Anti emetic drugs pharmacology according to kdt
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive content to write a detailed, KDT-style answer on antiemetic drug pharmacology. Let me compile it all.
Antiemetic Drugs - Pharmacology (KDT Style)
Note: KDT (Tripathi's Essentials of Medical Pharmacology) is not in the textbook library, but the content below is drawn from Katzung's Basic & Clinical Pharmacology (16th ed.) and Lippincott Illustrated Reviews: Pharmacology, which follow the same pharmacological framework as KDT.
Physiology of Vomiting - The Basis of Drug Action
Understanding antiemetics requires knowing the vomiting reflex pathways:
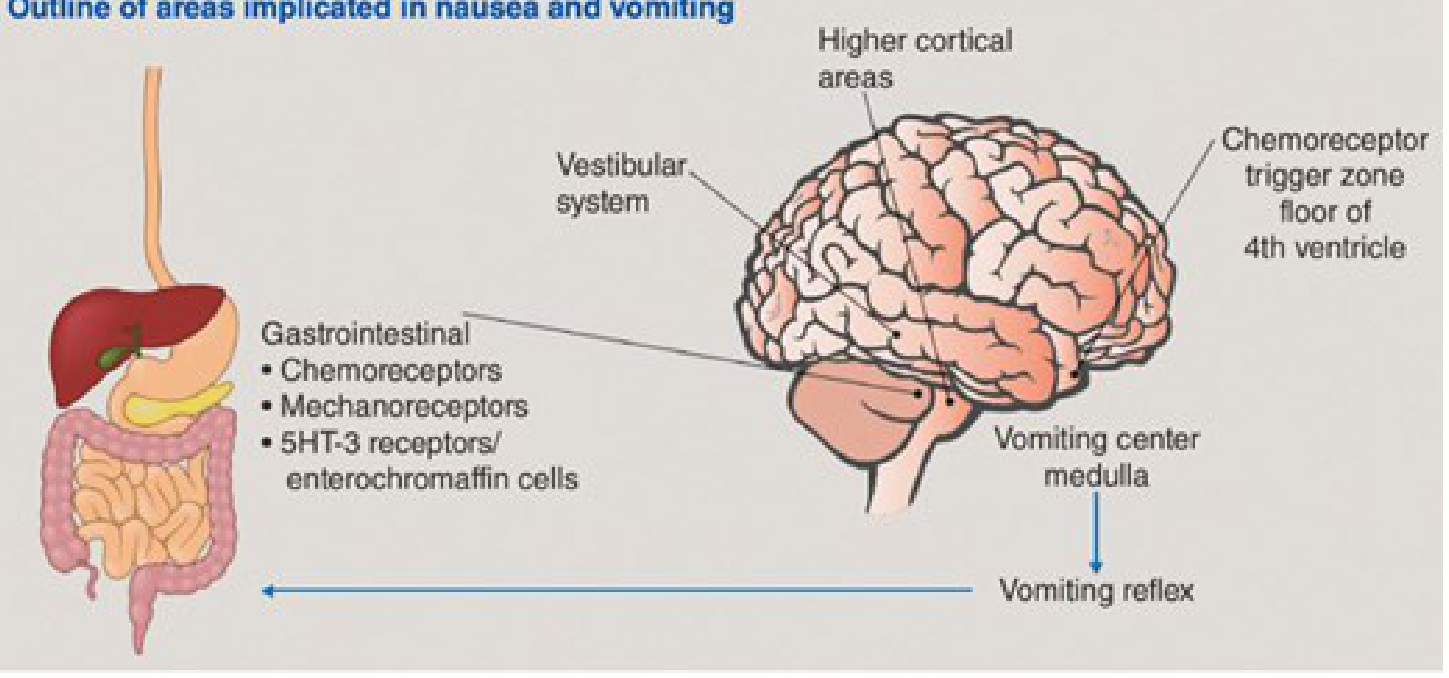
The vomiting center (VC) in the medulla receives input from four major sources:
-
Chemoreceptor Trigger Zone (CTZ) - located at the caudal end of the 4th ventricle (area postrema), outside the blood-brain barrier. It is accessible to emetogenic stimuli in blood/CSF. Rich in D2, opioid, 5-HT3, and NK1 receptors.
-
Vestibular system - via CN VIII; important in motion sickness. Rich in muscarinic M2 and H1 receptors.
-
Vagal/spinal GI afferents - rich in 5-HT3 receptors. GI mucosal irritation (chemotherapy, radiation, acute gastroenteritis) releases serotonin from enterochromaffin cells → activates 5-HT3 receptors → stimulates vagal afferents to VC and CTZ.
-
Higher CNS centers - involved in anticipatory vomiting, psychiatric disorders, stress.
Classification of Antiemetic Drugs
| Class | Drugs | Receptor Targeted |
|---|---|---|
| 5-HT3 antagonists | Ondansetron, Granisetron, Dolasetron, Palonosetron | 5-HT3 (central + peripheral) |
| NK1 antagonists | Aprepitant, Fosaprepitant, Rolapitant, Netupitant | NK1 (Substance P receptor) |
| Dopamine D2 antagonists | Metoclopramide, Domperidone, Prochlorperazine, Droperidol | D2 in CTZ |
| Phenothiazines | Prochlorperazine, Promethazine, Thiethylperazine | D2 + muscarinic + H1 |
| H1 antihistamines | Dimenhydrinate, Meclizine, Cyclizine, Diphenhydramine, Promethazine | H1 |
| Anticholinergics | Scopolamine | Muscarinic M1 |
| Corticosteroids | Dexamethasone, Methylprednisolone | Unknown |
| Cannabinoids | Dronabinol (THC), Nabilone | CB1 |
| Benzodiazepines | Lorazepam | GABAergic (for anticipatory vomiting) |
1. Serotonin 5-HT3 Receptor Antagonists ("Setrons")
Drugs: Ondansetron, Granisetron, Dolasetron, Palonosetron (tropisetron, ramosetron outside USA)
Mechanism
Block 5-HT3 receptors both centrally (in the VC and CTZ) and peripherally (on vagal afferent nerve terminals in the gut). Their antiemetic action is mainly through peripheral 5-HT3 blockade, reducing the GI serotonin signal that triggers the vomiting reflex. - Katzung's Basic and Clinical Pharmacology, 16th Ed.
Pharmacokinetics
- First-generation (ondansetron, granisetron, dolasetron): serum half-life 4-9 hours
- Second-generation (palonosetron): greater receptor affinity, half-life ~40 hours - more effective for delayed CINV
- All undergo extensive hepatic metabolism; dose reduction may be needed with ondansetron in hepatic insufficiency
- Available IV and oral; granisetron also available as transdermal patch
Clinical Uses
- First-line for chemotherapy-induced nausea and vomiting (CINV) - both prophylaxis and treatment
- Postoperative nausea and vomiting (PONV)
- Radiation-induced nausea (whole-body or abdominal radiation)
- Efficacy is enhanced by combining with dexamethasone + NK1 antagonist (triple therapy for CINV)
Doses (IV, 30 min before chemotherapy)
- Ondansetron: 8 mg IV or oral
- Granisetron: 1 mg IV, 2 mg oral
- Dolasetron: 100 mg
- Palonosetron: 0.25 mg IV, 0.5 mg oral
Adverse Effects
- Headache, dizziness, constipation (most common)
- QT prolongation - especially dolasetron; avoid in patients with long QT or on other QT-prolonging drugs. Palonosetron does NOT prolong QT.
- Serotonin syndrome risk when combined with SSRIs/SNRIs
2. NK1 (Neurokinin-1) Receptor Antagonists
Drugs: Aprepitant (oral), Fosaprepitant (IV prodrug), Rolapitant, Netupitant (in combo as AKYNZEO)
Mechanism
Block NK1 receptors (Substance P receptors) centrally in the CNS, specifically in the VC. Substance P is a key mediator of the delayed vomiting response. No effect on 5-HT, dopamine, or steroid receptors.
Clinical Uses
- Effective for both early AND delayed emesis in cancer chemotherapy - especially useful for delayed CINV (24-120 hours)
- Always used as add-on to a 5-HT3 antagonist + dexamethasone (triple antiemetic regimen)
Pharmacokinetics
- Aprepitant is given orally (125 mg day 1, 80 mg days 2-3)
- Fosaprepitant is an IV prodrug converted to aprepitant
- Metabolized by CYP3A4 - significant drug interactions
Adverse Effects & Drug Interactions
- Generally well tolerated: fatigue, dizziness, diarrhea
- CYP3A4 inhibitor/substrate: may increase levels of docetaxel, paclitaxel, etoposide, imatinib, vincristine, dexamethasone
- Reduces INR in patients on warfarin
- Drugs that inhibit CYP3A4 (ketoconazole, clarithromycin, ritonavir) significantly increase aprepitant levels
- Katzung's Basic and Clinical Pharmacology, 16th Ed.
3. Dopamine D2 Receptor Antagonists
A. Metoclopramide & Domperidone (Substituted Benzamides / Prokinetics)
Mechanism:
- Block D2 receptors in the CTZ (area postrema) → antiemetic
- Block peripheral D2 receptors in the GI tract → prokinetic (accelerates gastric emptying, increases LES tone)
- Metoclopramide also has mild 5-HT4 agonist activity (prokinetic) and at high doses blocks 5-HT3 receptors
Key Difference - Domperidone vs. Metoclopramide:
| Feature | Metoclopramide | Domperidone |
|---|---|---|
| BBB penetration | Yes | Minimal |
| CNS/extrapyramidal side effects | Common (5-25%) | Rare |
| Tardive dyskinesia risk | Yes (with long-term use) | Very rare |
| Galactorrhea/prolactin elevation | Yes | Yes (via pituitary, outside BBB) |
| Cardiac QT prolongation | No | Yes (avoid in cardiac disease) |
Clinical Uses:
- CINV, PONV
- Gastroparesis (diabetic, postsurgical)
- GERD
- Metoclopramide: facilitating nasoenteric tube placement
Doses: Metoclopramide 10-20 mg oral/IV every 6 hours
Adverse Effects of Metoclopramide:
- Extrapyramidal effects (dystonias, akathisia, parkinsonism) - acute in 25% at high doses, 5% long-term
- Tardive dyskinesia (irreversible) - avoid long-term use especially in elderly
- Restlessness, drowsiness, anxiety, insomnia (10-20%)
- Galactorrhea, gynecomastia, impotence, menstrual disorders (hyperprolactinemia)
- Black box warning for tardive dyskinesia
B. Phenothiazines
Drugs: Prochlorperazine, Promethazine, Thiethylperazine
Mechanism: Block D2 and muscarinic receptors (antiemetic action); also block H1 receptors (sedation). Act on the CTZ and VC.
Clinical Uses:
- Moderate efficacy for CINV, PONV, opioid-induced vomiting
- Prochlorperazine widely used in emergency settings
Adverse Effects: Sedation, extrapyramidal effects, anticholinergic effects, hypotension, QT prolongation
C. Butyrophenones
Drugs: Droperidol, Haloperidol
Mechanism: Central D2 blockade → potent antiemetic
Clinical Uses: PONV (droperidol); droperidol used IM/IV but causes extreme sedation
Adverse Effects:
- Extrapyramidal effects, hypotension
- QT prolongation → risk of torsades de pointes (fatal) - use only when other agents fail; screen for QT prolongation before use
4. H1 Antihistamines
Drugs: Dimenhydrinate, Meclizine, Cyclizine, Diphenhydramine, Promethazine
Mechanism: Block H1 receptors in the vestibular nuclei and VC
Clinical Uses:
- Most effective for motion sickness
- Effective for morning sickness (pregnancy-associated vomiting) - promethazine used
- Ineffective against CTZ-mediated emesis (chemo, drugs, toxins)
Adverse Effects: Sedation, anticholinergic effects (dry mouth, urinary retention, blurred vision, constipation)
5. Anticholinergic (Muscarinic Antagonists)
Drug: Scopolamine (hyoscine)
Mechanism: Block muscarinic M1 receptors in the vestibular apparatus and CNS
Clinical Uses:
- Best drug for motion sickness - transdermal patch applied behind ear
- Effective for postoperative nausea
- NOT effective for CINV or CTZ-mediated vomiting
Adverse Effects: Dry mouth, blurred vision, urinary retention, sedation, confusion (especially elderly)
6. Corticosteroids
Drugs: Dexamethasone, Methylprednisolone
Mechanism: Unknown - but they have clear antiemetic activity, especially potentiating the effect of 5-HT3 antagonists
Clinical Uses:
- Used as adjuncts in CINV regimens
- Standard regimen: dexamethasone 8-20 mg IV before chemotherapy, then 8 mg/day orally for 2-4 days
- Enhance efficacy of 5-HT3 antagonists for both acute and delayed CINV
7. Cannabinoids
Drugs: Dronabinol (delta-9-THC), Nabilone
Mechanism: Activate CB1 (cannabinoid) receptors in the CNS - suppress the vomiting center
Clinical Uses:
- Reserved for CINV refractory to other antiemetics
- FDA-approved for cancer chemotherapy-induced nausea
Adverse Effects:
- CNS effects (euphoria, dysphoria, sedation, "high"), dizziness
- Tachycardia, hypotension
- Potential for abuse; psychosis in susceptible individuals
- Not used first-line due to CNS side effects
Standard Antiemetic Regimens (KDT-style summary)
| Clinical Situation | Preferred Drugs |
|---|---|
| Highly emetogenic chemotherapy | 5-HT3 antagonist + NK1 antagonist + Dexamethasone (triple therapy) |
| Moderately emetogenic chemotherapy | 5-HT3 antagonist + Dexamethasone ± NK1 antagonist |
| Delayed CINV (>24 hrs) | Aprepitant + Dexamethasone |
| Motion sickness | Scopolamine (best) / H1 antihistamines |
| Postoperative vomiting | Ondansetron, Droperidol, Dexamethasone |
| Pregnancy (morning sickness) | Promethazine, Meclizine, Metoclopramide |
| Gastroparesis / GI motility disorder | Metoclopramide, Domperidone |
| Opioid-induced nausea | Metoclopramide, Prochlorperazine, Ondansetron |
| Refractory CINV | Dronabinol / Cannabinoids |
| Anticipatory vomiting | Lorazepam (benzodiazepine) |
Quick Comparison Table
| Drug | Receptor | Motion Sickness | CINV | PONV | ADRs |
|---|---|---|---|---|---|
| Ondansetron | 5-HT3 | No | +++ | +++ | Headache, QT ↑, constipation |
| Palonosetron | 5-HT3 (high affinity) | No | +++ (acute+delayed) | ++ | Headache, constipation; no QT |
| Aprepitant | NK1 | No | +++ (esp. delayed) | + | CYP3A4 interactions |
| Metoclopramide | D2 + 5-HT4 | No | ++ | ++ | Tardive dyskinesia, EPS |
| Domperidone | D2 (peripheral) | No | ++ | + | Cardiac QT ↑ |
| Prochlorperazine | D2, M, H1 | + | + | ++ | Sedation, EPS |
| Droperidol | D2 | No | + | ++ | QT ↑, sedation, EPS |
| Scopolamine | Muscarinic M1 | +++ | No | ++ | Anticholinergic |
| Dimenhydrinate | H1 | ++ | + | + | Sedation |
| Dexamethasone | Unknown | No | ++ (adjunct) | + | Hyperglycemia |
| Dronabinol | CB1 | No | + (refractory) | No | CNS "high", dysphoria |
Key KDT Points to Remember:
- The CTZ (outside BBB) responds to drugs/toxins in blood → targeted by D2 antagonists and 5-HT3 antagonists
- Vestibular emesis (motion sickness) → best treated with scopolamine or H1 antihistamines
- CINV → setrons are first-line; triple therapy with NK1 + steroid for highly emetogenic agents
- Metoclopramide crosses BBB → EPS and tardive dyskinesia risk; domperidone does NOT → safer CNS profile
- Palonosetron (2nd gen setron) is superior for delayed CINV due to its 40-hour half-life
- NK1 antagonists (aprepitant) uniquely cover delayed emesis (>24 hours) which setrons alone miss
Sources: Katzung's Basic and Clinical Pharmacology, 16th Ed.; Lippincott Illustrated Reviews: Pharmacology
This is a shared conversation. Sign in to Orris to start your own chat.