Give me a detailed information of lungs
Reading File
Finding Sources
Finding Sources
Searching the Web
lung anatomy physiology detailed overview lobes segments blood supply
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content from Murray & Nadel's Textbook of Respiratory Medicine and the histology textbook. Let me compile a thorough, well-organized answer.
The Lungs: Detailed Overview
Based primarily on Murray & Nadel's Textbook of Respiratory Medicine and Histology: A Text and Atlas (Ross & Pawlina), supplemented with current anatomical references.
1. Overview and Essential Functions
The lungs have two essential, interdependent functions:
- Gas exchange (ventilation-perfusion matching) - delivering O2 to the body and removing CO2 produced by cellular metabolism.
- Host defense - protecting against airborne pathogens, chemicals, and particulates.
Secondary functions include surfactant synthesis and recycling, mucociliary clearance, neuroendocrine signaling, and synthesis/secretion of molecules by epithelial and endothelial cells - all of which underscore the lung's central role in homeostasis.
- Murray & Nadel's Textbook of Respiratory Medicine, pp. 32-33
2. Gross Anatomy
Size and Weight
- In life, each human lung weighs approximately 450-500 g (total ~900-1000 g), of which nearly 40-50% is blood.
- At end-expiration (FRC), gas volume is about 2.5 L; at maximal inspiration (TLC), it may reach 6 L.
- Lung density varies from 0.30 g/mL at FRC to 0.14 g/mL at TLC - not uniform; ~1 g/mL near the hilum, ~0.1 g/mL peripherally.
- The height of the lungs at FRC is approximately 24 cm.
Shape and Position
- Pyramid-shaped, paired organs located in the thoracic cavity on either side of the mediastinum.
- Connected to the trachea by the right and left main bronchi.
- Inferiorly bordered by the diaphragm; enclosed by the pleurae which attach to the mediastinum.
- Suspended from the mediastinum by the lung root (a collection of structures entering and leaving each lung: main bronchus, pulmonary artery, two pulmonary veins, bronchial vessels, lymphatics, and nerves).
Lobes and Fissures
| Lung | Lobes | Fissures |
|---|---|---|
| Right | 3 (upper, middle, lower) | Oblique (major) + horizontal (minor) fissures |
| Left | 2 (upper, lower) | Oblique (major) fissure only |
The left lung is smaller due to the cardiac notch (an indentation accommodating the heart) and the lingula (a tongue-like projection of the left upper lobe).
Surfaces and Borders
- Costal surface - convex, faces the ribs
- Mediastinal surface - concave medially, contains the hilum
- Diaphragmatic surface (base) - concave, rests on the diaphragm
- Apex - projects 2-3 cm above the clavicle into the neck
Bronchopulmonary Segments
The lungs are divided into bronchopulmonary segments - independent structural and functional units each supplied by a segmental bronchus, artery, and vein. There are:
- Right lung: 10 segments
- Left lung: 8-10 segments (some fused)
These are surgically resectable units (segmentectomy) and clinically relevant for localizing disease (e.g., pneumonia, bronchiectasis, tumors).
3. The Airway Tree
The conducting airways form a branching system from the trachea to the terminal bronchioles (purely conducting, no gas exchange), then transition to the respiratory zone.
Trachea
- Cartilaginous and fibromuscular tube extending from the cricoid cartilage (~C6/C7) to the carina (~T4/T5).
- Bifurcates into right and left main bronchi at the carina.
- Right main bronchus: wider, shorter, more vertical (explains why foreign bodies and aspiration commonly go right).
Bronchi
The wall of a bronchus is composed of:
- Mucosa (pseudostratified columnar ciliated epithelium)
- Lamina propria (with lymphoid tissue)
- Smooth muscle (spiral bands)
- Submucosa (seromucous glands between cartilaginous plates)
- Cartilaginous plates (provide structural rigidity)
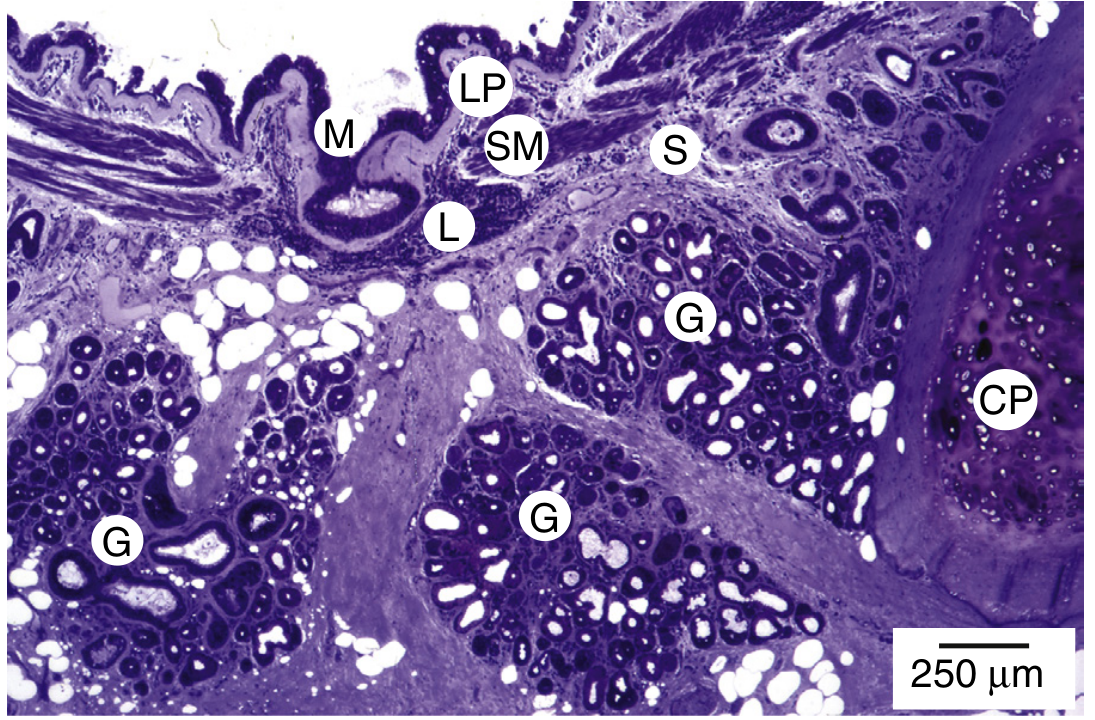
Figure: Wall structure of a bronchus. Seromucous glands (G) are located between spiral bands of smooth muscle (SM) and cartilaginous plates (CP). - Murray & Nadel's, p. 35
Bronchioles
- No cartilage; wall maintained by smooth muscle.
- Terminal bronchioles: the last purely conducting airways; lined by ciliated pseudostratified to simple columnar epithelium, with club cells (formerly Clara cells) that produce a surface-active agent aiding lung expansion.
- Respiratory bronchioles: transitional airways where gas exchange begins; wall alternates between thick regions (club cell epithelium + smooth muscle) and thin alveolar regions.
Alveolar Ducts and Sacs
- Alveolar ducts: passages lined entirely by rows of alveoli; rings of smooth muscle in interalveolar septa.
- Alveolar sacs: terminal enlarged spaces surrounded by clusters of alveoli.
4. The Terminal Respiratory Unit (TRU) / Acinus
The TRU (physiologist's acinus) consists of one respiratory bronchiole and all its alveolar ducts, alveolar sacs, and alveoli. Key facts:
-
Each TRU contains approximately 100 alveolar ducts and 2000 alveoli
-
At FRC, each TRU is ~5 mm diameter with a volume of ~0.02 mL
-
There are approximately 150,000 TRUs in adult human lungs
-
Gas-phase diffusion is so rapid within a TRU that O2 and CO2 partial pressures are essentially uniform throughout the unit
-
Most disorders of oxygenation arise from ventilation-perfusion inequalities, not diffusion failure
-
Murray & Nadel's, p. 40
5. Alveoli: The Gas-Exchange Units
The lungs contain approximately 300-500 million alveoli, providing a total surface area of 50-70 m² (roughly the size of a tennis court) for gas exchange.
Alveolar Lining Cells
| Cell Type | Coverage | Function |
|---|---|---|
| Type I pneumocytes (AT1) | ~95% of alveolar surface | Extremely thin squamous cells; primary site of gas exchange |
| Type II pneumocytes (AT2) | ~5% of surface (more numerous by count) | Cuboidal; secrete pulmonary surfactant (reduces surface tension); progenitor cells for AT1 repair |
The Air-Blood Barrier
The path for O2 diffusion from alveolar air to red blood cells crosses:
- Alveolar epithelium (Type I cell)
- Fused basal laminae of epithelium and endothelium (thin side ~0.2-0.4 µm)
- Capillary endothelium
- Plasma
- Red blood cell membrane + intracellular cytoplasm
On the thick side of the barrier, elastin, collagen, and matrix separate the epithelium from the capillary endothelium - this side contributes less to gas exchange but provides structural support.
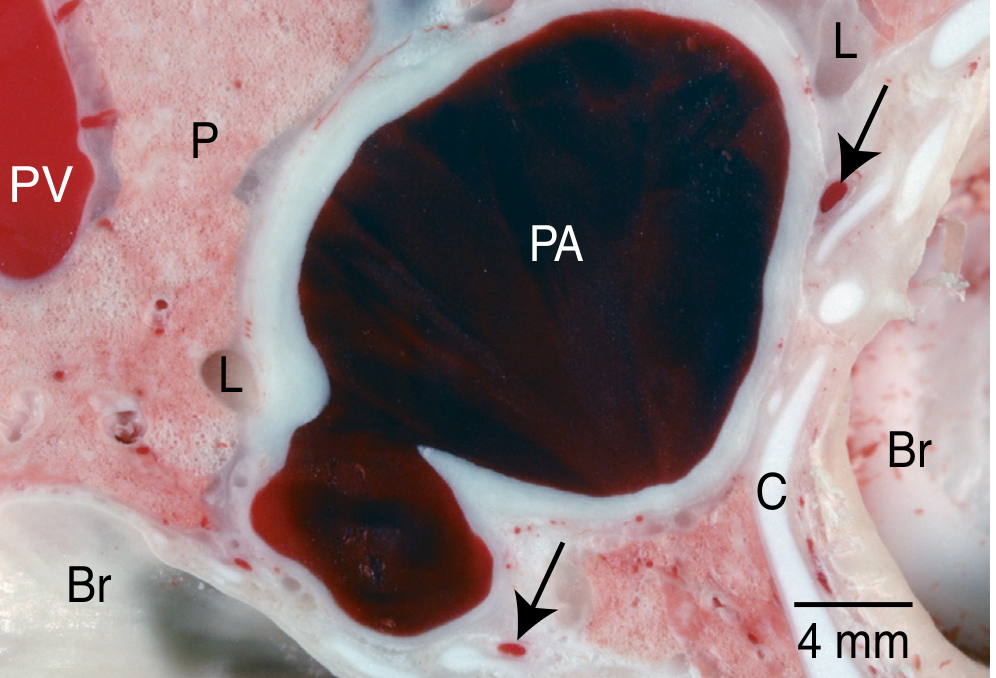
Figure: Levels of oxygenation in lung tissue. Pulmonary arterial (PA) blood is dark/deoxygenated; gas exchange across parenchyma results in oxygenated pulmonary venous (PV) blood. - Murray & Nadel's, p. 33
Pulmonary Surfactant
- Produced by AT2 cells; composed mainly of dipalmitoylphosphatidylcholine (DPPC) and surfactant proteins (SP-A, SP-B, SP-C, SP-D).
- Reduces surface tension at the air-liquid interface, preventing alveolar collapse during expiration.
- Deficiency causes Respiratory Distress Syndrome (RDS) in premature infants.
Interalveolar Septum
The tissue between adjacent alveoli; consists of:
- Alveolar epithelial cells + basal lamina
- Capillary endothelial cells + basal lamina
- Connective tissue elements (collagen, elastin, fibroblasts, macrophages, mast cells) between the two basal laminae
- This is the site of the air-blood barrier
6. Connective Tissue Framework
The lung's architecture rests on an "elastic continuum" - a weave of collagen and elastin fibers providing both structural support and elastic recoil.
- Collagen: provides tensile strength; prevents overdistension.
- Elastin: provides elastic recoil; enables the lung to spring back after expansion.
- Glycosaminoglycans and proteoglycans: fill the interstitial matrix with a gel-like structure; regulate epithelial cell phenotype and cytokine signaling.
Interstitial compartment organization:
- Axial (peribronchovascular) connective tissue: surrounds airways and pulmonary vessels; expands with interstitial edema first.
- Peripheral (subpleural) connective tissue: forms interlobular septa and visceral pleura.
- Parenchymal interstitium: alveolar walls.
7. Circulation: Dual Blood Supply
The lungs have a unique dual blood supply:
Pulmonary Circulation (functional)
- Pulmonary arteries: carry deoxygenated blood from the right ventricle at low pressure (~25/10 mmHg) to pulmonary capillaries around alveoli.
- Pulmonary capillaries (~8-10 µm diameter) form a dense network around alveoli for gas exchange.
- Pulmonary veins (4 total, 2 from each lung): carry oxygenated blood back to the left atrium.
- Blood pressure in pulmonary vessels increases at the rate of 1 cm H2O per cm height going down the lung, so vessels at the base are more distended than at the apex.
Bronchial Circulation (nutritive)
- Bronchial arteries (typically 2 left, 1 right) arise from the thoracic aorta.
- Supply the conducting airways (trachea to terminal bronchioles), visceral pleura, lymph nodes, and pulmonary nerves.
- Bronchial veins drain into the azygos/hemiazygos system.
8. Lymphatic Drainage
Two lymphatic plexuses:
- Superficial (subpleural) plexus: drains toward the hilum via interlobular septa.
- Deep (peribronchovascular) plexus: runs alongside bronchi and pulmonary arteries.
Lymph drains to hilar and mediastinal lymph nodes, then to the thoracic duct (left) or right lymphatic duct (right).
Lymphatic endothelial cells have discontinuous basement membranes (unlike blood capillaries which have continuous membranes), allowing easy uptake of large molecules and cells.
Initial lymphatics are concentrated in the loose-binding peribronchovascular connective tissue spaces - this is why interstitial edema fluid first accumulates here (it appears as peribronchial cuffing on chest X-ray).
9. Innervation
The lungs receive both autonomic and sensory innervation via the pulmonary plexus (anterior and posterior), formed by branches of the vagus nerve (CN X) and sympathetic trunk.
| Division | Effect on Airways | Effect on Vessels |
|---|---|---|
| Parasympathetic (vagal) | Bronchoconstriction; increased secretion | Vasodilation |
| Sympathetic | Bronchodilation; decreased secretion | Vasoconstriction |
| Non-adrenergic non-cholinergic (NANC) | Both inhibitory (VIP-mediated bronchodilation) and excitatory (substance P-mediated bronchoconstriction) | - |
Sensory fibers include:
- C-fibers (J-receptors): near alveolar capillaries; respond to congestion, chemical irritants, causing rapid shallow breathing.
- Stretch receptors (Hering-Breuer reflex): in airway smooth muscle; inhibit inspiration when lungs are over-inflated.
- Irritant receptors: in airway epithelium; trigger cough and bronchoconstriction.
Visceral pain from the lung is referred to the shoulder and neck (phrenic nerve territory, C3-C5) and the chest wall.
10. Pleura
The pleural cavity is formed by two serous membranes:
| Layer | Location | Subdivisions |
|---|---|---|
| Visceral pleura | Covers lung surface (including fissures) | - |
| Parietal pleura | Lines thoracic wall, diaphragm, mediastinum | Costal, diaphragmatic, mediastinal, cervical |
In life, the two layers are separated by only a few micrometers of pleural fluid (~5-15 mL total); this fluid acts as a lubricant and by surface tension, keeps the lung apposed to the chest wall.
Pleural recesses (potential spaces that expand during deep inspiration):
- Costodiaphragmatic recess: most clinically important; site of pleural effusion accumulation; used for thoracentesis.
- Costomediastinal recess: between the costal and mediastinal parietal pleura.
Pleural cells (mesothelial cells) are flat polygonal cells with long microvilli that increase surface area for pleural fluid absorption and provide a non-adhesive surface.
11. Cellular Anatomy: Key Cell Types
Airway Lining Cells
| Cell | Location | Function |
|---|---|---|
| Ciliated columnar cells | Trachea to respiratory bronchioles | Beat in coordinated waves to move mucus (mucociliary escalator) |
| Goblet cells | Trachea to bronchioles | Secrete mucus (gel layer) |
| Club cells (formerly Clara) | Terminal/respiratory bronchioles | Secrete surface-active material; detoxify inhaled substances; progenitor cells |
| Basal cells | Trachea and bronchi | Stem cells for airway epithelium |
| Neuroendocrine cells (PNEC) | Throughout airways | Secrete serotonin, bombesin; oxygen sensing |
Mesenchymal Cells
- Fibroblasts: produce extracellular matrix (collagen, elastin, glycosaminoglycans); highly heterogeneous - airway fibroblasts (collagen-rich) differ from alveolar fibroblasts (cytoskeletal-oriented).
- Myofibroblasts: key in secondary septum formation during alveologenesis; deposit elastin at septal tips; become fibrotic foci in IPF (idiopathic pulmonary fibrosis).
- Smooth muscle cells: two subtypes differing in origin and function; provide tone in airways (bronchoconstriction) and vessels.
- Pericytes: surround pulmonary capillaries.
Immune/Inflammatory Cells
- Alveolar macrophages (dust cells): primary phagocytes of the alveolar space; remove inhaled particles, bacteria, dead cells; first line of innate defense.
- Dendritic cells: antigen-presenting cells in airway epithelium and alveoli; bridge innate and adaptive immunity.
- Mast cells: in airway connective tissue; release histamine and leukotrienes in allergic/asthmatic responses.
- Lymphocytes: in bronchial-associated lymphoid tissue (BALT).
12. Molecular Anatomy: Key Molecules
- Surfactant proteins:
- SP-A, SP-D: hydrophilic; innate immune defense (opsonization of pathogens)
- SP-B, SP-C: hydrophobic; critical for surfactant film formation and function
- Extracellular matrix: collagen types I, III, IV; elastin; fibronectin; laminin; proteoglycans (heparan sulfate, versican, decorin)
- Tight junction proteins (claudins, occludins): maintain epithelial barrier integrity
- Aquaporins (especially AQP5 in AT1 cells): water transport across alveolar walls
- Ion channels (ENaC, CFTR): regulate fluid clearance from alveolar surface; CFTR mutations cause cystic fibrosis
13. Lung Volumes and Capacities (Reference Values)
| Parameter | Definition | Normal Value |
|---|---|---|
| Tidal Volume (TV) | Air moved per normal breath | ~500 mL |
| Inspiratory Reserve Volume (IRV) | Extra air above TV | ~3000 mL |
| Expiratory Reserve Volume (ERV) | Extra air below TV | ~1100 mL |
| Residual Volume (RV) | Air remaining after maximal expiration | ~1200 mL |
| Total Lung Capacity (TLC) | Total air at full inspiration | ~6000 mL |
| Functional Residual Capacity (FRC) | Air at end of normal expiration | ~2500 mL |
| Vital Capacity (VC) | Maximum air forcibly exhaled after max inspiration | ~4800 mL |
14. Clinical Correlations
| Condition | Anatomical/Physiological Basis |
|---|---|
| Pneumothorax | Air enters pleural space, disrupts the surface tension keeping lung apposed to chest wall |
| Pleural effusion | Fluid in costodiaphragmatic recess; blunts costophrenic angle on CXR |
| COPD/Emphysema | Destruction of alveolar walls reduces gas-exchange surface area; loss of elastin destroys recoil |
| Asthma | Smooth muscle hypertrophy + mucus hypersecretion + airway inflammation causes reversible obstruction |
| Pulmonary fibrosis (IPF) | Myofibroblast activation lays down excess collagen; stiffens lung; restricts volume |
| RDS (neonatal) | Surfactant deficiency (AT2 immaturity in prematurity) causes diffuse alveolar collapse |
| Cystic fibrosis | CFTR mutation impairs Cl-/water secretion; thick mucus accumulates; recurrent infections |
| Pulmonary embolism | Blocked pulmonary artery branch creates dead space (ventilated but not perfused) |
| Lung cancer | Arises from airway epithelial cells or AT2 cells; bronchopulmonary segments guide surgical resection |
| Aspiration pneumonia | Right lower lobe most commonly affected (wider, more vertical right main bronchus) |
Summary
The lungs are architecturally elegant organs whose entire design serves two master functions: gas exchange and host defense. From the branching airway tree (ensuring all 300+ million alveoli receive fresh air) to the gossamer-thin air-blood barrier (enabling millisecond-fast O2/CO2 diffusion), from the dual blood supply to the innate immune sentinels in the alveolar space, every structural feature reflects a precise functional purpose.
Source: Murray & Nadel's Textbook of Respiratory Medicine, 2-Volume Set, Section A - Anatomy, Chapter 1; Histology: A Text and Atlas (Ross & Pawlina), Chapter on Respiratory System.
This is a shared conversation. Sign in to Orris to start your own chat.