APPENDICITIS
Reading File
Finding Sources
Searching PubMed
"appendicitis"[MeSH Terms] AND ("diagnosis" OR "management")
Searching Images
appendicitis anatomy pathology CT scan
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I have excellent comprehensive coverage. Let me now compile the full, well-organized response on appendicitis.
APPENDICITIS
Overview & Epidemiology
Appendicitis is the most common intra-abdominal surgical emergency, affecting ~1 per 1,000 adults annually worldwide. Lifetime risk is 7–10% (8.7% men, 6.9% women). In the United States, ~400,000 cases are diagnosed per year, with 16–40% presenting with perforation. Peak incidence is ages 9–12 years; it is uncommon under age 5 but carries the highest perforation rate in that group (>50% ruptured at surgery).
- Current Surgical Therapy 14e | Goldman-Cecil Medicine | Rosen's Emergency Medicine
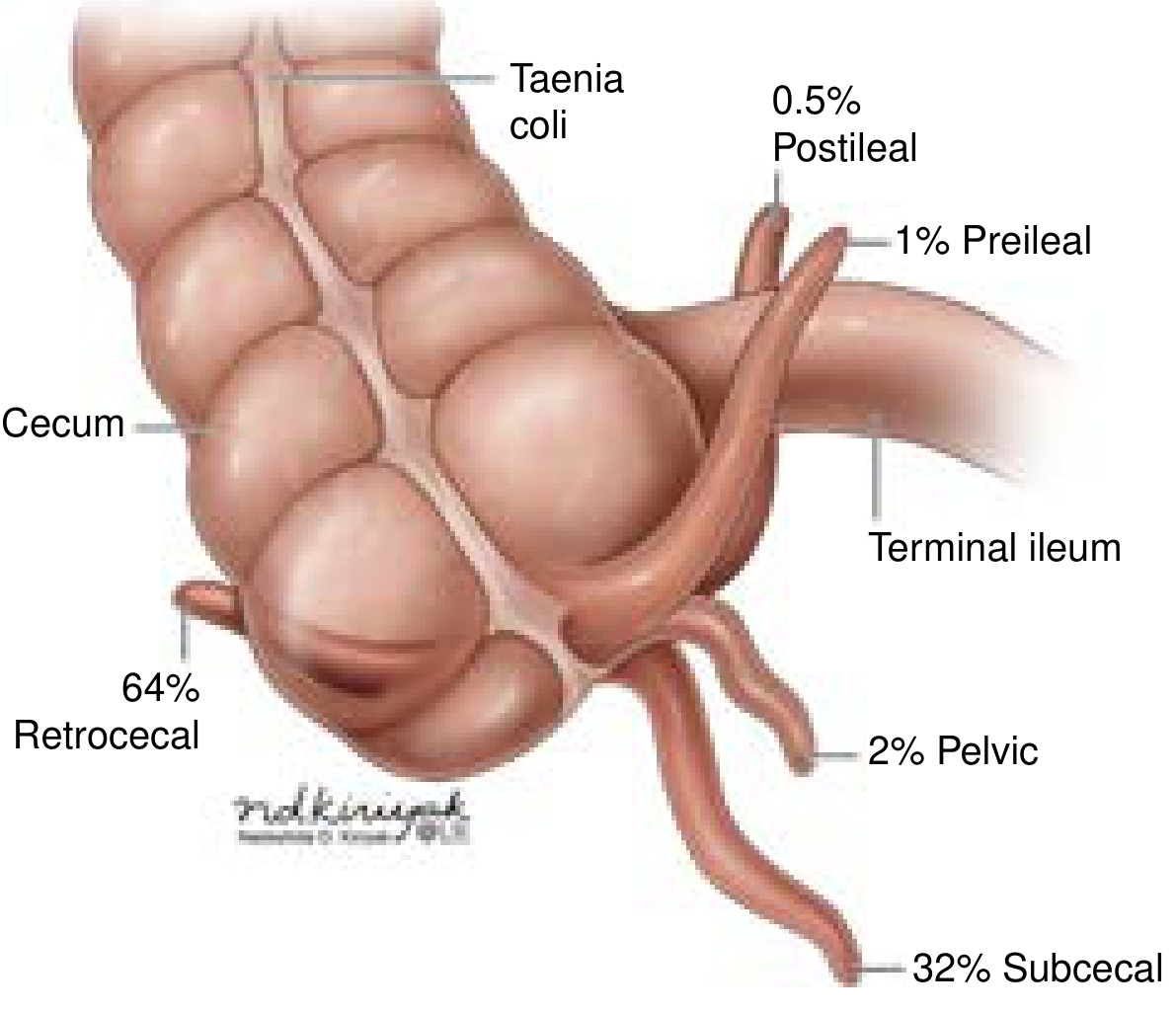
Anatomy
The appendix is an ~9 cm long, 0.6 cm wide vermiform ("worm-shaped") hollow structure arising from the terminal cecum, at the convergence of the three taenia coli. While the base is consistently cecal, the tip position varies widely:
- Retrocecal (most common, ~65%)
- Pelvic / subcecal
- Pre-ileal / post-ileal
This positional variability explains the diversity of clinical presentations. Blood supply: appendiceal artery, a branch of the ileocolic artery (branch of superior mesenteric artery).
Pathophysiology
The central mechanism is luminal obstruction → bacterial overgrowth → progressive ischemia → perforation.
Causes of obstruction:
| Cause | Notes |
|---|---|
| Fecalith / appendicolith | Most common |
| Lymphoid hyperplasia | Common in children (viral infections) |
| Neoplasm | Carcinoid, mucocele |
| Parasites | Enterobius, Ascaris |
| Foreign body | Less common |
Sequence of events:
- Obstruction → increased intraluminal pressure
- Mucus accumulation, bacterial overgrowth (E. coli, B. fragilis, Klebsiella, Streptococcus, Enterococcus, Pseudomonas)
- Venous congestion → distension → visceral pain (periumbilical)
- Arterial ischemia → necrosis → gangrene
- Perforation → local abscess or diffuse peritonitis
Children have thinner appendiceal walls and underdeveloped omentum → perforation occurs earlier and diffuse peritonitis develops more readily.
- Current Surgical Therapy 14e
Clinical Features
Classic Presentation
- Anorexia (often earliest symptom)
- Nausea and vomiting
- Periumbilical pain initially (visceral, colicky) → migrates to RLQ (McBurney's point) within hours as parietal peritoneum becomes involved
- Low-grade fever (develops later; high fever suggests perforation/abscess)
- Progressive worsening over 24–72 hours
McBurney's point: two-thirds of the distance from the umbilicus to the right anterosuperior iliac spine.
Physical Examination Signs
| Sign | How to Elicit | Significance |
|---|---|---|
| McBurney's tenderness | Direct palpation at McBurney's point | Most reliable |
| Rovsing's sign | Palpation of LLQ causes RLQ pain | Peritoneal irritation |
| Psoas sign | Pain with extension of right hip (patient prone) or flexion against resistance | Retrocecal appendix |
| Obturator sign | Pain with internal rotation of flexed right hip | Pelvic appendix |
| Dunphy's sign | Increased RLQ pain with coughing | Peritonitis |
| Heel-tap sign | RLQ pain when patient drops from tiptoes | Peritoneal irritation |
| Rebound tenderness | Sudden release of pressure causes pain | Peritoneal irritation |
| Guarding / rigidity | Involuntary muscle spasm | Peritonitis |
Important caveats: Rovsing, psoas, and obturator signs have poor sensitivity/specificity, especially in young children. Classic signs may be absent in retrocecal appendicitis, elderly patients, immunosuppressed patients, and pregnant women.
- Rosen's Emergency Medicine | Textbook of Family Medicine 9e
Differential Diagnosis
Surgical causes: Intestinal obstruction, intussusception, acute cholecystitis, Meckel's diverticulitis, mesenteric adenitis, ovarian torsion, ectopic pregnancy
Gynecological: Pelvic inflammatory disease, ovarian cyst (ruptured/torsion), endometriosis, mittelschmerz
Medical/other: Urinary tract infection, right ureteral stone, psoas abscess, right-sided pneumonia, Crohn's disease, gastroenteritis, constipation
- Goldman-Cecil Medicine, Table 128-1
Diagnostic Workup
Laboratory Tests
No single test is diagnostic. Typical findings:
- WBC >10,000/μL (in 87–92% of cases) but <18,000/μL unless perforation has occurred; left shift
- CRP elevated (>0.6 mg/dL sensitive; highly elevated suggests perforation/abscess)
- Procalcitonin: elevated with complicated appendicitis
- Urinalysis: mild sterile pyuria (<5–10 WBC/hpf) possible due to ureteral inflammation; does not exclude appendicitis
- β-hCG: mandatory in women of reproductive age to exclude ectopic pregnancy
Clinical Scoring Systems
Alvarado Score (MANTRELS):
| Feature | Points |
|---|---|
| Migration of pain to RLQ | 1 |
| Anorexia | 1 |
| Nausea/vomiting | 1 |
| RLQ tenderness | 2 |
| Rebound tenderness | 1 |
| Elevated temperature (>37.3°C) | 1 |
| Leukocytosis (WBC >10,000) | 2 |
| Left shift | 1 |
| Total | 10 |
Interpretation: ≤4 = unlikely; 5–6 = possible; 7–8 = probable; 9–10 = very likely.
Other validated systems: Pediatric Appendicitis Score (PAS), Adult Appendicitis Score, Appendicitis Inflammatory Response (AIR) score.
Imaging
| Modality | Sensitivity | Specificity | Notes |
|---|---|---|---|
| CT (multidetector, low-dose) | ≥94% | ≥94% | Preferred in adults and obese patients; can detect perforation and complications |
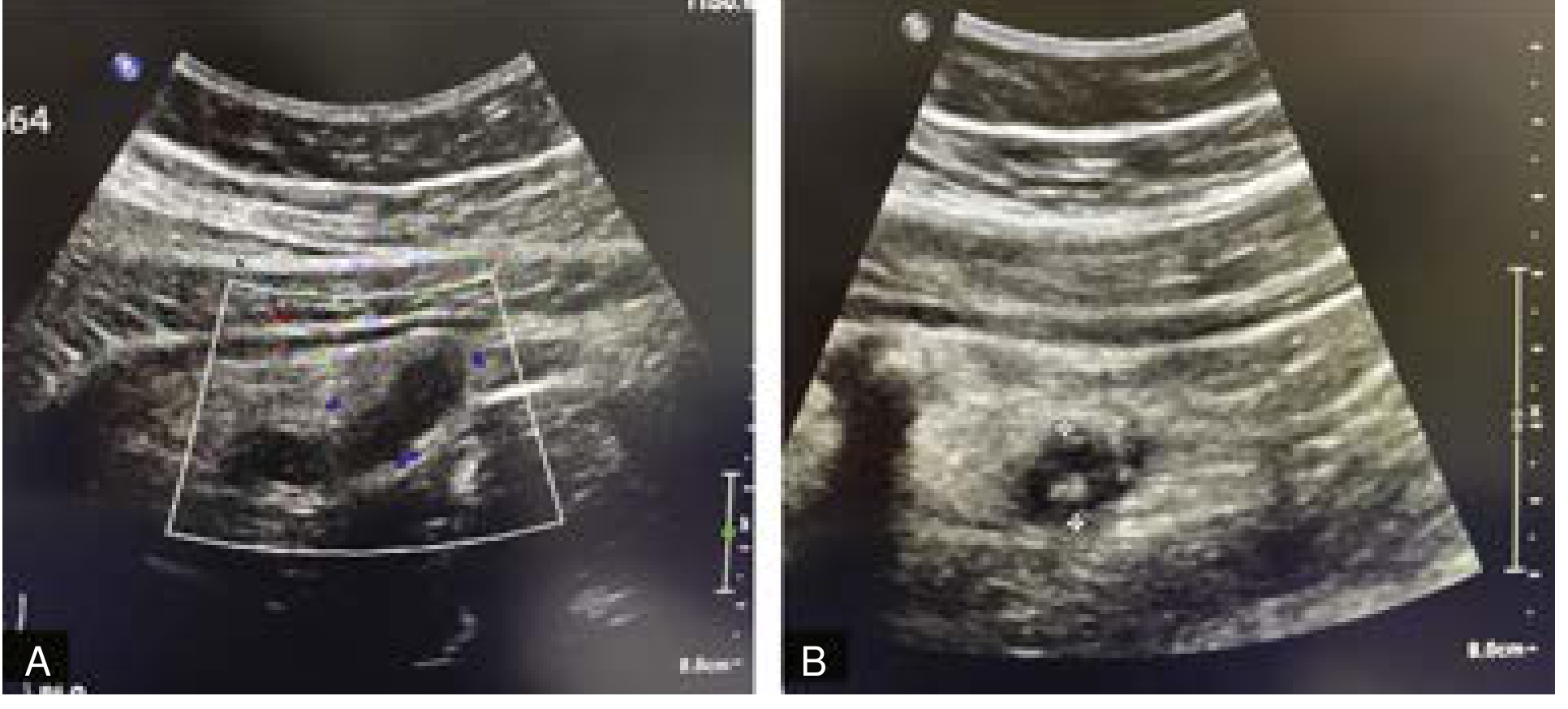
| Ultrasound | ~83% | ~93% | First-line in children and pregnant women; non-compressible appendix >6 mm is diagnostic; operator-dependent |
| MRI | Comparable to CT | Comparable to CT | Preferred in pregnancy (avoids radiation); good alternative |
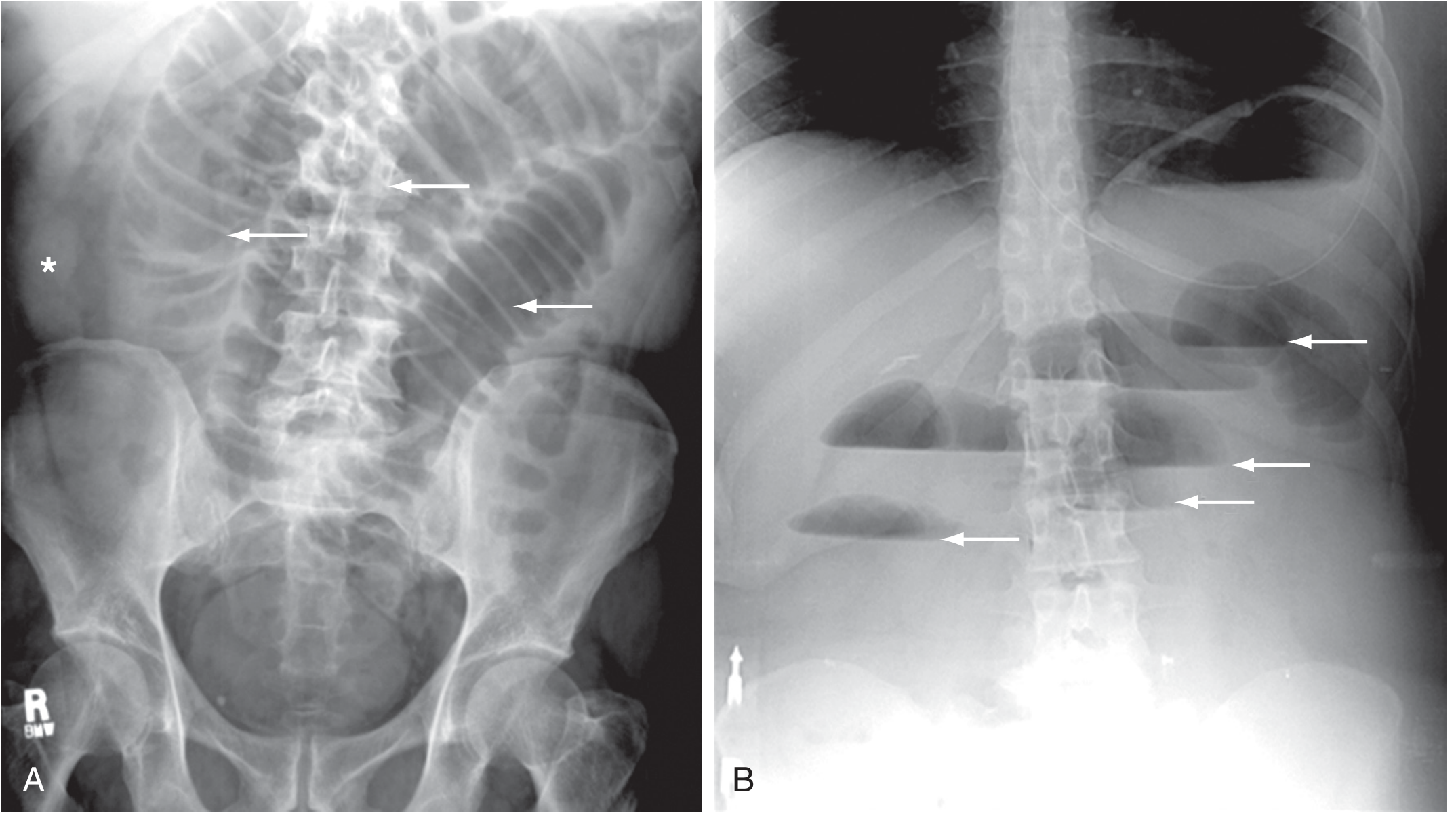
| Plain X-ray | Low | Low | Not diagnostic; may show appendicolith, ileus, RLQ soft tissue density |
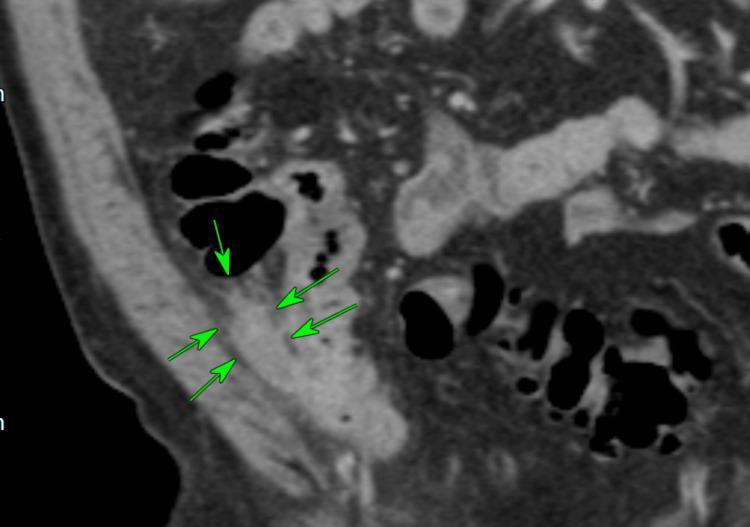
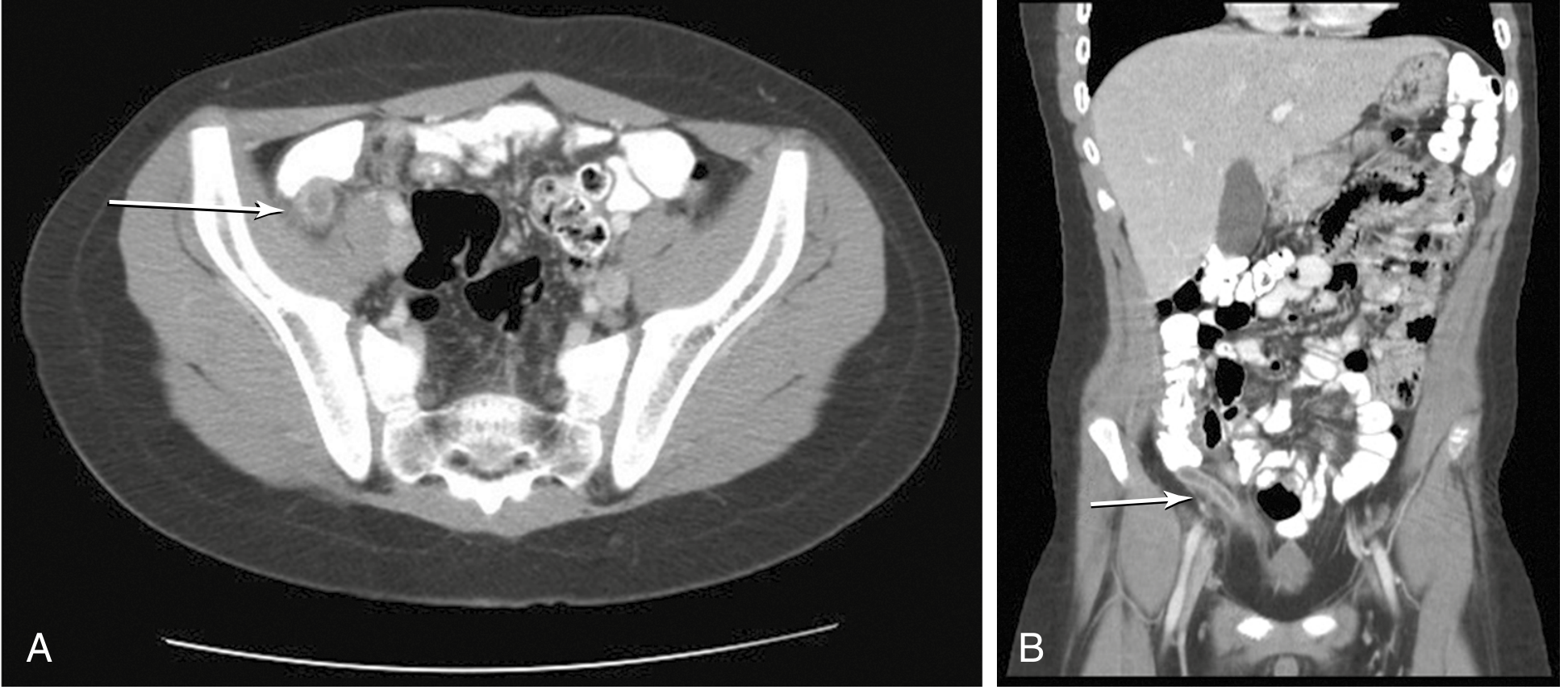
CT findings in appendicitis:
- Dilated appendix >6 mm diameter
- Appendiceal wall thickening and enhancement
- Periappendiceal fat stranding
- Appendicolith (seen in ~30%)
- Periappendiceal abscess (with perforation)

- Goldman-Cecil Medicine | Current Surgical Therapy 14e | Rosen's Emergency Medicine
Classification
| Type | Features |
|---|---|
| Simple (uncomplicated) | Inflamed but intact; no necrosis, perforation, or abscess |
| Gangrenous | Necrosis of appendiceal wall; almost always associated with luminal obstruction |
| Perforated | Full-thickness rupture; risk of peritonitis or abscess |
| Phlegmon / Abscess | Walled-off perforation; mass palpable in RLQ |
Management
Preoperative
- IV fluids and electrolyte correction
- NPO
- Preoperative antibiotics (reduce infectious complications in uncomplicated disease):
- Cefotetan 2 g IV, or Cefoxitin 2 g IV (3 postoperative doses for uncomplicated disease)
- Piperacillin-tazobactam or ticarcillin-clavulanic acid for complicated/perforated
- Target: E. coli, Bacteroides (gram-negative aerobes + anaerobes)
Operative Management
Laparoscopic appendectomy is now the standard of care for most cases:
- Lower rate of postoperative complications vs. open
- Faster return to normal activity and diet
- Appropriate for: uncomplicated and most complicated appendicitis
Open appendectomy (McBurney's / Gridiron incision):
- Preferred when perforation is evident preoperatively
- McBurney's incision: oblique through McBurney's point; muscle-splitting (gridiron)
- Remains essential skill for surgeons
Interval appendectomy: For patients who present with phlegmon/abscess after >5 days of symptoms → nonoperative management first (IV antibiotics ± percutaneous drainage by interventional radiology), followed by interval appendectomy at 6–8 weeks.
Nonoperative (Antibiotic-Only) Management
Growing evidence supports antibiotics alone for uncomplicated appendicitis:
-
~80–90% symptom resolution within 24–48 hours
-
2025 WSES Jerusalem Guidelines and 2024 SAGES Guidelines acknowledge this as a viable alternative
-
Recurrence rate ~25–40% at 5 years (higher in children)
-
Contraindicated if: fecalith/appendicolith present, perforation, immunocompromised, unable to comply with follow-up
-
Most surgeons still prefer operative management as definitive treatment
-
Current Surgical Therapy 14e | Goldman-Cecil Medicine | SAGES 2024 [PMID: 38740595] | WSES 2025 [PMID: 41604201]
Complications
| Complication | Features |
|---|---|
| Perforation | Increases mortality 0.0002% → 3%; morbidity 3% → 47% |
| Peritonitis | Diffuse or localized; requires broad-spectrum antibiotics + surgery |
| Periappendiceal abscess | Walled-off perforation; drain percutaneously if accessible |
| Wound infection | More common after open or contaminated surgery |
| Ileus / adhesions | Post-surgical bowel obstruction |
| Pylephlebitis | Septic portal vein thrombosis (rare but serious) |
| Stump appendicitis | Inflammation of residual appendiceal stump after appendectomy |
Special Populations
Children
- Perforation rate inversely correlates with age; >50% perforation rate in children <5 years
- US and MRI preferred (avoid radiation)
- Nonoperative management acceptable in select cases; recurrence up to 40%
- Same-day discharge possible after laparoscopic appendectomy in early disease
Pregnancy
- Most common surgical emergency in pregnancy (same incidence as non-pregnant)
- Diagnosis challenging: displaced appendix (tip moves to RUQ by third trimester in <25% of cases), physiologic leukocytosis and elevated ESR
- MRI preferred imaging (avoids fetal radiation)
- Perforation → increased risk of sepsis, fetal mortality, preterm labor
- Laparoscopic appendectomy safe throughout all trimesters
Elderly
- Atypical presentation common; diagnosis often delayed
- Higher perforation rate at presentation (~70%)
- Higher mortality and morbidity
Prognosis
- Uncomplicated appendicitis: mortality ~0.0002%; full recovery expected
- Perforated appendicitis: mortality ~3%; morbidity ~47%
- Laparoscopic vs. open: laparoscopic carries lower wound infection rate, shorter hospital stay
Recent Guidelines (2024–2025)
| Guideline | Key Recommendation |
|---|---|
| SAGES 2024 [PMID: 38740595] | Laparoscopic appendectomy preferred; antibiotics-first is a valid option for uncomplicated disease in selected patients |
| WSES Jerusalem Guidelines 2025 [PMID: 41604201] | Updated diagnostic and management algorithms; CT preferred for adults; nonoperative management supported for uncomplicated, fecalith-free appendicitis |
Sources: Current Surgical Therapy 14e | Rosen's Emergency Medicine | Goldman-Cecil Medicine | Textbook of Family Medicine 9e | Gray's Anatomy for Students | SAGES 2024 [PMID 38740595] | WSES 2025 [PMID 41604201]
Definition Etiology Pathophysiology ( chart form) Clinical features Types Diagnosis/ investigation Management ( table form) Medical management Surgical management Algorithm to approach appendicitis (chart form) with arrow Of appendicitis
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
I now have all the content needed. Let me compile the comprehensive, structured response exactly as requested.
APPENDICITIS — Structured Clinical Reference
1. DEFINITION
Appendicitis is an acute inflammation of the vermiform appendix — a blind-ended tubular structure arising from the cecum — resulting from luminal obstruction, bacterial overgrowth, and progressive ischemic injury to the appendiceal wall.
It is the most common intra-abdominal surgical emergency worldwide, responsible for ~300,000–400,000 hospitalizations annually in the United States, with a lifetime risk of 6–10% in the general population.
Sabiston Textbook of Surgery | Goldman-Cecil Medicine
2. ETIOLOGY
Primary Cause: Luminal Obstruction
| Cause | Details |
|---|---|
| Fecalith / Appendicolith | Most common; hardened stool or calcified concretion; ~1/3 of cases |
| Lymphoid hyperplasia | Common in children/adolescents following viral infections (adenovirus, EBV) |
| Neoplasms | Carcinoid tumor, mucinous adenocarcinoma, carcinoma |
| Parasites | Enterobius vermicularis (pinworm), Ascaris lumbricoides |
| Foreign body | Ingested material, vegetable seeds, barium |
| Fecal stasis | Low-fiber, high-fat (Western) diet implicated epidemiologically |
| Stricture / adhesion | Post-inflammatory scarring |
Bacteriology (polymicrobial)
- Escherichia coli
- Bacteroides fragilis
- Klebsiella pneumoniae
- Enterococcus spp.
- Pseudomonas aeruginosa
- Streptococcus spp.
Sabiston Textbook of Surgery | Current Surgical Therapy 14e
3. PATHOPHYSIOLOGY (Flow Chart)
LUMINAL OBSTRUCTION
(fecalith, lymphoid hyperplasia, neoplasm, parasite)
│
▼
INCREASED INTRALUMINAL PRESSURE
(mucus secretion + bacterial gas production continue)
│
▼
VENOUS CONGESTION & LYMPHATIC OBSTRUCTION
(visceral afferent nerve fibers stretched)
│
▼
VAGUE PERIUMBILICAL / EPIGASTRIC PAIN
(T10 dermatome, colicky, visceral)
│
▼
BACTERIAL OVERGROWTH & MUCOSAL ISCHEMIA
(E. coli, B. fragilis, Klebsiella, Pseudomonas)
│
▼
TRANSMURAL INFLAMMATION
(appendiceal wall becomes full-thickness inflamed)
│
▼
PARIETAL PERITONEUM INVOLVED
│
▼
LOCALIZED SOMATIC PAIN → RLQ (McBurney's point)
+ Fever, guarding, rigidity
│
▼
┌───────┴────────┐
▼ ▼
UNCOMPLICATED ARTERIAL ISCHEMIA
APPENDICITIS → FULL-THICKNESS NECROSIS
(inflamed but (Gangrenous appendicitis)
intact) │
▼
PERFORATION
┌──────┴──────┐
▼ ▼
LOCALIZED FREE PERFORATION
ABSCESS / (Diffuse peritonitis,
PHLEGMON sepsis, death)
Sabiston Textbook of Surgery | Current Surgical Therapy 14e
4. CLINICAL FEATURES
Symptoms
| Symptom | Description |
|---|---|
| Anorexia | Earliest and most consistent symptom |
| Periumbilical pain | Initial visceral pain — vague, colicky |
| Migration of pain to RLQ | Hallmark; occurs over 12–24 h as parietal peritoneum becomes involved |
| Nausea & vomiting | Usually follows pain onset |
| Low-grade fever | 37.5–38.5°C; high fever (>39°C) suggests perforation |
| Constipation / diarrhea | Variable; tenesmus possible with pelvic appendix |
Signs
| Sign | Method | Significance |
|---|---|---|
| McBurney's tenderness | Direct palpation 2/3 from umbilicus to ASIS | Most reliable RLQ finding |
| Guarding / rigidity | Involuntary abdominal wall spasm | Peritoneal irritation |
| Rebound tenderness (Blumberg's) | Sudden release of deep pressure → pain | Peritonitis |
| Rovsing's sign | LLQ palpation → RLQ pain | Refers peritoneal irritation |
| Psoas sign | Pain on right hip extension (patient prone) or active flexion against resistance | Retrocecal appendix |
| Obturator sign | Pain with internal rotation of flexed right hip | Pelvic appendix |
| Dunphy's (cough) sign | RLQ pain increased by coughing | Peritonitis |
| Heel-drop test | Patient drops from tiptoes → RLQ pain | Peritoneal irritation |
| Rigidity / Board-like abdomen | Involuntary muscle guarding | Perforated / diffuse peritonitis |
Rosen's Emergency Medicine | Textbook of Family Medicine 9e | Sabiston Textbook of Surgery
5. TYPES / CLASSIFICATION
By Acuity
| Type | Features |
|---|---|
| Acute appendicitis | Evolves over hours to days; most common presentation |
| Chronic / Recurrent appendicitis | Symptoms spanning weeks to months; low-grade, intermittent pain |
By Severity (most clinically important)
| Type | Pathology | Key Features |
|---|---|---|
| Simple (Uncomplicated) | Inflamed appendix, wall intact, no necrosis | RLQ pain, fever, leukocytosis; no perforation |
| Gangrenous | Full-thickness wall necrosis | More severe pain; almost always associated with fecalith; pre-perforation state |
| Perforated | Transmural rupture | High fever, peritonism, sepsis; two subtypes below |
| Appendiceal Phlegmon | Contained inflammatory mass | Palpable RLQ mass; present after ≥5 days of symptoms |
| Periappendiceal Abscess | Walled-off pus collection | Mass, swinging fever; amenable to percutaneous drainage |
| Diffuse Peritonitis | Free perforation, peritoneal soilage | Generalized rigidity, sepsis, high mortality |
Sabiston Textbook of Surgery | Current Surgical Therapy 14e
6. DIAGNOSIS / INVESTIGATIONS
Clinical Scoring: Alvarado Score (MANTRELS)
| Feature | Score |
|---|---|
| Migration of pain to RLQ | 1 |
| Anorexia | 1 |
| Nausea / vomiting | 1 |
| Tenderness in RLQ | 2 |
| Rebound tenderness | 1 |
| Elevated temperature (>37.3°C) | 1 |
| Leukocytosis (WBC >10,000) | 2 |
| Shift to left (neutrophilia) | 1 |
| Total | 10 |
Interpretation: ≤4 = Appendicitis unlikely | 5–6 = Possible | 7–8 = Probable | 9–10 = Highly likely
Other scores: Pediatric Appendicitis Score (PAS), Appendicitis Inflammatory Response (AIR) Score, Adult Appendicitis Score
Laboratory Investigations
| Test | Expected Finding | Notes |
|---|---|---|
| WBC count | >10,000/μL; usually <18,000 | Elevated in 87–92%; left shift (neutrophilia) |
| CRP | Elevated (>0.6 mg/dL) | Highly elevated → perforation/abscess |
| Procalcitonin | Elevated | Indicates complicated/perforated disease |
| Urinalysis | Mild sterile pyuria possible | ≤5–10 WBC/hpf; bacteria absent; from ureteral irritation |
| β-hCG (serum/urine) | Negative | Mandatory in all women of reproductive age |
| Blood cultures | Positive in sepsis | Needed if systemic infection suspected |
| Electrolytes / BMP | Disturbances with vomiting | Baseline for surgical planning |
| LFTs / Lipase | Normal (helps exclude biliary/pancreatic) | Part of differential workup |
Imaging Investigations
| Modality | Sensitivity | Specificity | When to Use |
|---|---|---|---|
| CT Abdomen/Pelvis (MDCT) | ≥94% | ≥94% | Gold standard in adults; low-dose (2 mSv); detects perforation, abscess, alternative diagnoses |
| Ultrasound (RLQ) | ~83% | ~93% | First-line in children and pregnant women; non-compressible appendix >6 mm diagnostic; operator-dependent |
| MRI Abdomen | ~95% | ~95% | Preferred in pregnancy (no radiation); safe, accurate |
| Plain X-ray (AXR) | Low | Low | Not routinely used; may show appendicolith, air-fluid levels, RLQ soft tissue density |
CT Diagnostic Criteria:
- Appendix diameter >6 mm
- Appendiceal wall thickening + enhancement
- Periappendiceal fat stranding
- Appendicolith (30% of cases)
- Periappendiceal fluid / abscess (with perforation)
- "Target sign": thickened, fluid-filled appendix (sagittal view)
Goldman-Cecil Medicine | Sabiston Textbook of Surgery | Current Surgical Therapy 14e
7. MANAGEMENT (Table Form)
Overview by Type
| Type of Appendicitis | Management Strategy |
|---|---|
| Uncomplicated (simple) | Laparoscopic appendectomy OR antibiotics-first (shared decision making) |
| Gangrenous | Laparoscopic appendectomy (urgent) |
| Perforated with diffuse peritonitis | Emergency open or laparoscopic appendectomy + peritoneal lavage |
| Perforated with abscess (<5 days) | Laparoscopic appendectomy + drainage |
| Phlegmon / Abscess (>5 days symptoms) | Nonoperative: IV antibiotics ± percutaneous drain → Interval appendectomy 6–8 weeks |
| Chronic/recurrent | Elective laparoscopic appendectomy |
A. MEDICAL MANAGEMENT
| Component | Details |
|---|---|
| IV Fluid Resuscitation | Normal saline or Lactated Ringer's to correct dehydration and electrolyte imbalances |
| NPO | Nothing by mouth in anticipation of surgery or while monitoring |
| Analgesia | IV opioids (morphine, fentanyl) — does NOT mask diagnosis; provide adequate pain relief |
| Antiemetics | Ondansetron, metoclopramide for nausea/vomiting |
| Antipyretics | Paracetamol / NSAIDs for fever management |
| Preoperative antibiotics | Single dose within 60 min of incision (reduces surgical site infections) |
Antibiotic Regimens
| Setting | First-Line | Alternatives |
|---|---|---|
| Uncomplicated (prophylaxis) | Cefotetan 2 g IV OR Cefoxitin 2 g IV | Cefazolin + metronidazole |
| Complicated / Perforated | Piperacillin-tazobactam 3.375 g IV q6h | Ticarcillin-clavulanate; Meropenem (severe) |
| Antibiotics-only (nonoperative) | Ertapenem 1 g IV daily OR Ceftriaxone + metronidazole | Amoxicillin-clavulanate (oral step-down) |
| Penicillin allergy | Ciprofloxacin + metronidazole | Aztreonam + metronidazole |
Duration:
- Uncomplicated: single preoperative dose (3 doses post-op max)
- Complicated/perforated: 3–5 days IV then consider oral step-down based on clinical response
- Nonoperative (antibiotics-only): 7–10 days (IV 24–48 h → oral)
Nonoperative (Antibiotics-Only) — Indications & Criteria
| Factor | Suitable for Nonoperative | NOT Suitable |
|---|---|---|
| Appendicolith | No | Yes (higher failure/complication rate) |
| Imaging | Uncomplicated, no abscess | Perforation, free air, abscess |
| Age | Adults, select pediatric | Very young children |
| Recurrence risk | Counseled (~25–40% at 5 years) | Refused by patient |
| Comorbidities | Low surgical risk prefers nonop | High surgical risk |
Sabiston Textbook of Surgery (CODA trial, APPAC trial) | Current Surgical Therapy 14e
B. SURGICAL MANAGEMENT
Laparoscopic Appendectomy (Standard of Care)
| Step | Details |
|---|---|
| Position | Supine; left arm tucked; possible reverse Trendelenburg + right side up |
| Access | Veress needle (closed) or Hasson technique (open) through umbilicus |
| Insufflation | CO₂ to 12–15 mmHg |
| Port placement | Umbilical camera port (10–12 mm) + 2 working ports (5 mm) in LLQ / suprapubic |
| Procedure | Identify cecum → follow taenia coli to appendix base → divide mesoappendix (stapler/LigaSure) → staple/ligate appendix base → place in retrieval bag → remove |
| Irrigation | Pelvic irrigation if contamination present; consider cultures |
| Advantages | Lower wound infection rate, faster recovery, shorter hospital stay, diagnostic capability |
Open Appendectomy
| Step | Details |
|---|---|
| Incision | McBurney's (gridiron): oblique muscle-splitting incision at McBurney's point |
| Alternative | Lanz (transverse) incision for better cosmesis |
| Preferred when | Perforation with peritonitis; technical failure of laparoscopy; laparoscopy unavailable |
| Technique | Identify cecum → mesoappendix ligated and divided → appendix base doubly ligated → appendix excised → stump inverted (optional) |
Interval Appendectomy
| Indication | Timing | Route |
|---|---|---|
| Phlegmon or abscess (>5 days) managed nonoperatively | 6–8 weeks after resolution | Elective laparoscopic |
Percutaneous Drainage (IR-guided)
- For periappendiceal abscess amenable to drainage
- Performed by interventional radiology
- Followed by interval appendectomy at 6–8 weeks
- Not appropriate if no safe window, peritonitis, or free perforation
Sabiston Textbook of Surgery | Current Surgical Therapy 14e | Goldman-Cecil Medicine
8. ALGORITHM TO APPROACH APPENDICITIS
PATIENT PRESENTS WITH ACUTE ABDOMINAL PAIN
│
▼
HISTORY & PHYSICAL EXAMINATION
(Pain migration, anorexia, RLQ tenderness,
fever, guarding, Rovsing/Psoas/Obturator signs)
│
▼
CALCULATE ALVARADO SCORE
┌──────────┼──────────┐
▼ ▼ ▼
SCORE ≤4 SCORE 5–6 SCORE ≥7
(Unlikely) (Equivocal) (Probable)
│ │ │
▼ │ ▼
Consider IMAGING LABS + IMAGING
Alternatives │ (CBC, CRP, PCT)
Discharge if ┌────┴─────┐ │
well │ │ │
ULTRASOUND CT CT ABDOMEN
(children, (adults, /PELVIS
pregnant) obese)
│
┌───────┴────────┐
▼ ▼
CT NEGATIVE CT POSITIVE
(Appendix normal) (Appendicitis confirmed)
│ │
▼ ▼
Observe / Admit DETERMINE TYPE
Re-evaluate │
Consider alt Dx ┌────────┴─────────┐
▼ ▼
UNCOMPLICATED COMPLICATED
(No perforation, (Perforation / Abscess /
no gangrene) Phlegmon / Peritonitis)
│ │
┌─────────┴──────┐ ┌──────┴──────┐
▼ ▼ ▼ ▼
APPENDECTOMY ANTIBIOTICS DURATION FREE
(Laparoscopic, -ONLY OF Sx <5d PERFORATION
Gold standard) (selected, Appendectomy /PERITONITIS
│ no fecalith) ± Drainage │
▼ │ │ ▼
PREOP ABX Ertapenem DURATION Sx ≥5d EMERGENCY
+ Resuscitation IV 24–48h ┌────────────┐ OPEN / LAP
│ → Oral 7–10d │ IV ABX + │ APPENDECTOMY
▼ │ │Percutaneous│ + LAVAGE
SURGERY MONITOR │ Drainage │
│ (Failure? │ │
▼ → Surgery)└────────────┘
POST-OP CARE │
(Uncomplicated: ▼
same-day/next-day INTERVAL APPENDECTOMY
discharge; at 6–8 WEEKS
Complicated:
IV ABX 3–5 days)
Sources: Sabiston Textbook of Surgery | Current Surgical Therapy 14e | Rosen's Emergency Medicine | Goldman-Cecil Medicine | Textbook of Family Medicine 9e | SAGES Guidelines 2024 [PMID 38740595] | WSES Jerusalem Guidelines 2025 [PMID 41604201]
Describe causes, ETIOPATHOGENESIS (chart)clinical features and treatment (medical and surgical? management) algorithm chart of chronic intestinal obstruction(
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from multiple authoritative sources. Let me compile the full structured response.
CHRONIC INTESTINAL OBSTRUCTION — Complete Clinical Reference
1. DEFINITION
Chronic intestinal obstruction refers to a long-standing, persistent or recurrent partial or complete impairment of the normal aboral progression of intestinal contents, lasting weeks to months, resulting from either a fixed mechanical narrowing of the bowel lumen or a chronic failure of intestinal neuromuscular motility (pseudo-obstruction).
It is distinguished from acute obstruction by:
- Gradual, insidious onset
- Prolonged, often intermittent symptoms
- Partial rather than complete obstruction in most mechanical cases
- Less immediate risk of strangulation (except in volvulus)
Two major categories exist:
- Chronic mechanical intestinal obstruction — fixed anatomical narrowing
- Chronic intestinal pseudo-obstruction (CIPO) — functional dysmotility with no obstructing lesion
Sleisenger & Fordtran's GI and Liver Disease | Schwartz's Principles of Surgery
2. CAUSES
A. Mechanical Causes (Intrinsic, Extrinsic, Intraluminal)
| Category | Cause | Example |
|---|---|---|
| Intraluminal | Tumour / neoplasm | Colorectal carcinoma, carcinoid |
| Impacted feces / bezoar | Fecal impaction | |
| Gallstone (gallstone ileus) | Erodes into bowel via cholecystoenteric fistula | |
| Foreign body | Ingested material | |
| Intramural | Carcinoma of colon / small bowel | Annular "apple-core" lesion |
| Crohn's disease | Stricture formation | |
| Radiation enteritis / stricture | Post-radiotherapy fibrosis | |
| Diverticular disease | Stricture of sigmoid colon | |
| Ischaemic stricture | After mesenteric ischaemia | |
| Tuberculosis (TB) of bowel | Ileocaecal involvement | |
| Endometriosis | Cyclic bowel involvement | |
| Intussusception (chronic) | Lead point tumour | |
| Extrinsic | Adhesions / bands | Post-surgical (most common overall) |
| Hernia | Inguinal, femoral, incisional — partially obstructing | |
| Pelvic/abdominal malignancy | Ovarian, pancreatic, gastric metastases | |
| Peritoneal carcinomatosis | Multifocal obstruction | |
| Mesenteric tumour | Desmoid, lymphoma | |
| Volvulus (subacute) | Sigmoid volvulus |
B. Functional / Pseudo-obstruction Causes (CIPO)
| Category | Cause |
|---|---|
| Primary (idiopathic) | Sporadic visceral myopathy or neuropathy (most common in adults) |
| Familial | Familial visceral myopathy (Types I–III); visceral neuropathy; X-linked (FLNA mutation) |
| Connective tissue disease | Scleroderma (PSS) — most common secondary cause; SLE; dermatomyositis |
| Neurological | Parkinson's disease; spinal cord injury; Chagas disease (T. cruzi destroys myenteric plexus) |
| Endocrine / Metabolic | Hypothyroidism (myxedema); Diabetes mellitus (autonomic neuropathy); hypoparathyroidism (hypocalcaemia) |
| Muscular dystrophy | Myotonic dystrophy; Duchenne muscular dystrophy |
| Amyloidosis | Infiltration of enteric nerves + smooth muscle |
| Paraneoplastic | Small-cell lung cancer → IgG anti-neuronal antibodies → myenteric plexus destruction |
| Drugs | Opioids, tricyclic antidepressants, phenothiazines, anticholinergics, antipsychotics |
| Radiation | Radiation enteritis causing dysmotility |
| Viral | Neurotropic viruses (EBV, CMV, HSV) |
| Mitochondrial disease | MNGIE syndrome (thymidine phosphorylase deficiency) |
Sleisenger & Fordtran | Schwartz's Principles of Surgery | Current Surgical Therapy 14e
3. ETIOPATHOGENESIS (Chart Form)
┌──────────────────────────────────────────────────────────────────────────┐
│ CHRONIC INTESTINAL OBSTRUCTION │
│ │
│ MECHANICAL CAUSE FUNCTIONAL CAUSE (CIPO) │
│ (fixed narrowing) (no obstructing lesion) │
└──────────┬───────────────────────────────┬──────────────────────────────┘
│ │
▼ ▼
┌──────────────────────┐ ┌───────────────────────────────────────┐
│ LUMINAL NARROWING │ │ NEUROMUSCULAR DYSFUNCTION │
│ (intraluminal / │ │ ┌────────────────────────────────┐ │
│ intramural / │ │ │ NEUROPATHIC: │ │
│ extrinsic) │ │ │ Degeneration / inflammation of │ │
└──────────┬───────────┘ │ │ myenteric (Auerbach) / Meissner│ │
│ │ │ plexus → uncoordinated or │ │
▼ │ │ absent peristaltic contractions│ │
PARTIAL OCCLUSION │ └────────────────────────────────┘ │
of intestinal lumen │ ┌────────────────────────────────┐ │
│ │ │ MYOPATHIC: │ │
▼ │ │ Smooth muscle atrophy / │ │
PROXIMAL DISTENSION │ │ fibrosis / replacement by │ │
(gas + fluid │ │ collagen → weak, absent │ │
accumulation) │ │ contractions │ │
│ │ └────────────────────────────────┘ │
▼ │ ┌────────────────────────────────┐ │
┌────────┴──────────┐ │ │ MESENCHYMOPATHY: │ │
│ WALL STRETCHING │ │ │ Deficiency / dysfunction of │ │
│ → visceral pain │ │ │ Interstitial Cells of Cajal │ │
│ (colicky / │ │ │ (ICC — pacemaker cells) → │ │
│ intermittent) │ │ │ lost slow waves / rhythmicity │ │
└────────┬──────────┘ │ └────────────────────────────────┘ │
│ └───────────────────┬───────────────────┘
│ │
▼ ▼
ALTERED MOTILITY INEFFECTIVE PERISTALSIS
(proximal hyper- → contents fail to advance
peristalsis, then
exhaustion)
│ │
└─────────────────┬────────────────────┘
▼
PROGRESSIVE BOWEL DISTENSION
+ STASIS + BACTERIAL OVERGROWTH
│
┌──────────────┼──────────────────┐
▼ ▼ ▼
MALABSORPTION INCREASED MUCOSAL INJURY
• Fat, protein INTRALUMINAL • Ulceration
• Vitamins SECRETIONS • Translocation of
• Malnutrition → Vomiting bacteria
→ Sepsis
│
▼
RAISED INTRALUMINAL PRESSURE
│
┌────────┴────────────┐
▼ ▼
VENOUS CONGESTION (In complete obstruction)
→ mucosal ischaemia ARTERIAL ISCHAEMIA
→ NECROSIS → PERFORATION
→ PERFORATION → PERITONITIS
Sleisenger & Fordtran's GI and Liver Disease | Sabiston Textbook of Surgery | Schwartz's Principles of Surgery
4. CLINICAL FEATURES
Symptoms
| Symptom | Description |
|---|---|
| Abdominal pain | Most consistent symptom; colicky, intermittent; may be dull and chronic in CIPO; worsens with eating |
| Abdominal distension | Progressive; particularly severe during acute-on-chronic episodes |
| Nausea & vomiting | Intermittent initially; bilious if proximal obstruction; feculent if distal/low obstruction |
| Constipation / obstipation | Gradual worsening over weeks–months; may alternate with diarrhoea (overflow) |
| Weight loss & malnutrition | Due to malabsorption, reduced oral intake, bacterial overgrowth; prominent in CIPO |
| Early satiety / bloating | After meals; relief with fasting |
| Change in bowel habit | Progressive constipation preceded by weeks–months in LBO |
Signs
| Sign | Significance |
|---|---|
| Abdominal distension | Tympanic to percussion |
| Visible peristalsis | Peristaltic waves visible through abdominal wall — ladder pattern in SBO |
| High-pitched / tinkling bowel sounds | Mechanical obstruction |
| Absent / diminished bowel sounds | CIPO / late exhaustion |
| Succussion splash | Gastric / proximal small bowel obstruction |
| Palpable mass | Tumour, faecal impaction, hernia |
| Hernia orifices | Examine groins, umbilicus, scars (irreducible = obstructing) |
| Cachexia / wasting | Malignancy, chronic malnutrition |
| Rectal exam | Empty rectum in obstruction; impacted faeces; blood — malignancy |
| Signs of malignancy | Sister Mary Joseph nodule, Virchow's node (left), hepatomegaly |
Features Specific to CIPO
- Recurrent acute episodes superimposed on chronic dysmotility
- Symptoms often fluctuate — better with fasting, worse after meals
- No mechanical cause found on imaging despite clinical picture of obstruction
- Small bowel dilatation on imaging with no transition point
- Prominent nutritional failure and malabsorption
Sleisenger & Fordtran | Schwartz's Principles of Surgery | Harrison's Principles of Internal Medicine 22e
5. DIAGNOSIS / INVESTIGATIONS
| Investigation | Finding / Purpose |
|---|---|
| Plain AXR (erect + supine) | Dilated loops of bowel; air-fluid levels; absent distal gas; "string of beads" (SBO); colonic dilatation (LBO/CIPO); caecal diameter >12–14 cm = emergency |
| CT Abdomen/Pelvis (IV ± oral contrast) | Gold standard; identifies site, cause, and complications; detects transition point, mass, volvulus, ischaemia (wall non-enhancement), abscess, peritoneal disease |
| CT Enteroclysis | Optimal for low-grade partial SBO; water-soluble contrast via naso-enteric tube distends loops for accurate assessment |
| Contrast studies (water-soluble) | Gastrografin enema for LBO; "apple-core" = carcinoma; delineates point of obstruction |
| Colonoscopy / flexible sigmoidoscopy | Diagnose and stent colonic tumours; decompress volvulus |
| Small bowel follow-through (SBFT) / MRI enterography | Crohn's disease strictures; radiation strictures; chronic partial SBO |
| Intestinal manometry | Key in CIPO: differentiates mechanical from functional obstruction; identifies neuropathic vs. myopathic pattern |
| Full-thickness biopsy (laparoscopic) | In CIPO: identifies ICC deficiency, myopathy, neuropathy — seldom reveals treatable cause |
| Bloods | FBC (anaemia, leukocytosis); CRP/ESR; U&E (dehydration, electrolyte disturbances); LFTs; serum albumin (nutritional status); TFTs (hypothyroidism); Ca²⁺ (hypoparathyroidism); glucose (DM) |
| Tumour markers | CEA, CA-125, CA 19-9 — if malignancy suspected |
| Urine / serum | Thymidine phosphorylase (MNGIE); lactate, CPK (mitochondrial disease) |
| Autoimmune screen | ANA, anti-Scl-70 (scleroderma); anti-Hu (paraneoplastic neuropathy) |
6. MANAGEMENT (Table Form)
A. MEDICAL MANAGEMENT
| Intervention | Indication / Details |
|---|---|
| IV Fluid Resuscitation | Correct dehydration; Hartmann's / Normal saline; monitor urine output |
| Nasogastric (NG) tube decompression | Decompress proximal bowel; remove accumulated gas/fluid; relieve vomiting |
| Electrolyte correction | K⁺, Na⁺, Cl⁻ — especially with vomiting; hypochloraemic hypokalaemic alkalosis (proximal obstruction) |
| NPO / bowel rest | Reduce luminal contents and distension |
| Nutritional support | Enteral (jejunal tube if feasible) preferred; Total parenteral nutrition (TPN) if severe CIPO or prolonged obstruction; high-calorie, high-protein liquid diet in partial obstruction |
| Antibiotics | Broad-spectrum (e.g., piperacillin-tazobactam, metronidazole) for bacterial translocation / sepsis; cover anaerobes + gram-negatives |
| Analgesia | Opioids for acute pain (avoid prolonged use — worsen motility); NSAIDs / antispasmodics for colicky pain |
| Antiemetics | Metoclopramide (partial/functional only), ondansetron, haloperidol; avoid metoclopramide in complete obstruction |
| Octreotide | Inhibits GI secretion → reduces distension, vomiting, colicky pain; key in malignant / CIPO obstruction; 100–300 mcg SC/IV TDS |
| Steroids (dexamethasone) | Anti-inflammatory; reduce peritoneal oedema; useful in malignant obstruction and CIPO (acute episodes) |
| Prokinetics (CIPO) | Pyridostigmine (acetylcholinesterase inhibitor — increases ACh at neuromuscular junction → promotes contractions); Neostigmine (IV — acute episodes); Prucalopride (5-HT₄ agonist); Erythromycin (motilin agonist) |
| Treat underlying cause | Levothyroxine (hypothyroidism); calcium (hypoparathyroidism); stop offending drugs (opioids, TCAs); treat Chagas disease, Parkinson's disease; immunosuppression for connective tissue disease |
| Endoscopic stenting | Self-expanding metal stents (SEMS): for colonic malignancy — bridge to surgery OR palliation; also gastroduodenal, jejunal; avoids emergency surgery |
| Colonoscopic decompression | Sigmoid/caecal volvulus — effective in up to 85% of sigmoid volvulus cases; recurrence is high — follow with elective surgery |
| Venting gastrostomy / gastrostomy tube | Palliative; avoids prolonged NG tube; allows oral intake for pleasure in inoperable malignant obstruction |
| Water-soluble contrast (Gastrografin) | Therapeutic in adhesion-related partial SBO: draws fluid into lumen, promotes resolution; also diagnostic |
B. SURGICAL MANAGEMENT
| Procedure | Indication | Notes |
|---|---|---|
| Adhesiolysis | Adhesive chronic/partial SBO | Laparoscopic preferred; open if dense/multiple adhesions |
| Bowel resection + anastomosis | Malignant stricture, Crohn's stricture, radiation stricture, ischaemic stricture | Primary anastomosis if bowel viable and patient stable |
| Strictureplasty | Crohn's disease — multiple strictures, preserve bowel length | Heineke-Mikulicz / Finney technique |
| Colostomy / Ileostomy | Decompressing stoma for LBO; palliation | Hartmann's procedure for perforated/obstructing sigmoid carcinoma |
| Right hemicolectomy | Right-sided colonic carcinoma | Includes terminal ileum; ileo-colic anastomosis |
| Left hemicolectomy / sigmoid resection | Left colonic / sigmoid carcinoma | Primary anastomosis or staged (Hartmann's) |
| Hernia repair + bowel resection | Obstructing hernia | Reduce bowel; resect if non-viable; mesh repair after contamination controlled |
| Volvulus reduction + resection | Sigmoid volvulus (after failed endoscopy); caecal volvulus | Sigmoid: resection + primary anastomosis or Hartmann's; Caecal: right hemicolectomy |
| Bypass surgery | Unresectable tumour; dense adhesions | Entero-enterostomy or gastrojejunostomy |
| Percutaneous endoscopic / IR gastrostomy | Malignant obstruction — palliation; CIPO — vent | Relieves nausea/vomiting; allows oral intake |
| Intestinal transplantation | End-stage CIPO with intestinal failure requiring long-term TPN | Specialist centre; last resort |
| Peritoneal carcinomatosis: cytoreductive surgery (CRS) + HIPEC | Selected patients with peritoneal malignancy | High morbidity; strict patient selection |
Harrison's Principles 22e | Sleisenger & Fordtran | Schwartz's Principles of Surgery | Current Surgical Therapy 14e
7. ALGORITHM TO APPROACH CHRONIC INTESTINAL OBSTRUCTION
PATIENT: Chronic / Progressive Abdominal Pain, Distension,
Vomiting, Constipation (weeks–months duration)
│
▼
HISTORY & PHYSICAL EXAMINATION
(Duration, bowel habit change, weight loss, prior
surgery, malignancy, hernia, medications, family Hx)
│
▼
INITIAL INVESTIGATIONS
(FBC, U&E, CRP, LFTs, albumin, TFTs, Ca²⁺,
tumour markers; erect + supine AXR)
│
▼
DILATED BOWEL ON AXR?
┌──────────────────────┐
▼ ▼
YES NO
CT Abdomen/Pelvis Consider other diagnosis
with IV contrast (IBS, gastroparesis,
│ constipation, etc.)
▼
─────────────────────────────────────────
IDENTIFY: MECHANICAL vs FUNCTIONAL
─────────────────────────────────────────
│
┌──────┴────────────────────────────────┐
▼ ▼
MECHANICAL OBSTRUCTION FUNCTIONAL (CIPO)
(transition point, mass, (dilated bowel, no
stricture, hernia on CT) transition point)
│ │
▼ ▼
DETERMINE SITE RULE OUT MECHANICAL
│ (CT enteroclysis /
├── SMALL BOWEL (SBO) water-soluble contrast)
│ │
└── LARGE BOWEL (LBO) INTESTINAL MANOMETRY
│ FULL-THICKNESS BIOPSY
▼ SEARCH FOR SECONDARY CAUSE
DETERMINE CAUSE (TFTs, ANA, anti-Hu,
│ glucose, drugs review)
├── ADHESIONS / BANDS │
├── MALIGNANCY ▼
├── HERNIA TREAT UNDERLYING CAUSE
├── CROHN'S STRICTURE + SUPPORTIVE MANAGEMENT
├── RADIATION STRICTURE (See Medical Mx above)
├── VOLVULUS │
└── OTHER ▼
│ NUTRITIONAL SUPPORT
▼ (oral → enteral → TPN)
IS THERE ISCHAEMIA / PERFORATION? │
│ ▼
┌─────┴──────┐ PROKINETICS (Pyridostigmine,
▼ ▼ Prucalopride, Neostigmine,
YES NO Octreotide for secretions)
│ │ │
▼ ▼ ┌─────────┴─────────┐
EMERGENCY COMPLETE vs ▼ ▼
SURGERY PARTIAL? IMPROVES FAILS TO IMPROVE
(IV ABx, │ (Continue (Endoscopic /
resuscitate, │ medical Mx) Surgical options)
urgent OR) │
┌───────┴───────┐
▼ ▼
COMPLETE PARTIAL
│ │
▼ ▼
URGENT TRIAL OF
SURGICAL CONSERVATIVE Mx
ASSESSMENT • IV fluids / NG tube
│ • Water-soluble contrast
▼ • 24–48 h observation
RESUSCITATE • Repeat CT at 48h if
IV ABx, NG no improvement
Correct │
electrolytes ▼
│ RESOLVES? FAILS?
▼ │ │
SURGERY ▼ ▼
┌────────┐ Discharge SURGERY
│ BY │ + elective ┌────────────────────────────────────┐
│ CAUSE │ workup │ BY CAUSE: │
└────────┘ │ • Adhesiolysis (laparoscopic/open) │
• Adhesiolysis │ • Bowel resection ± anastomosis │
• Resection ± anastomosis │ • Strictureplasty (Crohn's) │
• Hernia repair │ • Colostomy / Hartmann's │
• Decompressing stoma │ • Hernia repair │
• Bypass │ • Volvulus reduction/resection │
• Volvulus Rx │ • Stenting (SEMS) — malignancy │
• SEMS for malignancy │ • Bypass / stoma (palliation) │
(bridge to surgery or └────────────────────────────────────┘
palliation)
Sources: Sleisenger & Fordtran's Gastrointestinal and Liver Disease | Schwartz's Principles of Surgery 11e | Current Surgical Therapy 14e | Mulholland & Greenfield's Surgery 7e | Harrison's Principles of Internal Medicine 22e
This is a shared conversation. Sign in to Orris to start your own chat.