I now have enough information for a thorough clinical analysis. Let me compile the full response.
Clinical Assessment
Patient Summary
56F, PE teacher, active lifestyle, no DM, prior hyperuricemia (medication stopped 1.5 years ago). Normal CBC. 3-month history of postprandial frequent motions (10-20 min after eating), solid to semi-solid, with a separate normal morning motion. No pain, no blood, no nocturnal diarrhea (unless eating at night), no weight change, no family history of colorectal cancer or IBD. Father had similar symptoms after age 60.
Most Likely Diagnosis: IBS-D (Irritable Bowel Syndrome, Diarrhea-Predominant) with an exaggerated Gastrocolic Reflex
Why This Fits
| Feature | This Patient | IBS-D Profile |
|---|
| Postprandial urgency/loose stool 10-20 min after meals | Yes | Classic - gastrocolic reflex |
| Preserved normal morning motion | Yes | Common in IBS-D |
| No blood, no nocturnal diarrhea | Yes | Absence of alarm features |
| Normal CBC | Yes | Expected |
| No weight loss | Yes | Expected |
| Solid to semi-solid (Bristol 5-6) | Yes | IBS-D stool pattern |
| Female, 56 years | Yes | IBS common in women; new onset at 50+ is a borderline alarm |
| Family history (father, similar symptoms) | Yes | Familial clustering known in IBS |
| Active lifestyle, moderate stress | Yes | Physical activity can augment GI motility |
| No pain during defecation | Partial mismatch (pain is the Rome IV hallmark) | See caveat below |
Important caveat - Rome IV criteria require recurrent abdominal pain. This patient does not clearly report pain. This means she may not meet strict Rome IV criteria for IBS. However, the pattern - frequent, exaggerated postprandial defecation with loose to semi-solid stool and no structural pathology - is best described clinically as a functional bowel disorder: exaggerated gastrocolic reflex / functional diarrhea, which sits on the same functional spectrum as IBS-D.
From Goldman-Cecil Medicine (26th ed.): "Postprandial symptoms, reported by about two thirds of patients, include abdominal pain, bloating, and flatulence. Meal-related symptoms are often triggered by larger meals, foods rich in carbohydrates or fats, coffee, alcohol, and spicy foods." - Goldman-Cecil Medicine, IBS Chapter
The gastrocolic reflex (colonic response to gastric distension) is physiologically normal but is exaggerated in functional bowel disorders - it triggers urgency and loose stool within 10-30 minutes of eating, exactly as seen here.
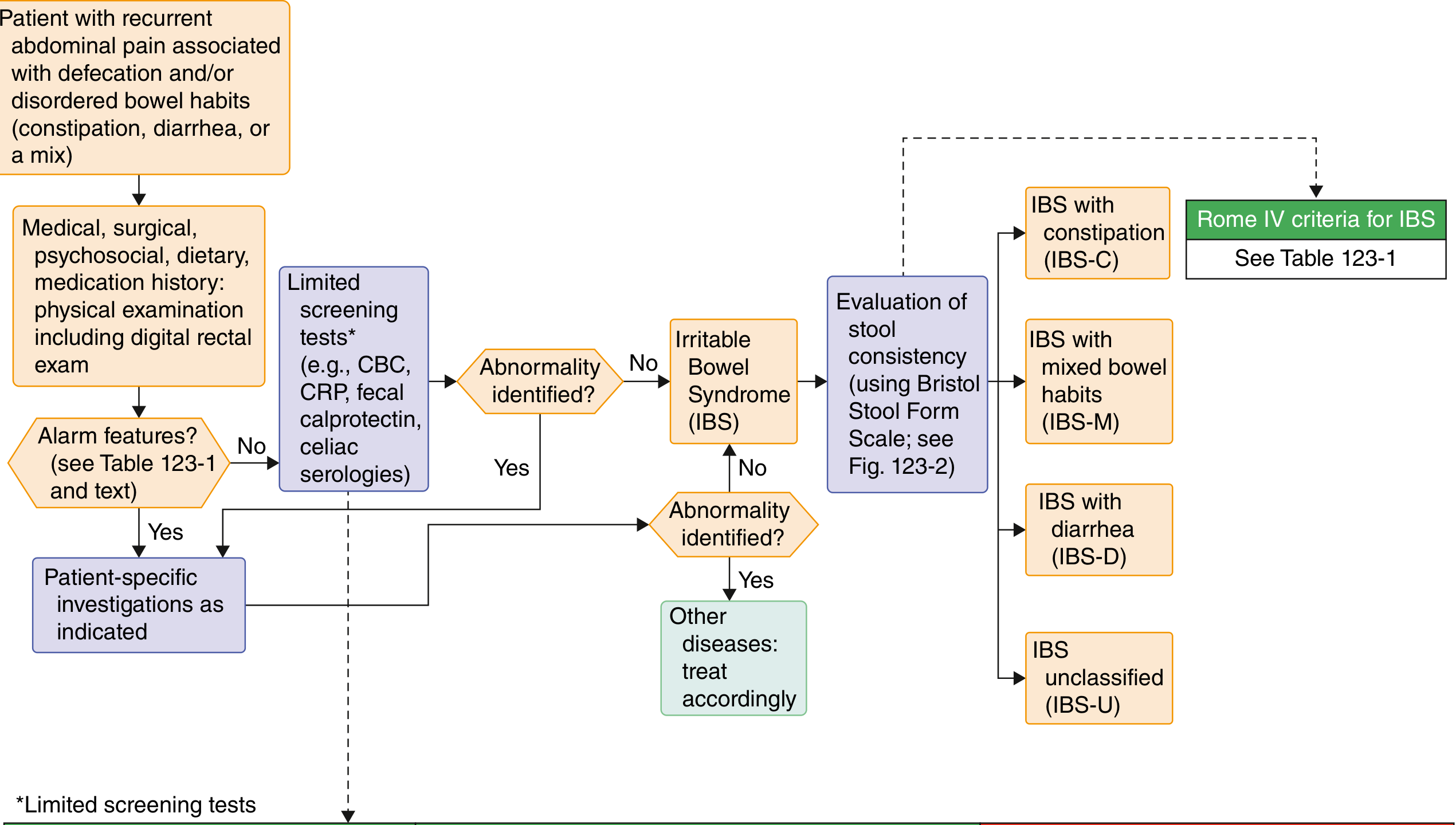
Diagnostic Algorithm
IBS diagnostic algorithm - Goldman-Cecil Medicine
Alarm Features Check (Rome IV Table 123-1)
| Alarm Feature | Present? |
|---|
| New onset at age ≥50 | Borderline - she is 56, onset at 56 |
| Unintentional weight loss | No |
| Hematochezia/melena | No |
| Nocturnal diarrhea (unprovoked) | No |
| Anemia (CBC abnormal) | No |
| Palpable mass/lymphadenopathy | Not reported |
| Family history of CRC/IBD/celiac | No |
One borderline flag: new onset at 56 years old. This warrants a colonoscopy to rule out organic pathology before confidently labeling this as functional.
Recommended Workup
Per Goldman-Cecil Medicine (Table 123-2):
Generally recommended:
- CBC - already done, normal ✓
- C-reactive protein (CRP) - to screen for occult inflammation
- Fecal calprotectin / lactoferrin - sensitive marker for intestinal inflammation (IBD, microscopic colitis)
- Celiac serology - IgA anti-tissue transglutaminase + total IgA (celiac can mimic this presentation perfectly)
- Colonoscopy - indicated here given new onset at age 56 (above the ≥50 threshold). If colonoscopy is done, random biopsies of the colon should be taken to exclude microscopic colitis / collagenous colitis, which is common in middle-aged women and causes exactly this pattern (painless, watery-to-loose postprandial stool, normal-looking mucosa)
- TSH - thyroid dysfunction (hyperthyroidism) can cause accelerated GI transit
- Stool for ova, parasites, and Giardia antigen (especially if any travel history)
Consider also:
- Serum uric acid - she stopped her medication 1.5 years ago; worth checking if gout/hyperuricemia has returned, though not directly relevant to GI symptoms
- Fasting blood glucose / HbA1c - diabetic autonomic diarrhea is unlikely given no DM history, but worth baseline screening at this age
Differential Diagnoses to Exclude
| Condition | Why Consider | Distinguishing Feature |
|---|
| Microscopic colitis | Middle-aged woman, painless postprandial loose stool, normal colonoscopy appearance | Diagnosed only on biopsy |
| Celiac disease | Can be asymptomatic or atypical, postprandial pattern, female | Serology + duodenal biopsy |
| Bile acid malabsorption | Postprandial watery/loose stool, exaggerated gastrocolic reflex | SeHCAT scan or empirical cholestyramine trial |
| Early colorectal neoplasm | New onset at 56, family history (father had similar GI symptoms late in life) | Colonoscopy |
| Hyperthyroidism | Can accelerate GI motility, active energetic woman | TSH |
| SIBO (Small Intestinal Bacterial Overgrowth) | Bloating, postprandial loose stool | Hydrogen breath test |
| IBD (early) | Though no blood or nocturnal symptoms, early IBD can be subtle | CRP, fecal calprotectin, colonoscopy |
Note on the father's history: The father had similar symptoms after age 60. While this could represent familial IBS clustering, it could also suggest hereditary colorectal neoplasia risk. This is not alarming in isolation but reinforces the case for colonoscopy now.
Management (If Functional Bowel Disorder Confirmed)
First-Line: Dietary
- Food diary for 1-2 weeks to identify triggers (common culprits: large meals, high-fat food, caffeine, dairy, high-FODMAP foods)
- Low-FODMAP diet - most evidence-based dietary intervention for postprandial IBS-D symptoms (reduce fermentable carbohydrates: onions, garlic, wheat, legumes, certain fruits). Best supervised by a dietitian
- Reduce meal size - smaller, more frequent meals blunt the gastrocolic reflex
- Limit caffeine post-meals - caffeine potentiates the gastrocolic reflex significantly
Per Sleisenger & Fordtran's GI and Liver Disease: "Reducing caffeine consumption, particularly after meals, may help lessen postprandial urgency and diarrhea."
Second-Line: Pharmacological
- Antispasmodics (e.g., mebeverine, hyoscine, dicyclomine) - taken 30 minutes before meals to blunt the reflex
- Peppermint oil - useful for abdominal pain and global IBS symptoms, can also be taken before meals
- Soluble fiber (psyllium) - can help normalize stool consistency
- Probiotics - combination products reduce global symptoms in ~20% of IBS patients; particularly useful for bloating
- Loperamide - for episodes of urgency or frequent loose motions, but not for chronic daily use
- If no response: Rifaximin (gut-selective antibiotic, particularly for IBS-D with bloating/gas)
Lifestyle
- Regular meal timing - predictable eating patterns help regulate GI motility
- Being a PE teacher with an active lifestyle is actually protective long-term; vigorous exercise right after meals may worsen symptoms, so a brief post-meal rest is reasonable
- Adequate sleep - her 6+2 hour pattern is acceptable; napping is fine
Bottom Line
This patient most likely has a functional bowel disorder - exaggerated gastrocolic reflex, likely IBS-D spectrum or functional diarrhea - based on the 3-month postprandial pattern, preserved morning motion, normal CBC, no alarm features (except age of onset). She does not strictly meet Rome IV criteria due to absent pain, making "functional diarrhea" or "functional bowel disorder" the precise label.
The immediate priority is colonoscopy with random biopsies (given new onset at 56, above the screening threshold), plus celiac serology, CRP, fecal calprotectin, and TSH. If all return negative, dietary modification and antispasmodics before meals are the first treatment steps with a very reassuring prognosis.
- Goldman-Cecil Medicine (26th ed.), Ch. 123 - IBS
- Sleisenger & Fordtran's GI and Liver Disease, Supportive Measures & Diarrhea chapters