Differential diagnosis for back pain
Reading File
Finding Sources
Finding Sources
Searching the Web
differential diagnosis back pain clinical approach 2024
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
I now have all the information needed for a comprehensive, well-organized answer. Here it is:
Differential Diagnosis of Back Pain
Back pain is one of the most common clinical complaints. The vast majority (~97%) of cases have mechanical causes, but a systematic approach is essential to avoid missing serious pathology.
Overview: Three Broad Categories
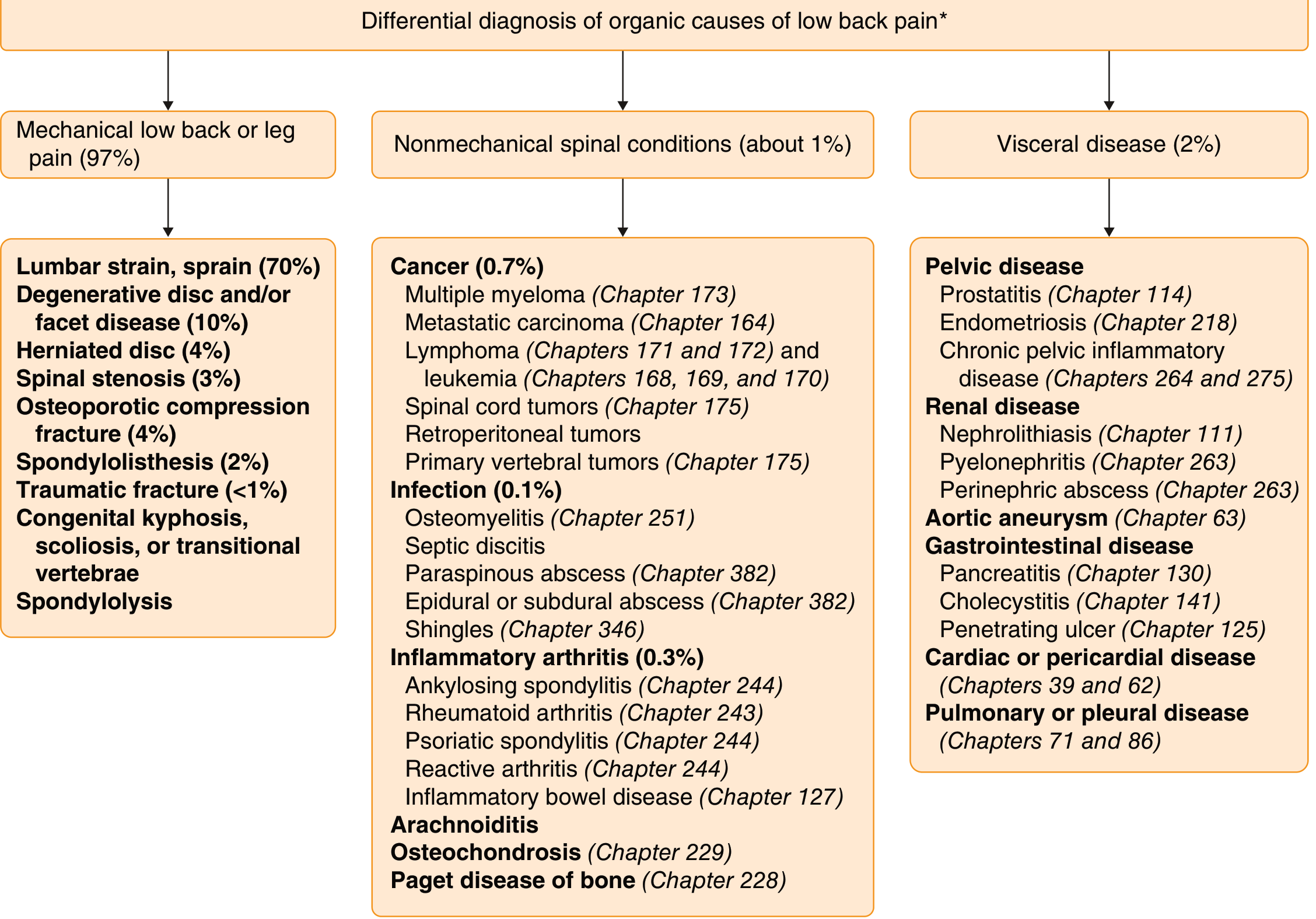
Goldman-Cecil Medicine — Differential diagnosis of organic causes of low back pain (percentages approximate)
1. Mechanical / Musculoskeletal (~97%)
| Condition | Key Features |
|---|---|
| Lumbar muscle strain / ligament sprain (~70%) | Acute onset, often after exertion; no neurological deficits; improves with rest |
| Degenerative disc & facet disease (~10%) | Chronic, worsens with activity; older adults; axial pain |
| Herniated nucleus pulposus (~4%) | Dermatomal radicular pain ± sensory/motor loss; ↑ with Valsalva/coughing |
| Osteoporotic compression fracture (~4%) | Acute severe pain in elderly; minimal or no trauma; kyphosis |
| Spinal stenosis (~3%) | Neurogenic claudication — bilateral leg pain/weakness ↑ with walking, ↓ with flexion |
| Spondylolisthesis (~2%) | Slippage of vertebral body; may be asymptomatic or cause radiculopathy |
| Traumatic fracture (<1%) | High-energy mechanism or low-energy in osteoporotic bone |
| Spondylolysis | Stress fracture of pars interarticularis; young athletes |
| Congenital deformity | Scoliosis, kyphosis, transitional vertebrae |
2. Nonmechanical Spinal Conditions (~1%)
Neoplastic (~0.7%)
- Metastatic carcinoma — most common (breast, prostate, lung, kidney, thyroid)
- Multiple myeloma
- Lymphoma / leukemia
- Primary vertebral tumors (e.g., osteoid osteoma, giant cell tumor)
- Spinal cord / intradural tumors
- Retroperitoneal tumors
Suspect in: age >50, history of cancer, pain worse at night or supine, unexplained weight loss.
Infectious (~0.1%)
- Vertebral osteomyelitis — Staph aureus most common; fever, ↑ ESR/CRP
- Septic discitis
- Epidural / paraspinous abscess — urgent: can compress cord
- Herpes zoster — radicular pain may precede rash by days
Risk factors: IV drug use, immunosuppression, recent bacteremia, spinal procedures.
Inflammatory Arthritis (~0.3%)
- Ankylosing spondylitis — young male; insidious onset; morning stiffness >1 h; improves with activity; ↑ with rest (opposite of mechanical)
- Psoriatic spondylitis
- Reactive arthritis (Reiter syndrome)
- Rheumatoid arthritis (cervical spine involvement)
- IBD-associated spondyloarthropathy
Other Nonmechanical Spinal
- Paget disease of bone
- Osteochondrosis
- Arachnoiditis — chronic pain after intrathecal procedure or surgery
3. Referred / Visceral Pain (~2%)
Vascular (Can Be Immediately Life-Threatening)
- Abdominal aortic aneurysm (AAA) — mid/low back pain radiating to hips; pulsatile mass; do not miss
- Aortic dissection — sudden tearing chest-to-back pain
- Spinal arteriovenous malformation — progressive myelopathy + pain
- Spinal cord infarction
Renal / Urologic
- Nephrolithiasis — colicky flank pain radiating to groin; hematuria
- Pyelonephritis — fever, CVA tenderness, dysuria
- Perinephric abscess
Gastrointestinal
- Pancreatitis — epigastric pain radiating to the back (L1 region); ↑ amylase/lipase
- Cholecystitis — mid-thoracic/right shoulder referred pain
- Penetrating peptic ulcer
- Diverticulitis
Pelvic / Gynecologic
- Endometriosis — cyclical low back/sacral pain
- Ectopic pregnancy — acute lower back/pelvic pain in reproductive-age women
- Pelvic inflammatory disease (PID)
- Prostatitis — sacral/perineal aching
Cardiac / Pulmonary
- Myocardial ischemia / infarction (rare back presentation)
- Pulmonary embolism / pleural disease — pleuritic mid-back pain
Neurological Causes (Classified Separately)
| Diagnosis | Distinguishing Feature |
|---|---|
| Radiculopathy | Dermatomal radiation; ↑ with coughing/straining; single nerve root pattern |
| Cauda equina syndrome | Bilateral leg weakness + bowel/bladder dysfunction + saddle anesthesia — surgical emergency |
| Lumbosacral plexopathy | Multi-root distribution; may be diabetic, neoplastic, or post-irradiation |
| Spinal epidural hematoma | Sudden severe back pain → rapid neurological deterioration |
| Guillain-Barré syndrome | Ascending weakness; back pain common early; CSF albuminocytologic dissociation |
Red Flags — Prompt Imaging / Urgent Workup
| Red Flag | Suggests |
|---|---|
| Age >50 with new onset or <20 years | Neoplasm, spondyloarthropathy |
| History of cancer | Metastatic disease |
| Constitutional symptoms (fever, weight loss, night sweats) | Infection or malignancy |
| Pain worse at night / supine | Tumor, infection |
| Neurological deficit | Cord compression, cauda equina |
| Bowel / bladder dysfunction | Cauda equina syndrome — emergency |
| Major trauma | Fracture |
| IV drug use / immunosuppression | Epidural abscess, osteomyelitis |
| Age >70 with minor trauma | Osteoporotic fracture |
| Prolonged corticosteroid use | Osteoporotic fracture |
| Morning stiffness >1 h, young patient, improves with activity | Inflammatory spondyloarthropathy |
A Quick Clinical Framework
- Pain location + radiation: Axial only → mechanical; dermatomal radiation → radiculopathy; non-dermatomal referred → visceral
- Age: <20 → spondylolysis, tumor (Ewing's); 20–50 → disc herniation, spondyloarthropathy; >50 → degenerative, metastases, osteoporotic fracture
- Onset: Acute after exertion → strain/disc; acute at rest → vascular/infectious; insidious → inflammatory or neoplastic
- Aggravating/relieving factors: ↑ with activity + ↓ with rest → mechanical; ↑ with rest + ↓ with activity → inflammatory; pain at night → tumor/infection
- Neurological exam: Always assess for motor weakness, sensory level, reflexes, and bowel/bladder function
Sources: Bradley and Daroff's Neurology in Clinical Practice; Goldman-Cecil Medicine; Neuroanatomy through Clinical Cases, 3rd Ed.
Management for low back pain and when to do investigations
Finding Sources
Finding Sources
Searching the Web
low back pain management guidelines 2024 investigation indications
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
I now have comprehensive, authoritative content from Harrison's 2025, Goldman-Cecil, Tintinalli's, Rosen's, and Bailey & Love's. I have everything needed for a thorough answer.
Management of Low Back Pain & When to Investigate
Guiding Principles
The vast majority of acute low back pain (LBP) is nonspecific and self-limiting — 80–90% of patients recover within 4–6 weeks without specific intervention. The priority is to:
- Identify and manage the small minority with serious ("red flag") pathology
- Avoid unnecessary investigations in uncomplicated cases
- Keep the patient active and functioning
"Mechanical low back pain, even with radicular symptoms, resolves without specific intervention within 30 days in most patients and within 3 months in 90% of patients." — Goldman-Cecil Medicine
Classification by Duration
| Type | Duration | Approach |
|---|---|---|
| Acute | <6 weeks | Reassurance, analgesia, activity continuation |
| Subacute | 6–12 weeks | As above + structured physiotherapy if not improving |
| Chronic | >3 months | Multimodal / biopsychosocial model; consider imaging |
Step 1: Initial Assessment — Screen for Red Flags
Before any treatment, rule out serious pathology requiring urgent workup or referral:
| Red Flag | Suggests |
|---|---|
| Fever, rigors, recent infection, IV drug use, immunosuppression | Spinal epidural abscess, osteomyelitis, discitis |
| History of cancer | Metastatic disease |
| Pain worst at night or at rest (not relieved by lying down) | Neoplasm or infection |
| Age >50, first episode of severe LBP | Malignancy, osteoporotic fracture |
| Major trauma; minor trauma in elderly/osteoporotic | Vertebral fracture |
| Unexplained weight loss | Malignancy |
| Bowel / bladder dysfunction or saddle anesthesia | Cauda equina syndrome — emergency |
| Progressive neurological deficit | Cord compression |
| Prolonged corticosteroid use | Osteoporotic fracture |
Non-Pharmacological Management (First-Line for All)
1. Activity Continuation (most important)
- Do not prescribe bed rest — patients resuming normal activities (using pain as the limiting factor) recover faster than those on bed rest
- Withhold formal exercise programs until the acute episode has significantly improved
2. Physical Therapy & Exercise
- Core-strengthening exercises, targeted physiotherapy for subacute/chronic LBP
- Yoga, tai chi, water gymnastics — all show beneficial effects for chronic LBP
- Exercise alone or combined with education is effective at preventing recurrence
- The effect of physiotherapy alone is modest but real
3. Heat / Cold
- Heat wrap provides moderate improvement in pain and function for acute LBP
- Evidence favors heat over cold
- Temporary symptomatic relief only
4. Spinal Manipulation (Chiropractic / Osteopathic)
- More helpful for acute than chronic LBP
- Small benefit; noninferior to other recommended physical therapies
- Not recommended as sole treatment
5. Massage
- Beneficial for acute and chronic LBP, especially soft tissue/spasmodic pain
- Benefits tend to be short-lived
6. Acupuncture
- Modest, short-lived benefit for both acute and chronic LBP
- Effects wane without continued therapy
7. Psychological Therapies (especially for Chronic LBP)
- Cognitive-behavioural therapy (CBT) — strongest evidence
- Mindfulness-based stress reduction, biofeedback, operant therapy
- High co-prevalence with depression (33–67%) and anxiety (10–30%) — address these
- Biopsychosocial model: identify psychosocial "yellow flags" (catastrophisation, fear-avoidance, low job satisfaction) that predict chronicity
Pharmacological Management
Acute LBP
| Drug | Role | Notes |
|---|---|---|
| NSAIDs (ibuprofen 400–800 mg TDS; naproxen 250–500 mg BD) | First-line | Most equally efficacious; lowest dose possible; add PPI if GI risk |
| Muscle relaxants (methocarbamol 1000–1500 mg QDS; cyclobenzaprine 5–10 mg TDS; tizanidine 2–6 mg TDS) | Adjunct for muscle spasm | Short-term only; cause sedation; no additional benefit when combined with NSAIDs |
| Paracetamol (acetaminophen) | Not recommended | Recent high-quality evidence shows no significant benefit for LBP; no longer first-line |
| Opioids | Reserve for moderate–severe pain, limited 3-day course only | Not first-line; guidelines do not recommend for acute LBP; risk of dependency |
| Systemic corticosteroids | Not indicated for nonspecific LBP | No benefit for axial or nonspecific LBP |
| Benzodiazepines | Avoid | Greater side effects and addiction risk compared with other muscle relaxants |
Chronic LBP (>3 months)
| Drug | Role | Notes |
|---|---|---|
| NSAIDs | Still first-line pharmacotherapy | Lowest effective dose |
| Duloxetine (60 mg OD — SNRI) | Effective for chronic LBP | Good option especially with comorbid depression |
| Tricyclic antidepressants | Useful adjunct | Modest evidence |
| Gabapentinoids (gabapentin, pregabalin) | Insufficient evidence for axial or radicular LBP | Not routinely recommended |
| Opioids | Controversial; not demonstrated significant long-term benefit | Avoid in ED; if used — lowest dose, shortest duration, defined goals; avoid with benzodiazepines |
"Opioid analgesics should not be prescribed for chronic back pain from the ED." — Tintinalli's Emergency Medicine
Interventional Procedures
| Procedure | Indication |
|---|---|
| Transforaminal / interlaminar epidural corticosteroid injection | Radicular pain (not axial LBP) |
| Medial branch nerve blocks (diagnostic) | Suspected facetogenic axial LBP |
| Radiofrequency ablation (RFA) | Confirmed facetogenic pain (positive medial branch blocks) — months of relief |
| SI joint injection | Confirmed SI joint pain (20–35% of axial LBP) |
| Facet joint injection | No benefit for purely axial neck/low back pain |
Epidural corticosteroids are for radicular symptoms only — they have no role in nonspecific axial back pain.
Surgical Management
Referral to a spine surgeon is appropriate when:
| Indication | Procedure |
|---|---|
| Cauda equina syndrome | Emergency decompression |
| Radiculopathy not responding to 6 weeks of conservative treatment | Discectomy / microdiscectomy |
| Spinal stenosis with neurogenic claudication refractory to non-surgical treatment | Laminectomy / decompression |
| Vertebral instability (fracture, tumor, infection) | Stabilisation / fusion |
| Discogenic pain failing rehabilitation | Lumbar spinal fusion or disc replacement |
| Cord compression / myelopathy | Decompression ± fusion |
RCT evidence shows lumbar spinal fusion for non-radicular degenerative LBP is only modestly helpful compared with no treatment and not beneficial compared with an active physiotherapy programme. Surgery should not be offered for non-specific LBP without clear structural target.
When to Investigate
Do NOT investigate routinely
- Uncomplicated, nonspecific acute LBP without red flags
- Monitor for 4–6 weeks before pursuing further diagnostics
- Routine imaging is not associated with improved outcomes and findings are often incidental
Blood Tests — Indicated When:
| Test | Indication |
|---|---|
| FBC, ESR, CRP | Suspected infection (abscess, osteomyelitis, discitis) or malignancy |
| Serum calcium, ALP, LDH, SPEP | Suspected multiple myeloma or bone metastases |
| PSA | Suspected prostate cancer metastasis |
| Urinalysis ± urine pregnancy test | Suspected renal/GU cause; reproductive-age women |
| Coagulation studies | Suspected epidural haematoma; patients on anticoagulants |
| Blood cultures | Suspected spinal infection / epidural abscess |
Elevated ESR + CRP should prompt imaging — raises suspicion for spinal epidural abscess, osteomyelitis, discitis, or malignancy.
Imaging — When to Order:
| Modality | When Indicated | Notes |
|---|---|---|
| Plain X-ray (AP + lateral) | Suspected fracture (trauma, osteoporosis, age >70); Moderate indication: age >50 with first severe LBP | Rarely diagnostic alone; osteophytes/disc narrowing on X-ray are common with age and often incidental |
| MRI (spine) | Investigation of choice for: suspected malignancy, infection, cord compression, cauda equina syndrome, neurological deficit, radiculopathy not improving, LBP not improving after 4–6 weeks of conservative treatment | Soft tissue, nerve root, cord, disc detail |
| CT spine | Fracture characterisation; bony detail when MRI is contraindicated | Higher radiation; inferior soft tissue contrast |
| CT angiography / Ultrasound abdomen | Suspected AAA or aortic dissection | Urgent when clinically suspected |
| Bone scan (SPECT) | Suspected spondylolysis (especially young athletes); occult metastases when MRI not possible | |
| CT-guided biopsy | Suspected spinal infection or tumour after imaging |
Summary: Imaging is indicated when:
- Any neurological deficit (motor, sensory, reflex, bowel/bladder)
- Red flags present (suspected malignancy, infection, fracture)
- No improvement after 4–6 weeks of adequate conservative treatment
- Considering interventional procedure or surgery (to identify target)
Radiculopathy — Additional Points
| Root | Pain | Motor Loss | Sensory Loss | Reflex Lost |
|---|---|---|---|---|
| L3 | Front of thigh | Hip flexion, knee extension | Anterior thigh, medial calf | Patellar |
| L4 | Front of leg | Knee extension | Around knee | Patellar |
| L5 | Lateral leg | Foot dorsiflexion | Web of big toe | None |
| S1 | Back of leg | Foot plantarflexion | Lateral foot | Achilles |
Prognosis
- 90% of acute LBP resolves within 3 months without specific intervention
- 50% will have recurrence within 1 year
- Risk factors for chronicity: obesity, low education, tobacco use, high initial pain severity, somatisation tendency, job dissatisfaction, heavy lifting at work, psychopathology
Sources: Harrison's Principles of Internal Medicine 22e (2025); Goldman-Cecil Medicine; Tintinalli's Emergency Medicine; Rosen's Emergency Medicine; Bailey & Love's Short Practice of Surgery 28e; Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.