Shoulder joint make proper notes so we get full marks 15marks with 3 4 easy diagram mbbs level in india based on standard books like vishram singh, BDC
SHOULDER JOINT (GLENOHUMERAL JOINT)
MBBS Anatomy Notes | 15 Marks | Based on Gray's Anatomy for Students & Vishram Singh
1. INTRODUCTION
- Type: Synovial ball-and-socket joint (multiaxial)
- Articulation: Large spherical head of humerus + small shallow glenoid cavity of scapula
- Key feature: Most mobile joint in the body - wide range of movement at the cost of stability
- Stability is provided by surrounding soft tissues, NOT bony architecture
Mnemonic for stability: "RBLC" - Rotator cuff, Biceps long head, Ligaments, Coracoacromial arch
2. ARTICULAR SURFACES
| Surface | Bone | Covering |
|---|---|---|
| Head of humerus | Humerus | Hyaline cartilage |
| Glenoid cavity | Scapula | Hyaline cartilage |
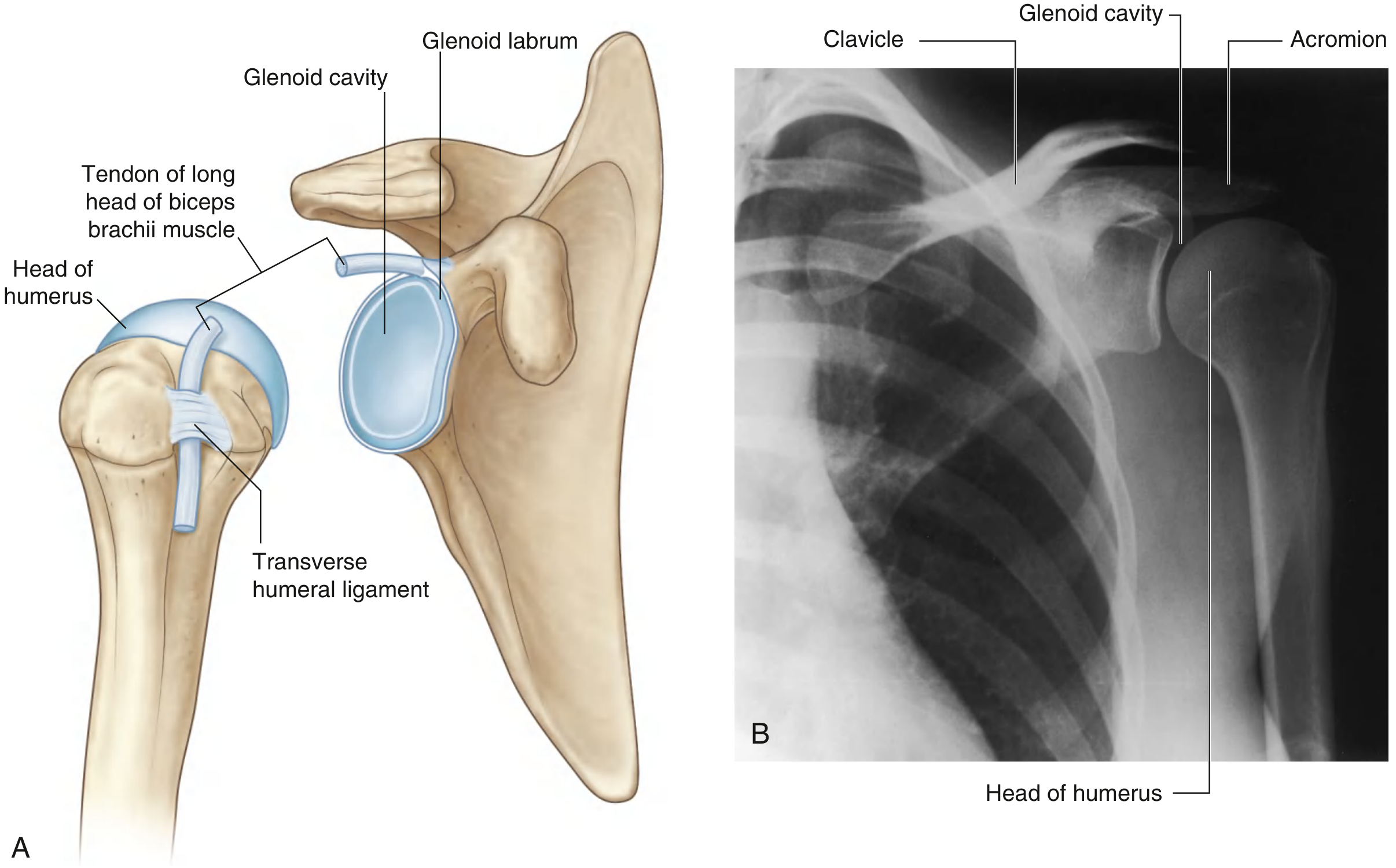
- The glenoid cavity is only 1/3rd the size of the humeral head
- Deepened by the glenoid labrum - a fibrocartilaginous rim attached to the margin of the glenoid fossa
- Superiorly, the labrum is continuous with the tendon of the long head of biceps brachii, which attaches to the supraglenoid tubercle
DIAGRAM 1 - Articular Surfaces of Glenohumeral Joint
3. JOINT CAPSULE
Fibrous Membrane:
- Attaches medially: to margin of glenoid cavity (outside attachment of glenoid labrum)
- Attaches laterally: to anatomical neck of humerus
- On the medial side of humerus, the attachment extends onto the shaft - forming a loose/redundant fold that accommodates abduction
- Inferiorly, the capsule is also loose - allows for full abduction
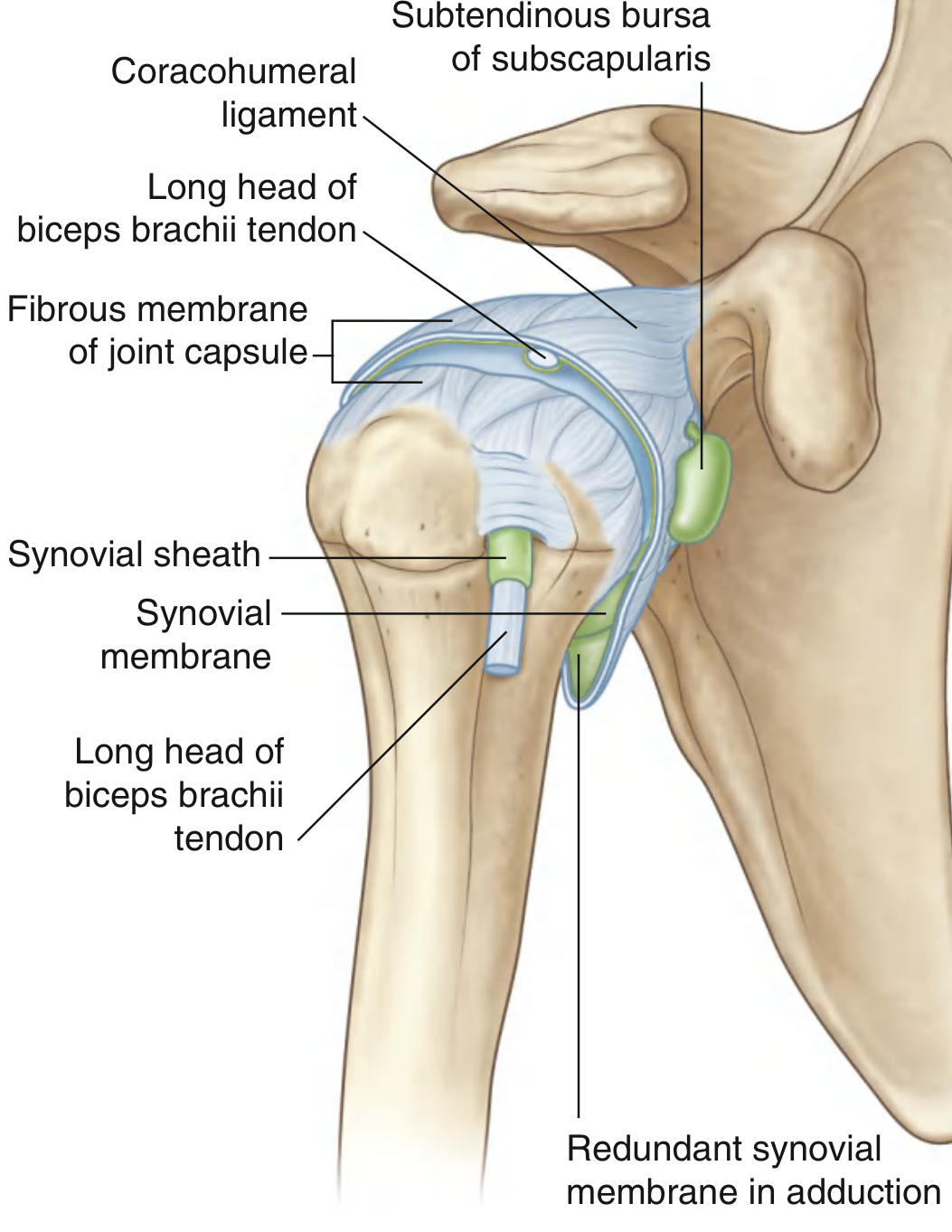
Openings in the fibrous membrane:
- Anteriorly - for subtendinous bursa of subscapularis to communicate with joint cavity
- In the intertubercular sulcus - for passage of tendon of long head of biceps (surrounded by synovial sheath)
4. SYNOVIAL MEMBRANE
- Attaches to margins of articular cartilage
- Lines the fibrous capsule from inside
- Redundant inferiorly (accommodates abduction)
- Protrudes through apertures in the fibrous membrane to form bursae
- Folds around the long head of biceps tendon as it passes through the joint
DIAGRAM 2 - Synovial Membrane and Joint Capsule
5. LIGAMENTS
A. Intrinsic Ligaments (thickenings of fibrous capsule):
| Ligament | Attachment | Function |
|---|---|---|
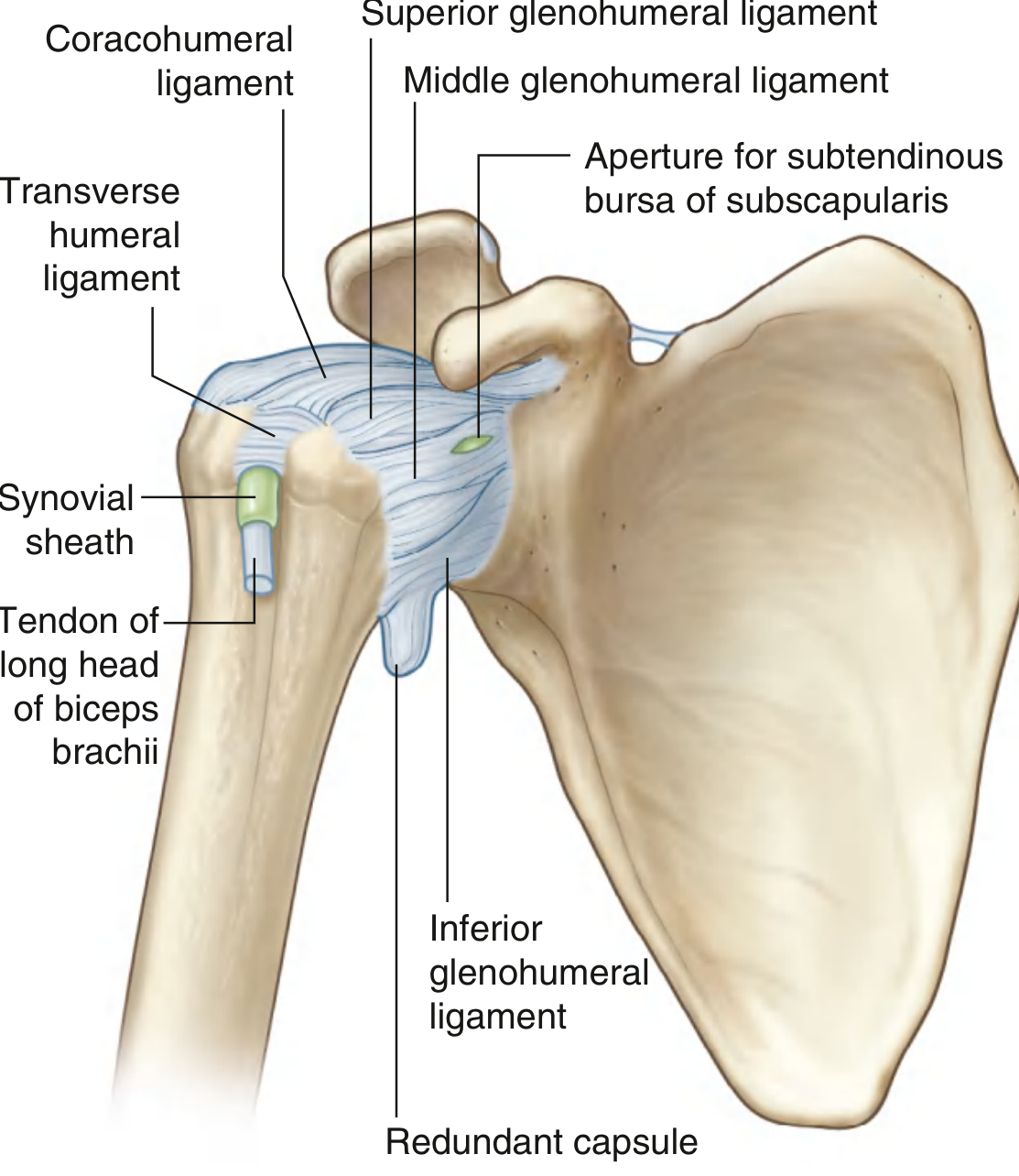
| Superior glenohumeral | Superomedial glenoid margin → lesser tubercle & intertubercular groove | Resists inferior translation |
| Middle glenohumeral | Upper glenoid margin → anatomical neck | Resists anterior displacement |
| Inferior glenohumeral | Inferior glenoid margin → anatomical neck (has anterior band, posterior band, axillary recess) | Most important - prevents anterior-inferior dislocation; forms a "hammock" during abduction |
| Coracohumeral | Base of coracoid process → greater and lesser tubercles | Stabilizes long head of biceps tendon in intertubercular sulcus |
| Transverse humeral | Greater tubercle → lesser tubercle | Holds long head of biceps in intertubercular sulcus |
B. Extrinsic Ligament:
- Coracoacromial ligament: Coracoid process → acromion
- Forms the coracoacromial arch - protects the superior aspect of the joint
- Together with the acromion and coracoid, prevents superior dislocation of humeral head
High-yield: The inferior glenohumeral ligament is the most important static stabilizer against anterior-inferior dislocation (the most common type of shoulder dislocation)
DIAGRAM 3 - Ligaments of Right Glenohumeral Joint (Anterior View)
6. BURSAE
Bursae communicating with joint cavity:
- Subtendinous bursa of subscapularis - between subscapularis muscle and fibrous membrane (most consistent)
Bursae NOT communicating with joint cavity:
- Subacromial (subdeltoid) bursa - between acromion/deltoid and supraspinatus/joint capsule (clinically most important)
- Between acromion and skin
- Between coracoid process and joint capsule
- Related to tendons of coracobrachialis, teres major, long head of triceps, latissimus dorsi
Clinical note: Inflammation of the subacromial bursa (subacromial bursitis) causes painful arc syndrome - pain during 60°-120° of abduction
7. STABILITY OF THE JOINT
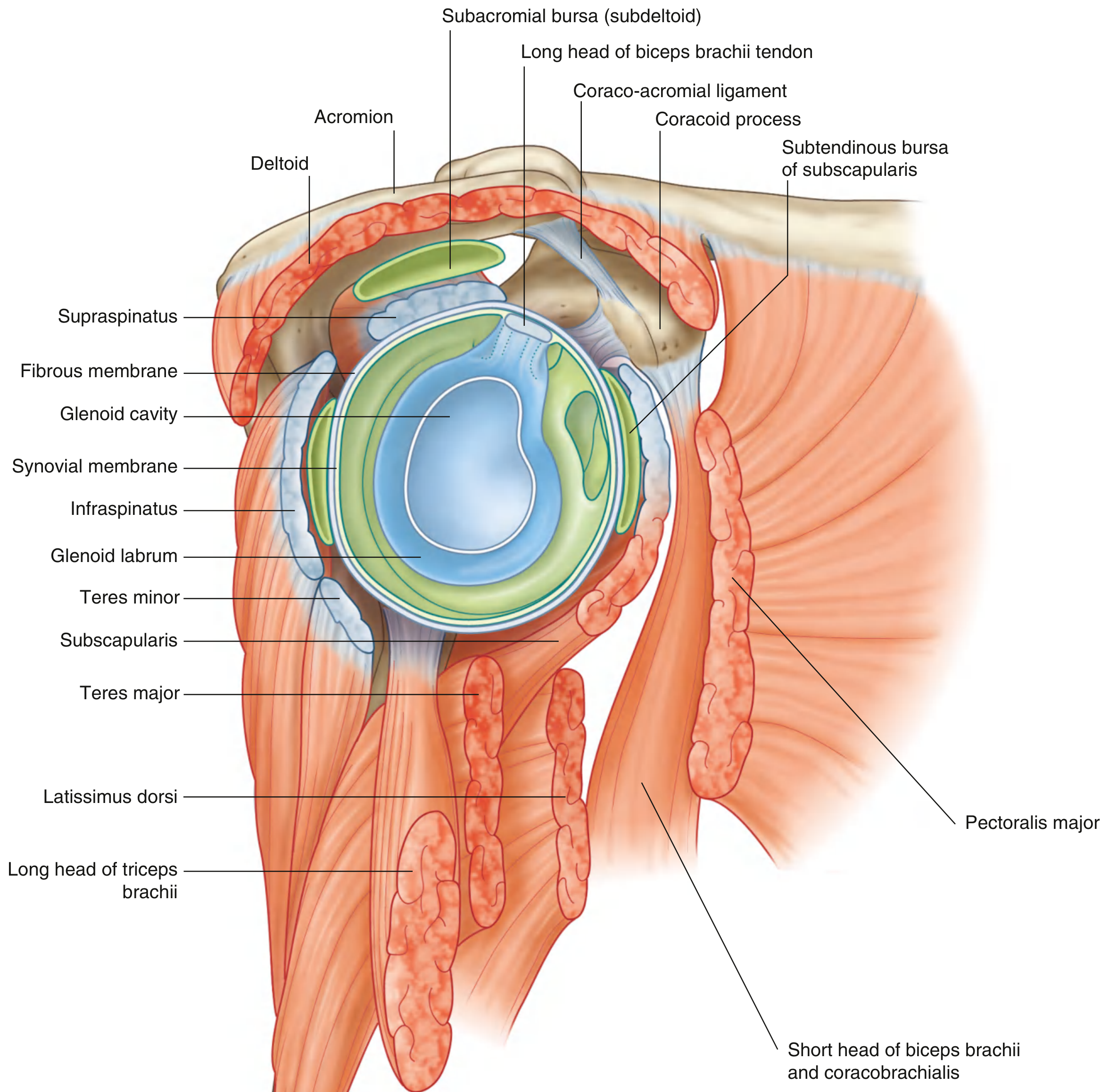
A. ROTATOR CUFF (Dynamic stabilizers - most important)
| Muscle | Origin | Insertion | Action | Nerve |
|---|---|---|---|---|
| Supraspinatus | Supraspinous fossa | Greater tubercle (superior facet) | Initiates abduction (0-15°) | Suprascapular (C5,6) |
| Infraspinatus | Infraspinous fossa | Greater tubercle (middle facet) | Lateral rotation | Suprascapular (C5,6) |
| Teres minor | Lateral border of scapula | Greater tubercle (inferior facet) | Lateral rotation | Axillary (C5,6) |
| Subscapularis | Subscapular fossa | Lesser tubercle | Medial rotation | Upper & lower subscapular (C5,6,7) |
Mnemonic: "SITS" - Supraspinatus, Infraspinatus, Teres minor, SubscapularisThe cuff surrounds posterior, superior, and anterior aspects of the joint (NOT inferior - hence inferiorly is the weak point - "axillary recess")
B. Long Head of Biceps Brachii
- Passes superiorly through the joint cavity
- Restricts upward displacement of humeral head
- Acts as an additional stabilizer
C. Coracoacromial Arch
- Formed by coracoid process + coracoacromial ligament + acromion
- Prevents superior dislocation
D. Glenoid Labrum
- Deepens the socket and increases contact area
DIAGRAM 4 - Rotator Cuff and Surrounding Muscles (Lateral/Coronal View)
8. MOVEMENTS
| Movement | Muscles | Range |
|---|---|---|
| Flexion | Anterior deltoid, pectoralis major (clavicular head), biceps brachii, coracobrachialis | 0-180° |
| Extension | Posterior deltoid, latissimus dorsi, teres major | 0-60° |
| Abduction | Supraspinatus (0-15°), deltoid (15-90°), trapezius + serratus anterior (90-180°) | 0-180° |
| Adduction | Pectoralis major, latissimus dorsi, teres major | - |
| Medial rotation | Subscapularis, pectoralis major, latissimus dorsi, teres major, anterior deltoid | 0-70° |
| Lateral rotation | Infraspinatus, teres minor, posterior deltoid | 0-90° |
| Circumduction | All the above muscles | - |
Important: Full abduction (180°) requires scapular rotation (by trapezius and serratus anterior) in addition to glenohumeral movement. The glenohumeral:scapular rotation ratio = 2:1.
9. BLOOD SUPPLY
- Anterior circumflex humeral artery (branch of axillary artery)
- Posterior circumflex humeral artery (branch of axillary artery)
- Suprascapular artery (branch of thyrocervical trunk)
The anterior circumflex humeral artery is the main supply to the humeral head - damage in fracture-dislocation causes avascular necrosis
10. NERVE SUPPLY
| Nerve | Source |
|---|---|
| Axillary nerve (C5,6) | Posterior cord of brachial plexus |
| Suprascapular nerve (C5,6) | Upper trunk of brachial plexus |
| Lateral pectoral nerve (C5,6,7) | Lateral cord of brachial plexus |
| Posterior cord branches | Brachial plexus |
Hilton's law: Muscles acting on a joint and the skin overlying those muscles receive innervation from the same nerve.Axillary nerve injury: Most common nerve injury with shoulder dislocation/surgical neck fracture - causes loss of shoulder abduction (deltoid paralysis) + loss of sensation over the "regimental badge area" (lower deltoid)
11. RELATIONS
| Position | Structures |
|---|---|
| Anterior | Subscapularis muscle, subtendinous bursa of subscapularis |
| Superior | Supraspinatus muscle, coracoacromial arch, subacromial bursa |
| Posterior | Infraspinatus, teres minor muscles |
| Inferior | Long head of triceps, axillary nerve and posterior circumflex humeral vessels (through quadrangular space) |
| Inside joint | Long head of biceps tendon (intra-articular but extrasynovial) |
12. DISLOCATION OF SHOULDER JOINT
Most Common Direction: ANTERIOR (Subcoracoid) - 95%
- The inferior aspect of the capsule is weakest (no rotator cuff reinforcement)
- When the arm is forcefully abducted + externally rotated, the humeral head is levered anteroinferiorly
- The inferior glenohumeral ligament tears
- Loss of normal rounded contour of shoulder (flattening)
- Arm held in slight abduction and external rotation
- Hollow below acromion (empty glenoid)
- Axillary nerve injury - loss of sensation over regimental badge area
- Axillary nerve injury (most common)
- Recurrent dislocation (especially in young patients)
- Bankart lesion - tear of anterior glenoid labrum
- Hill-Sachs lesion - posterolateral compression fracture of humeral head
- Rotator cuff tear (especially in elderly)
- Axillary artery injury (rare)
QUICK REVISION TABLE
| Feature | Details |
|---|---|
| Type | Synovial, ball-and-socket, multiaxial |
| Articular cartilage | Hyaline |
| Labrum | Fibrocartilage, deepens glenoid |
| Capsule attachment | Glenoid margin → anatomical neck humerus |
| Intra-articular tendon | Long head of biceps (extra-synovial) |
| Weakest point | Inferiorly (no rotator cuff) |
| Most common dislocation | Anterior (subcoracoid) |
| Most common nerve injured | Axillary nerve (C5,6) |
| Blood supply | Ant. + Post. circumflex humeral + suprascapular |
| Rotator cuff mnemonic | SITS |
HIGH-YIELD EXAM POINTS (for 15-mark questions)
- Glenoid labrum - fibrocartilaginous, continuous with long head of biceps superiorly; torn in Bankart lesion
- Rotator cuff = SITS - surrounds anterior, superior, posterior; NOT inferior (hence inferiorly is the weak spot)
- Subacromial bursa does NOT communicate with joint cavity (unlike subscapularis bursa)
- Long head of biceps is intra-articular but extra-synovial (enclosed in synovial sheath)
- Axillary nerve (C5,6) - passes through quadrangular space, supplies deltoid + teres minor; most commonly injured in shoulder dislocation
- Inferior glenohumeral ligament = most important static stabilizer; forms "hammock" during abduction
- Coracoacromial arch = secondary protection superiorly; prevents superior dislocation
- Scapulohumeral rhythm - 2:1 ratio (glenohumeral : scapular rotation) for full 180° abduction
- Transverse humeral ligament - retains biceps tendon in intertubercular sulcus
- Anterior circumflex humeral artery - main blood supply to humeral head; damage = avascular necrosis
Makes more easy diagram so I made in exam easily
Simple hand-drawn style anatomy diagram of shoulder joint articular surfaces for MBBS exam. Clean black and white line drawing on white background. Show: glenoid cavity (scapula, shallow cup shape on the right), head of humerus (large ball on left), fibrocartilaginous glenoid labrum rim around glenoid cavity clearly labeled with an arrow, transverse humeral ligament bridging greater and lesser tubercles, long head of biceps tendon passing through joint labeled, hyaline cartilage shown on both surfaces. All labels in clear bold text with neat leader lines. Style: simple textbook schematic, easy to reproduce by hand in an exam in 2-3 minutes
Simple hand-drawn style anatomy diagram of shoulder joint ligaments anterior view for MBBS exam. Clean black line drawing on white background. Show the shoulder joint from the front: scapula with glenoid on right, humerus on left. Draw and clearly label: 1) Coracohumeral ligament (from coracoid process to greater and lesser tubercles), 2) Superior glenohumeral ligament, 3) Middle glenohumeral ligament, 4) Inferior glenohumeral ligament (thickest, most important - mark with asterisk), 5) Transverse humeral ligament, 6) Coracoacromial ligament (from coracoid to acromion forming the arch). Use different line thicknesses for different ligaments. Include small labels: "WEAK AREA = inferior" with arrow pointing down. Bold clear text labels, neat leader lines. Style: simple schematic easy to copy in exam
Simple hand-drawn style diagram of rotator cuff muscles SITS for MBBS exam. Clean black and white schematic on white background. Show scapula from the back (posterior view) and humerus. Draw and label the 4 rotator cuff muscles wrapping around the joint like a cuff: 1) Supraspinatus (top - from supraspinous fossa to greater tubercle, label: abduction initiator), 2) Infraspinatus (posterior - from infraspinous fossa to greater tubercle, label: lateral rotation), 3) Teres minor (inferior posterior - from lateral border scapula to greater tubercle, label: lateral rotation), 4) Subscapularis (anterior - from subscapular fossa to lesser tubercle, label: medial rotation). Show the gap inferiorly with label "NO CUFF HERE = WEAK POINT = site of dislocation". Large bold mnemonic box: "SITS = S-I-T-S". Simple exam-friendly style
Simple hand-drawn style diagram of bursae around shoulder joint for MBBS exam. Clean black and white schematic on white background. Coronal section view of shoulder showing: acromion at top, deltoid muscle over it, humerus below, glenoid cavity and scapula to the right. Clearly draw and label with arrows: 1) Subacromial bursa (subdeltoid bursa) - between acromion/deltoid and supraspinatus - LARGE and colored gray, marked "DOES NOT communicate with joint", 2) Subtendinous bursa of subscapularis - anterior to subscapularis tendon - marked "COMMUNICATES with joint cavity" with a dotted line connection to joint, 3) Supraspinatus tendon labeled, 4) Joint cavity in center labeled. Use a box legend: "Communicates: subscapularis bursa only. Does NOT communicate: subacromial/subdeltoid bursa". Bold labels, simple style for quick exam reproduction
429 Too Many Requests. {'message': '{\n "error": {\n "code": 429,\n "message": "Resource exhausted. Please try again later. Please refer to https://cloud.google.com/vertex-ai/generative-ai/docs/error-code-429 for more details.",\n "status": "RESOURCE_EXHAUSTED"\n }\n}\n', 'status': 'Too Many Requests'}
We encountered an error while processing your request. Please try again or reach out to us for help.
Generate PDF
An error occurred (ValidationException) when calling the ConverseStream operation: Expected toolResult blocks at messages.20.content for the following Ids: tooluse_k44H2WUvOxRMq5eHqhsd7c, tooluse_8kRMbwCDeK7MydzDAvzOpF
We encountered an error while processing your request. Please try again or reach out to us for help.