognomonic
- Key point: In patients >35 years, always exclude metastatic lymph node (necrotic) before assuming branchial cyst
- Treatment: Complete surgical excision (passes superficial to hypoglossal and glossopharyngeal nerves, deep to posterior belly of digastric; identify spinal accessory nerve)
Branchial Fistula
- Persistent second branchial cleft
- External opening: lower 1/3 of neck, anterior border of SCM
- Internal opening: anterior pillar of fauces, behind the tonsil
- May be unilateral or bilateral
Cystic Hygroma (Lymphangioma)
- Origin: Congenital lymphangioma - abnormal lymphatic development
- Age: Infants and children (usually present at birth or by age 2)
- Site: Root of neck, posterior triangle; may extend to axilla, mediastinum
- Character: Multilocular, brilliantly transilluminates (clear fluid); soft; fluid can be compressed from one locule to another; shows impulse on coughing if mediastinal extension
- Treatment: Sclerotherapy (OK-432, bleomycin) or surgical excision
Dermoid Cyst
- Midline, anywhere; smooth, doughy, non-fluctuant; does NOT transilluminate well; does NOT move with swallowing
Laryngocele
- Air-filled or mucus-filled; arises from laryngeal ventricle
- May be internal (within thyroid cartilage) or external (protrudes through thyrohyoid membrane)
- Increases with Valsalva/coughing; reducible
Cervical Rib
- Posterior triangle, supraclavicular; may cause thoracic outlet syndrome (vascular/neurological symptoms in arm)
3. Neoplastic - Benign
| Tumour | Features |
|---|---|
| Goitre | Moves with swallowing (attached to trachea/larynx); midline + bilateral; multiple types |
| Solitary thyroid nodule | Moves with swallowing; consider malignancy (10-15% risk) |
| Carotid body tumour (Paraganglioma) | At carotid bifurcation (C3-4 level, anterior to SCM); pulsatile, bruit; moves laterally but NOT vertically ("Fontaine's sign" or "potato tumour"); transmitted pulsation from carotid |
| Salivary gland tumour | Parotid (angle of jaw), submandibular; pleomorphic adenoma most common |
| Lipoma | Soft, lobulated, non-tender; posterior triangle common |
| Neurofibroma/Schwannoma | Moves horizontally but NOT vertically (tethered to nerve) |
4. Neoplastic - Malignant
Cervical Lymph Node Metastasis (most common malignant neck mass in adults >40)
- Features: Stony hard, irregular surface, fixed to skin or deep structures, painless, rapidly growing
- Majority: Deep to anterior border of SCM
- Search for primary:
- Above clavicle: Oral cavity (floor of mouth, tongue), tonsil, nasopharynx, larynx, thyroid, external auditory meatus, parotid
- Left supraclavicular (Virchow's node / Troisier's sign): Infraclavicular primary - stomach, colon, lung, breast, ovary, testis (via thoracic duct)
- Bilateral supraclavicular: Lymphoma or infraclavicular primary
Primary Lymphoma (Hodgkin's/Non-Hodgkin's)
- Young adults or elderly; rubbery-firm, multiple nodes; systemic "B symptoms" (fever, night sweats, weight loss)
- Hodgkin's: cervical nodes involved in 60-70% of cases
Thyroid Carcinoma
- Moves with swallowing; hard, irregular; may cause hoarseness (recurrent laryngeal nerve invasion), dysphagia, dyspnoea
KEY VIVA QUESTIONS
Q: What is the most important clinical sign of a thyroglossal cyst?
A: It moves upward on swallowing AND on protrusion of the tongue (pathognomonic - tethered to the foramen caecum via the tract through the hyoid bone).
Q: What is the Sistrunk operation?
A: Excision of thyroglossal cyst along with the central portion (body) of the hyoid bone and the tract up to the base of the tongue. Removing just the cyst without the hyoid leads to high recurrence rates.
Q: What is the content of a branchial cyst and how do you confirm diagnosis?
A: Thick, turbid fluid containing cholesterol crystals and desquamated squamous epithelial cells. FNA revealing cholesterol crystals is diagnostic.
Q: What is the difference between cystic hygroma and branchial cyst on transillumination?
A: Cystic hygroma transilluminates brilliantly (clear lymphatic fluid). Branchial cyst does NOT transilluminate (thick, turbid content).
Q: What is Virchow's (Troisier's) node?
A: An enlarged left supraclavicular lymph node due to metastasis from an infraclavicular primary tumour (classically gastric carcinoma). It receives lymph via the thoracic duct.
Q: What is a "collar stud" abscess?
A: Occurs in tuberculous cervical lymphadenitis when the deep cervical fascia is breached - pus tracks from a deep abscess through a small opening in the fascia to form a superficial abscess, giving a dumbbell/collar stud shape. Clinically: fluctuation is more easily elicited in the superficial component.
Q: What is a carotid body tumour and how does it differ from a pulsatile lymph node?
A: Carotid body tumour is a paraganglioma at the carotid bifurcation. It is truly pulsatile (expansile) with an audible bruit, and can be moved laterally but NOT vertically ("potato tumour" / Fontaine's sign). A lymph node near the carotid only shows transmitted (not expansile) pulsation.
Q: Which neck lumps move with swallowing?
A: Thyroid swellings, thyroglossal cyst (also moves with tongue protrusion), subhyoid bursitis (attached to hyoid). These structures are attached to the pretracheal fascia.
Q: What are the features of malignant vs. benign lymph nodes?
| Feature | Benign | Malignant |
|---|---|---|
| Tenderness | Present | Absent |
| Consistency | Firm/soft | Stony hard |
| Surface | Smooth | Nodular/irregular |
| Mobility | Mobile | Fixed (late) |
| Skin | Normal | May be adherent |
| Size | Usually <2 cm | Often >2 cm |
Q: What is Ludwig's angina?
A: Severe, rapidly spreading bilateral cellulitis of the floor of the mouth involving submandibular, submental, and sublingual spaces. It is a surgical emergency - the danger is oedema of the glottis causing asphyxia. Caused by dental infection (usually mandibular molar). Management: airway protection, IV antibiotics, surgical decompression.
INVESTIGATIONS FOR NECK SWELLING
| Investigation | Purpose |
|---|---|
| Ultrasound neck | First-line; cystic vs. solid, thyroid nodule assessment, guide FNAC |
| FNAC | Cytological diagnosis (lymphoma, metastasis, thyroid) |
| CT neck with contrast | Assess extent, vascular involvement, deep structures, staging |
| MRI | Soft tissue delineation, parapharyngeal lesions |
| X-ray chest/neck | Tracheal deviation, mediastinal widening, cervical rib |
| Thyroid function tests | If thyroid swelling suspected |
| Mantoux/IGRA | Suspected TB lymphadenitis |
| LDH, ESR, PET-CT | Lymphoma staging |
| Barium swallow | Pharyngeal pouch |
| Panendoscopy | Search for primary in head and neck malignancy |
Sources: S Das Manual on Clinical Surgery 13e, Chapter 26 & 27; Bailey and Love's Short Practice of Surgery 28e, Chapter 52; Sabiston Textbook of Surgery; Scott-Brown's Otorhinolaryngology & Head and Neck Surgery, Chapter 36; Rosen's Emergency Medicine
Create a visual comparison poster of branchial cyst vs. thyroglossal cyst vs. cystic hygroma
Generating Image
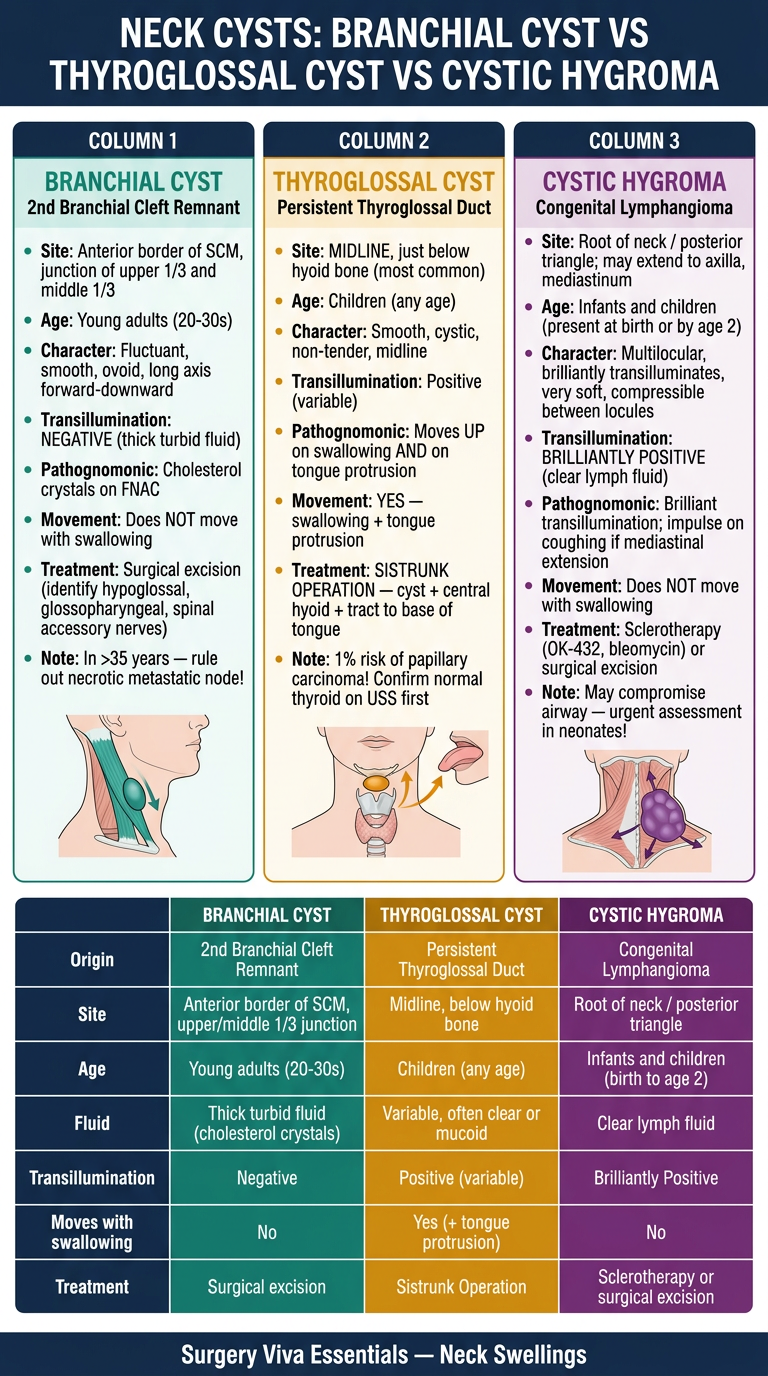
Here's your surgery viva comparison poster! Here's a quick summary of what's on it:
The 3 key differentiators to nail in a viva:
| Feature | Branchial Cyst | Thyroglossal Cyst | Cystic Hygroma |
|---|---|---|---|
| Site | Anterior border of SCM (upper 1/3 - middle 1/3 junction) | Midline, below hyoid | Posterior triangle / root of neck |
| Age | Young adults | Children | Infants / neonates |
| Transillumination | ❌ Negative | ± Variable | ✅ Brilliantly positive |
| Moves with swallowing | ❌ No | ✅ Yes (+ tongue protrusion) | ❌ No |
| Fluid | Thick, turbid, cholesterol crystals | Mucoid | Clear lymph fluid |
| Treatment | Surgical excision | Sistrunk operation | Sclerotherapy / excision |
The most commonly asked viva question is why thyroglossal cyst moves with tongue protrusion - because the tract is tethered to the foramen caecum at the base of the tongue through the body of the hyoid bone.
Chleak leak management
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from 4 major surgical textbooks. Let me deliver the full answer.
Chyle Leak Management
(Assuming you meant chyle leak - chylous fistula/chylothorax. If you meant something else, let me know.)
What is Chyle?
Chyle is a milky, white fluid containing:
- High concentration of triglycerides and chylomicrons
- Lymphocytes (predominantly)
- Fat-soluble vitamins, proteins, immunoglobulins
Normal thoracic duct flow: 0.5 - 3.0 L/day. Loss of this volume causes malnutrition, immunosuppression, and significant morbidity.
Anatomy - Why It Matters
- The thoracic duct ascends from the cisterna chyli through the right chest, crosses to the left at T4-5, and enters the neck to empty into the left subclavian vein at or within 1 cm of the junction with the left IJV
- It is more accurately described as a plexus of tributaries - any branch can create a fistula if transected
- Left-sided leaks: 75% - thoracic duct injury
- Right-sided leaks: 25% - right lymphatic duct injury (also important!)
Causes / Etiology
Iatrogenic/Traumatic (most common):
- Neck dissection (radical or modified) - 1-2% incidence
- Esophagectomy - 4.3% incidence
- Lung, mediastinal, or thoracic aortic surgery
- Subclavian vein catheterization
- Blunt/penetrating chest or neck trauma
Neoplastic:
- Lymphoma (most common non-traumatic cause)
- Lung, esophageal, mediastinal tumours
- Metastatic carcinoma
Infectious/Other:
- Tuberculous lymphadenitis
- Mediastinitis
- Congenital (most common cause of pleural effusion in neonates; associated with Down, Turner, Noonan syndromes)
- Lymphangioleiomyomatosis
- Venous thrombosis (superior vena cava)
Diagnosis
Clinical
- Neck chyle fistula (post-neck dissection): Drain output changes from serosanguinous to milky white after resumption of feeding
- Chylothorax: Dyspnoea, cough, chest discomfort; pleural effusion on CXR
Biochemical (Diagnostic)
| Test | Chyle Leak | Normal Drain |
|---|---|---|
| Triglycerides (TG) | >110 mg/dL AND > serum TG | <100 mg/dL |
| Appearance | Milky white | Serosanguinous |
| Cell count | >1,000/mL | - |
| Differential | Lymphocyte predominance >80% | - |
| LDH | Low | - |
| Cholesterol | <200 mg/dL | - |
- CXR: essential to rule out concurrent chylothorax when neck chyle leak identified
- Lymphangiography/lymphoscintigraphy: Localize the leak site for percutaneous embolization planning
Intraoperative Detection & Management
When chyle leak is suspected intraoperatively (especially during lower neck dissection):
- Ask anaesthesiologist to apply positive pressure ventilation - pools milky fluid or reveals discrete lymph vessels
- Meticulous ligation with non-absorbable sutures (silk)
- Adjuncts:
- Operating microscope for identification
- Fat grafting
- Surgicel (oxidised cellulose) application
- Sclerosing agents
Surgical trick to identify the leak: Give cream or olive oil via nasogastric tube before surgery - increases chyle drainage into the operative field, making the duct visible
Postoperative Management Algorithm
Classification by Output Volume
| Output | Category | Management |
|---|---|---|
| <500 mL/24h (low output) | Conservative | Non-operative management |
| 500-1000 mL/24h (moderate) | Watch & treat | Trial of conservative Rx 3-5 days; if no improvement → surgical |
| >1000 mL/24h (high output) | Surgical | Early intervention regardless of duration |
Conservative Management (Low-Output)
Step 1: Dietary Modification
- Medium-Chain Triglyceride (MCT) diet: MCTs (C6-C12 chain length) are absorbed directly into the portal circulation, bypassing the lymphatic system and reducing chyle flow
- Low-fat or fat-free diet with MCT supplementation
- Note: Long-chain TGs stimulate chyle flow - must be avoided
Step 2: Bowel Rest + Parenteral Nutrition
- NPO (nil per os) + Total Parenteral Nutrition (TPN): Eliminates enteral fat, maximally reduces lymphatic flow
- Most effective at reducing output
Step 3: Pharmacological Reduction of Chyle Flow
| Drug | Mechanism | Notes |
|---|---|---|
| Octreotide (somatostatin analogue) | Reduces splanchnic blood flow → decreases GI chyle production | Long-acting; subcutaneous injection; most evidence |
| Somatostatin | Same as octreotide | Short half-life; IV infusion |
| Etilefrine / Midodrine | Sympathomimetics; reduce lymphatic flow | Used in some centres |
| Orlistat | Pancreatic lipase inhibitor (OTC) | Reduces fat absorption; may be as effective as octreotide |
Step 4: Wound/Drainage Management
- Closed drainage promotes skin flap adherence
- Pressure dressings over neck (if cervical leak)
- Avoid prolonged continuous drainage (causes chyle loss, malnutrition, immunosuppression)
Interventional / Surgical Management (High-Output or Refractory)
1. Percutaneous Thoracic Duct Embolization (TDE)
- Lymphangiography identifies the site of leak
- Intranodal or pedal lymphangiography → opacifies the thoracic duct
- Percutaneous catheter embolization with coils/glue
- Success rate ~70-80% for post-surgical chylothorax
- Less invasive alternative to surgery; increasingly preferred
2. Surgical Thoracic Duct Ligation
- Approach: Via right chest (thoracotomy or VATS) - the thoracic duct is accessed as it enters the thorax through the diaphragmatic hiatus
- The classic technique ligates all tissue en masse between the aorta, esophagus, spine, and azygos vein (mass ligation)
- VATS (Video-Assisted Thoracoscopic Surgery) is the preferred minimally invasive approach
- Thoracic duct ligation for cervical chyle leak via neck wound re-exploration is also performed
3. Pleurodesis
- Chemical pleurodesis (talc, tetracycline) obliterates pleural space
- Used when definitive surgery is not possible
4. Pleuroperitoneal Shunt
- Refractory cases; relieves symptoms, minimises chyle loss, reduces TPN dependency
- Contraindicated if ascites present
- Risk: shunt occlusion (high fibrinogen in chyle)
5. Indwelling Pleural Catheter (IPC)
- Refractory cases not suitable for surgery
- Allows intermittent drainage at home
Fluid & Nutritional Replacement
Because chyle contains proteins, fat, fat-soluble vitamins, and T-lymphocytes:
- Albumin infusion for hypoalbuminaemia
- TPN to replace caloric and protein losses
- Immunoglobulin supplementation in prolonged leaks (lymphocyte depletion causes immunosuppression)
- Close monitoring of electrolytes
Summary Algorithm
Chyle Leak Diagnosed
|
├── Low output (<500 mL/day)
| → NPO + TPN + MCT diet + Octreotide
| → Pressure dressing / closed drain
| → Wait 2-4 weeks for spontaneous closure
|
├── Moderate (500-1000 mL/day)
| → Trial conservative Rx 3-5 days
| → If not improving → Intervention
|
└── High output (>1000 mL/day)
→ Early intervention
→ Lymphangiography + Percutaneous TDE (first line, if available)
→ If failed → Surgical TD ligation (VATS or open right thoracotomy)
→ Pleurodesis / pleuroperitoneal shunt for refractory cases
Key Viva Points
- Diagnostic fluid TG level: >110 mg/dL (some sources: >100 mg/dL) confirms chyle
- MCT rationale: Absorbed via portal vein, NOT lacteals - bypasses lymphatics
- Octreotide mechanism: Reduces splanchnic blood flow → less mesenteric lymph → less chyle
- Surgical approach for TD ligation: Right chest (not left) - thoracic duct enters from right via aortic hiatus
- Cream via NGT before surgery: Increases chyle flow to identify the leaking duct intraoperatively
- Most common cause of chylothorax in neonate: Congenital (commonest cause of neonatal pleural effusion)
- Most common non-traumatic cause in adults: Lymphoma
Sources: Cummings Otolaryngology Head and Neck Surgery, Chapter 119; Sabiston Textbook of Surgery, Chapter 110; Fischer's Mastery of Surgery 8e; Murray & Nadel's Textbook of Respiratory Medicine, Chapter 111; Mulholland and Greenfield's Surgery 7e
This is a shared conversation. Sign in to Orris to start your own chat.