Answer each question
cd /home/daytona/workspace/attachments/f3a7b748-4398-4603-810f-87b6f8d7a170/ && python3 -c " import subprocess result = subprocess.run(['antiword', 'practical skills 2026.doc'], capture_output=True, text=True) print(result.stdout[:5000]) print('STDERR:', result.stderr[:500]) "
cd "/home/daytona/workspace/attachments/f3a7b748-4398-4603-810f-87b6f8d7a170/" && python3 -c " import subprocess # Try libreoffice conversion result = subprocess.run(['libreoffice', '--headless', '--convert-to', 'txt', 'practical skills 2026.doc', '--outdir', '/home/daytona/workspace/'], capture_output=True, text=True, timeout=60) print('STDOUT:', result.stdout) print('STDERR:', result.stderr[:500]) print('Return code:', result.returncode) "
cd "/home/daytona/workspace/attachments/f3a7b748-4398-4603-810f-87b6f8d7a170/" && python3 -c " import subprocess # Try docx conversion result = subprocess.run(['libreoffice', '--headless', '--convert-to', 'docx', 'practical skills 2026.doc', '--outdir', '/home/daytona/workspace/'], capture_output=True, text=True, timeout=60) print('STDOUT:', result.stdout) print('STDERR:', result.stderr[:500]) print('Return code:', result.returncode) "
# Try extracting text directly from the binary doc file with python-docx or olefile python3 -c " import olefile import os path = '/home/daytona/workspace/attachments/f3a7b748-4398-4603-810f-87b6f8d7a170/practical skills 2026.doc' ole = olefile.OleFileIO(path) # Word document streams if ole.exists('WordDocument'): stream = ole.openstream('WordDocument') data = stream.read() print('WordDocument stream size:', len(data)) # Try to get text from the 0Table or 1Table stream if ole.exists('1Table'): stream = ole.openstream('1Table') data1 = stream.read() print('1Table stream size:', len(data1)) # decode stream = ole.openstream('WordDocument') raw = stream.read() # Extract ASCII text import re text = raw.decode('latin-1', errors='replace') # Find readable text - look for sequences of printable chars readable = re.findall(r'[ -~\n\r\t]{4,}', text) for r in readable[:100]: if len(r) > 8: print(repr(r)) "
python3 -c " import re, struct path = '/home/daytona/workspace/attachments/f3a7b748-4398-4603-810f-87b6f8d7a170/practical skills 2026.doc' with open(path, 'rb') as f: data = f.read() # Extract readable text sequences (latin-1 encoded) text = data.decode('latin-1', errors='replace') readable = re.findall(r'[A-Za-z0-9 .,;:!?()\-\'\"]{10,}', text) for r in readable: if any(c.isalpha() for c in r): print(r) " 2>/dev/null | head -200
| # | Topic |
|---|---|
| 1 | Action potential graph + phases + ionic mechanism |
| 2 | Excitability changes during AP + refractory periods (ARP, RRP) |
| 3 | AP propagation - myelinated (saltatory) vs. non-myelinated (continuous) |
| 4 | Neuromuscular junction scheme + synaptic transmission steps |
| 5 | Single twitch vs. tetanic contraction curves |
| 6 | Mechanism of muscular contraction and relaxation (Ca²⁺, troponin, cross-bridge cycling) |
| 7 | Spinal cord reflex arch (5 components) |
| 8 | Pre- and postsynaptic inhibition in CNS |
| 9 | Autonomic reflex arch - sympathetic and parasympathetic |
| 10 | Protein hormone action (GPCR/RTK, cAMP, second messengers) |
| 11 | Steroid hormone action (nuclear receptor, gene expression) |
| 12 | Hypothalamic-pituitary axis (HPT axis example + negative feedback) |
| 13 | Blood test interpretation (CBC reference ranges) |
| 14 | ABO and Rh blood typing principles |
| 15 | Ventricular cardiomyocyte AP - phases 0-4 + ionic basis |
| 16 | Pacemaker cell AP - If current, T-type Ca²⁺, spontaneous depolarization |
| 17 | Cardiac conduction system + frequencies + conduction velocities |
| 18 | ECG pacemaker identification criteria |
| 19 | ECG heart rate calculation + cardiac cycle duration |
| 20 | Electrical axis determination in frontal plane |
| 21 | Sphygmogram curve + phases (anacrotic, dicrotic notch, catacrotic) |
| 22 | Phlebogram curve + a, c, x, v, y waves |
| 23 | External respiration methods (spirometry, FEV₁, plethysmography, DLCO, ABG) |
| 24 | RAAS scheme + kidney's role in BP maintenance |
| 25 | Osmotic pressure regulation feedback loop (ADH, osmoreceptors) |
| 26 | Sensory system structural and functional organization |
| 27 | Conditioned reflex rules (Pavlov) + stages of development |
| 28 | Thermoregulation at HIGH temperature (sweating, vasodilation) |
| 29 | Thermoregulation at LOW temperature (shivering, vasoconstriction, thermogenesis) |
| 30 | Conditioned vs. unconditioned salivary reflexes |
| 31 | Gamma loop scheme + alpha vs. gamma motoneuron characteristics |
| 32 | Hans Selye's GAS - 3 stages + hormonal roles |
Give realistic diagrams from testbooks
Q1 & Q2 — Nerve Action Potential + Ionic Conductances + Refractory Periods
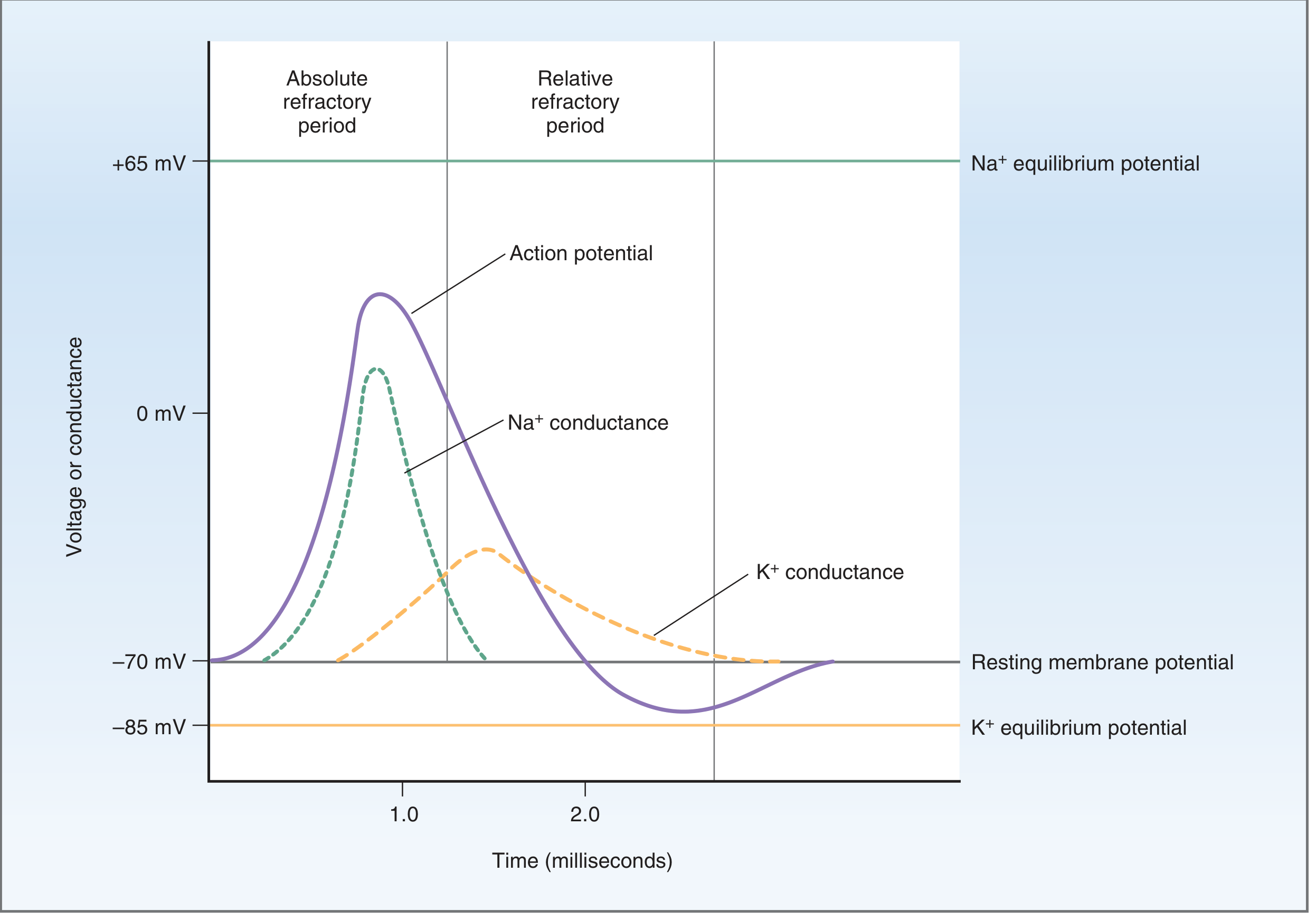
Shows the AP waveform (purple), Na⁺ conductance spike (green dashed), K⁺ conductance curve (orange dashed), equilibrium potentials, resting potential (-70 mV), undershoot, and both the absolute and relative refractory periods marked above.
Q1 (continued) — Na⁺ Channel Gate States
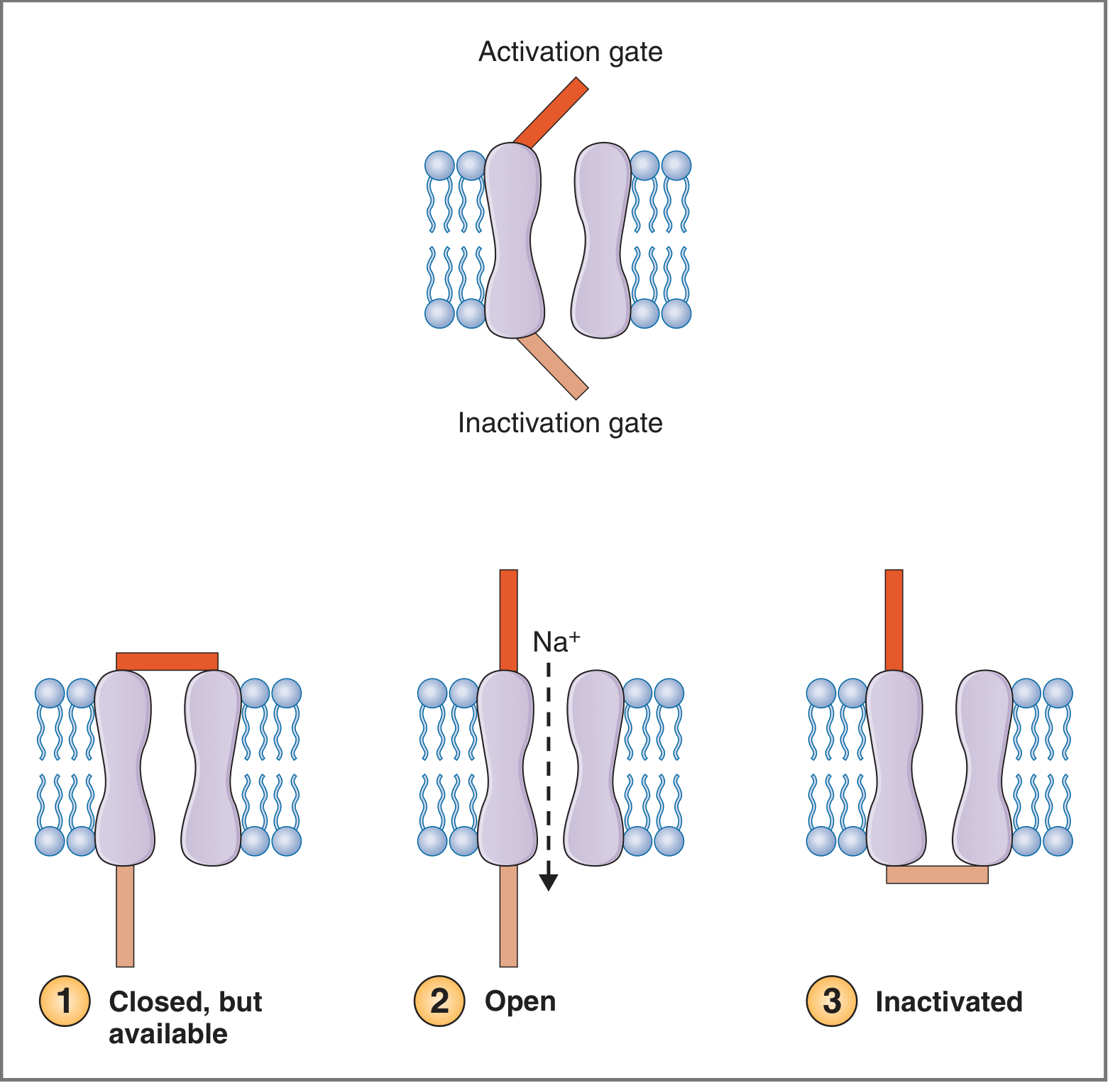
The three states of the voltage-gated Na⁺ channel: (1) Closed but available (resting) - activation gate closed, inactivation gate open; (2) Open (upstroke) - both gates open, Na⁺ flows in; (3) Inactivated (repolarization) - inactivation gate closed, channel non-conducting. This directly explains the ARP.
Q4 — Neuromuscular Junction Structure
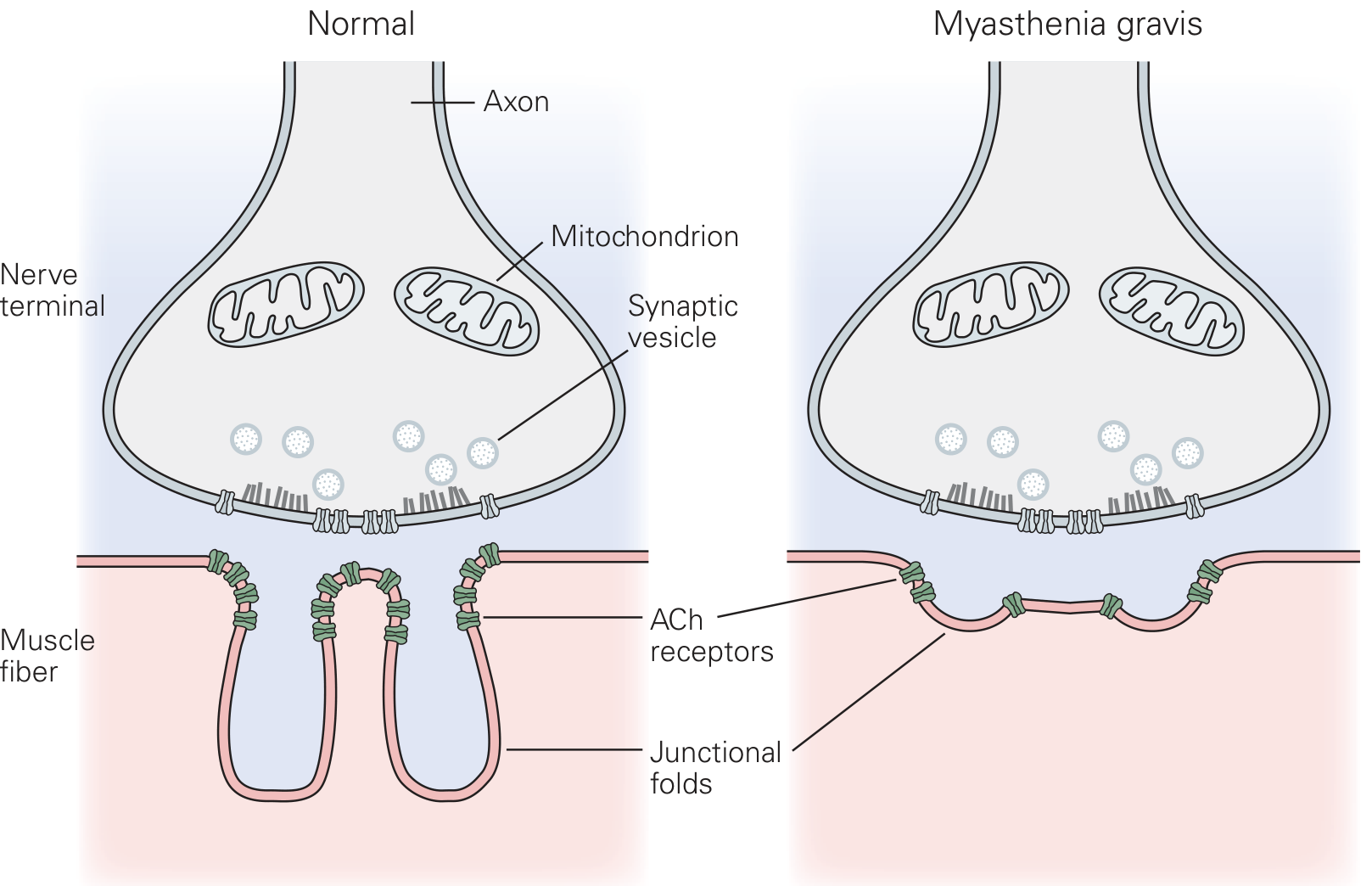
The normal NMJ (left): axon terminal contains mitochondria and synaptic vesicles (ACh); active zones release ACh into the cleft; nicotinic ACh receptors cluster at the peaks of junctional folds on the muscle fiber membrane. AChE in the cleft hydrolyzes ACh.
Q6 — Mechanism of Muscular Contraction (Cross-Bridge Cycle)
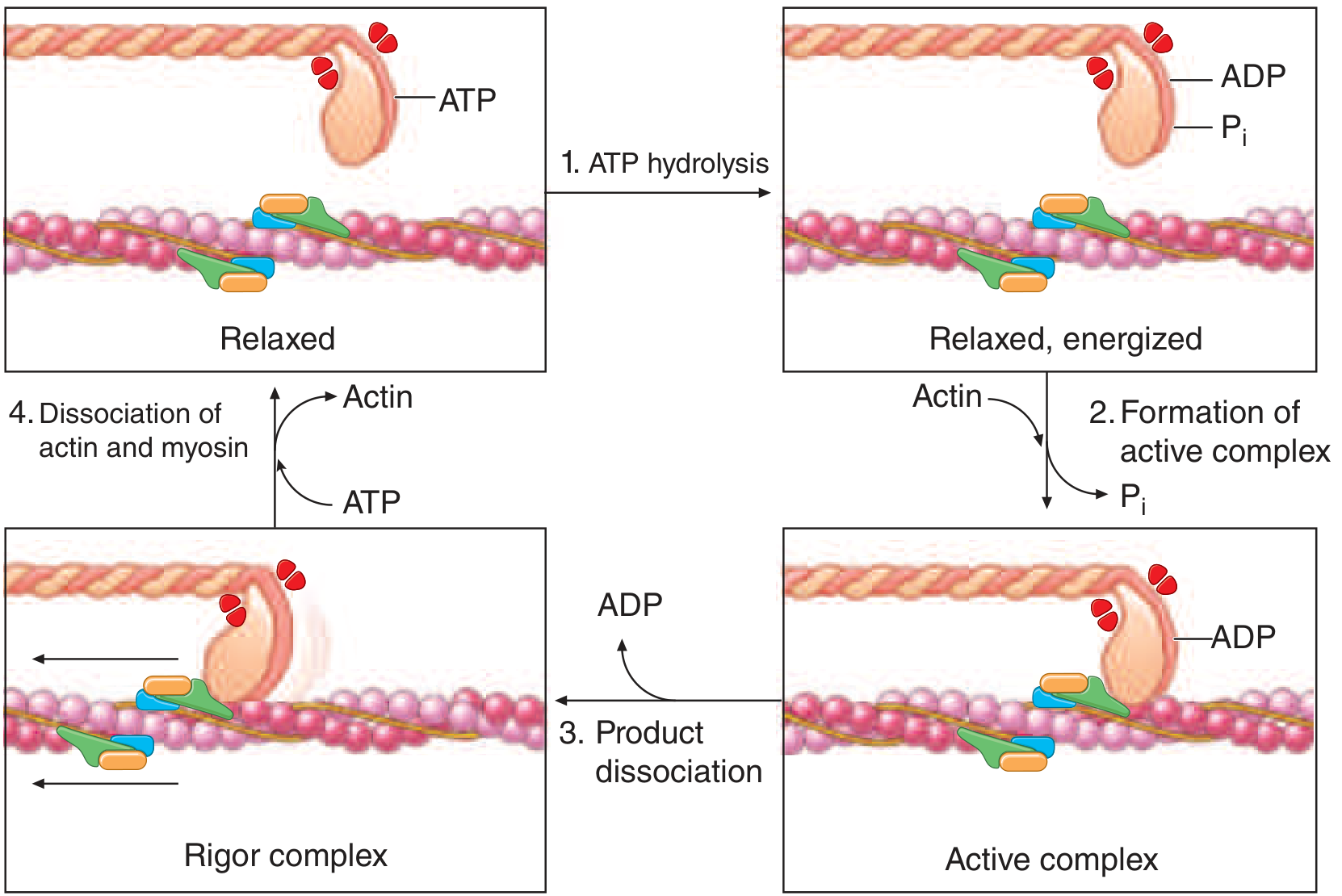
The 4-step cross-bridge cycle:
- Relaxed → ATP on myosin head dissociates thick/thin filaments
- Step 1 (ATP hydrolysis): Myosin head "re-cocked", energized (ADP + Pi)
- Step 2 (Active complex): Ca²⁺ exposes actin sites; myosin binds actin, Pi released
- Step 3 (Power stroke): ADP released; myosin head pivots → filaments slide → force
- Step 4 (Rigor): New ATP binds → cross-bridge detaches → cycle repeats
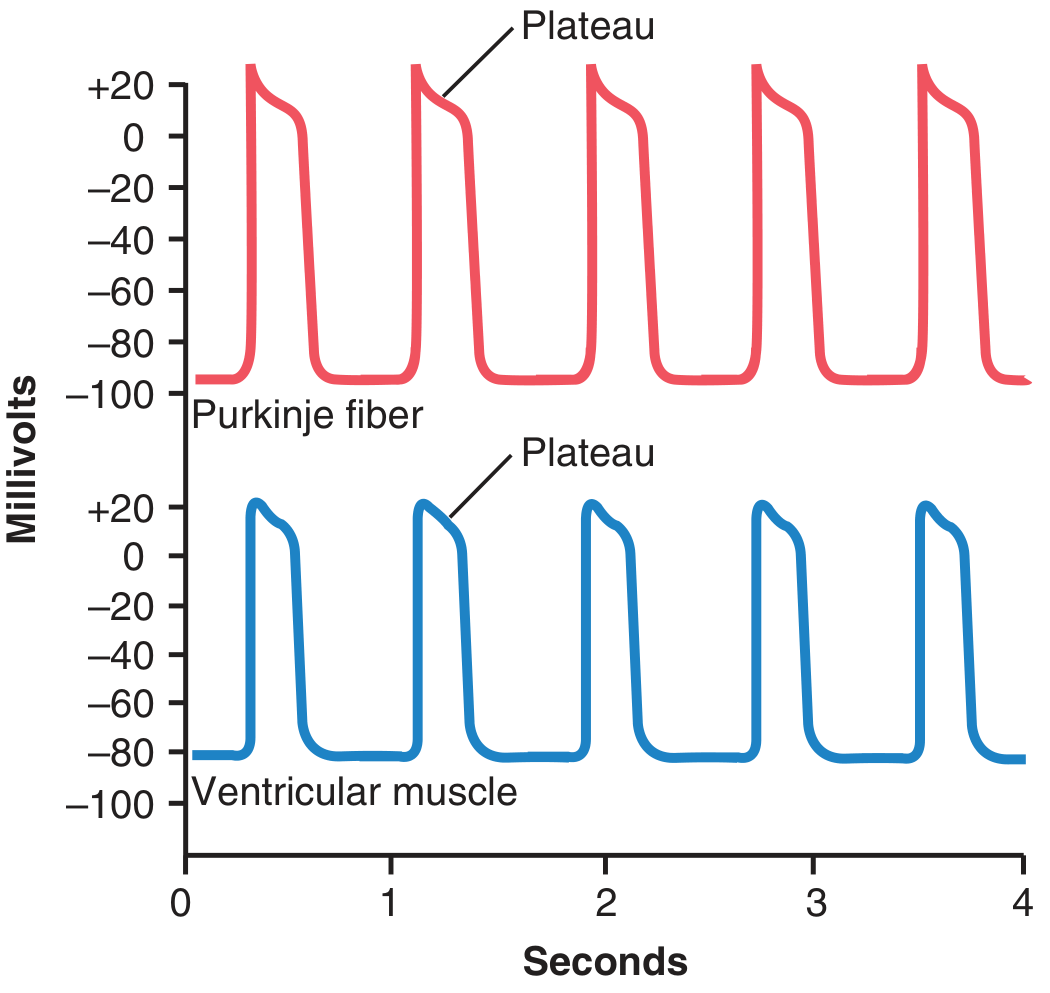
Q15 — Cardiac Ventricular Action Potential (Phases 0-4 + Ionic Currents)
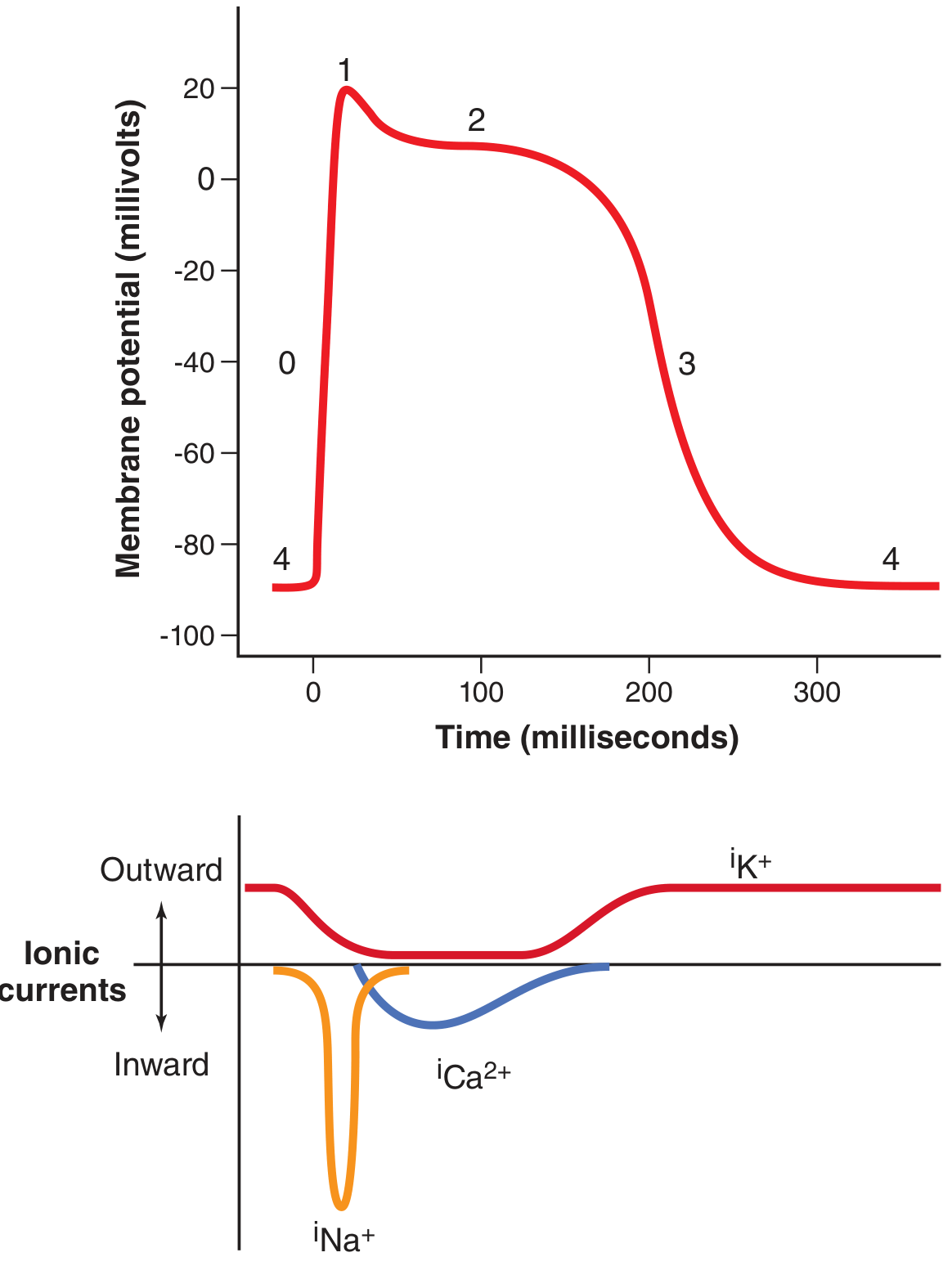
Phase 0: Fast Na⁺ influx (iNa) → rapid upstroke to +20 mV Phase 1: Na⁺ channels inactivate → brief early repolarization Phase 2 (Plateau): L-type Ca²⁺ influx (iCa²⁺) balanced by K⁺ efflux → flat plateau ~200 ms Phase 3: Ca²⁺ channels close; K⁺ channels (iK⁺) fully open → rapid repolarization Phase 4: Resting at -85 to -90 mV; iK⁺ (inward rectifier) maintains
Q16 — Pacemaker AP (SA Node) vs. Ventricular AP - Side by Side
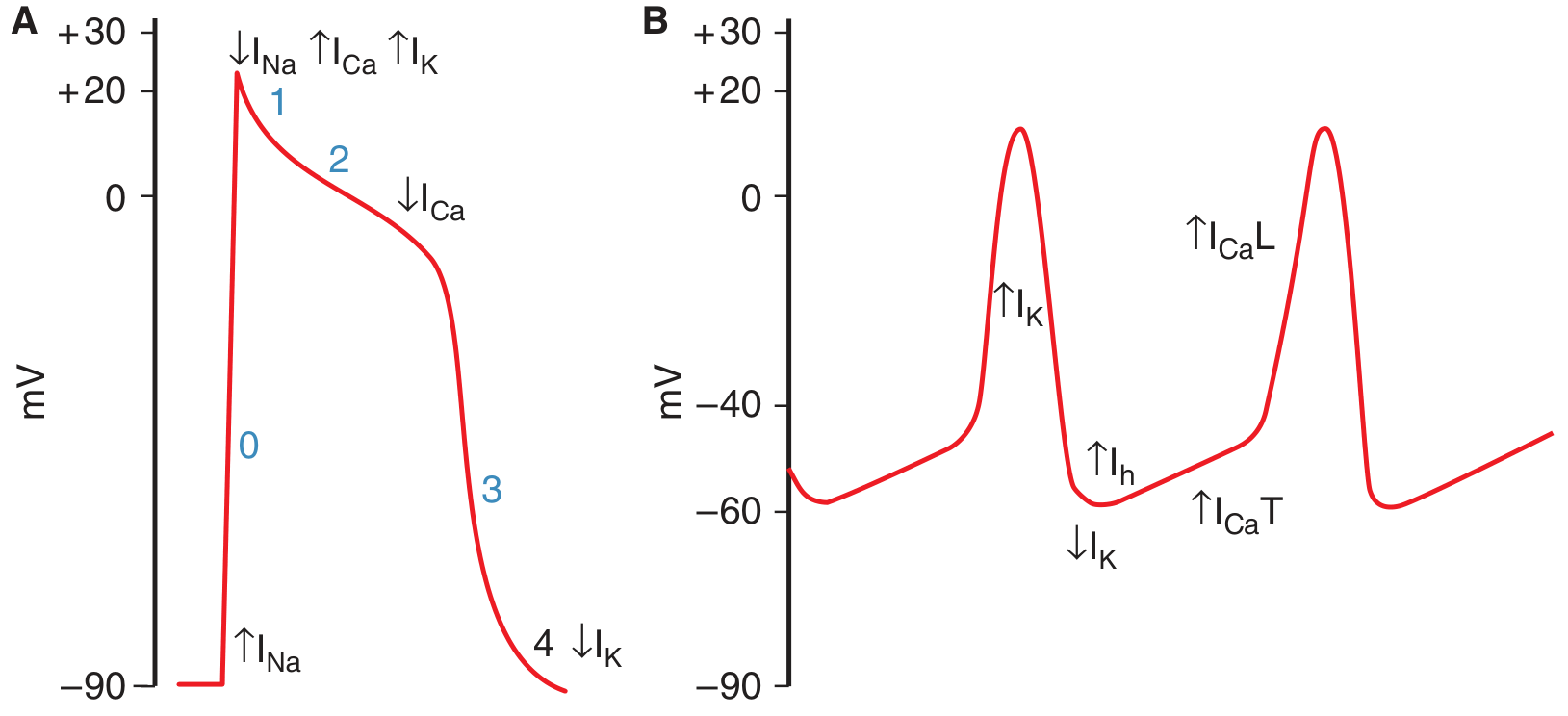
Panel A (ventricular): Phases 0-4 with ion current labels (↑INa = upstroke; ↑ICa + ↑IK = plateau; ↓IK = resting at -90 mV)Panel B (pacemaker - SA node): No stable resting potential - instead a slow spontaneous depolarization (pacemaker potential) from -60 mV to threshold:
- ↑Ih (HCN "funny" current): inward Na⁺ current activated by hyperpolarization → initial slow drift upward
- ↓IK: K⁺ channels gradually close → less outward current → further depolarization
- ↑ICaT (T-type Ca²⁺): activates near -50 mV → accelerates depolarization to threshold
- ↑ICaL (L-type Ca²⁺): carries the upstroke (no fast Na⁺ channels in nodal cells!)
Q17 — Cardiac Conduction System
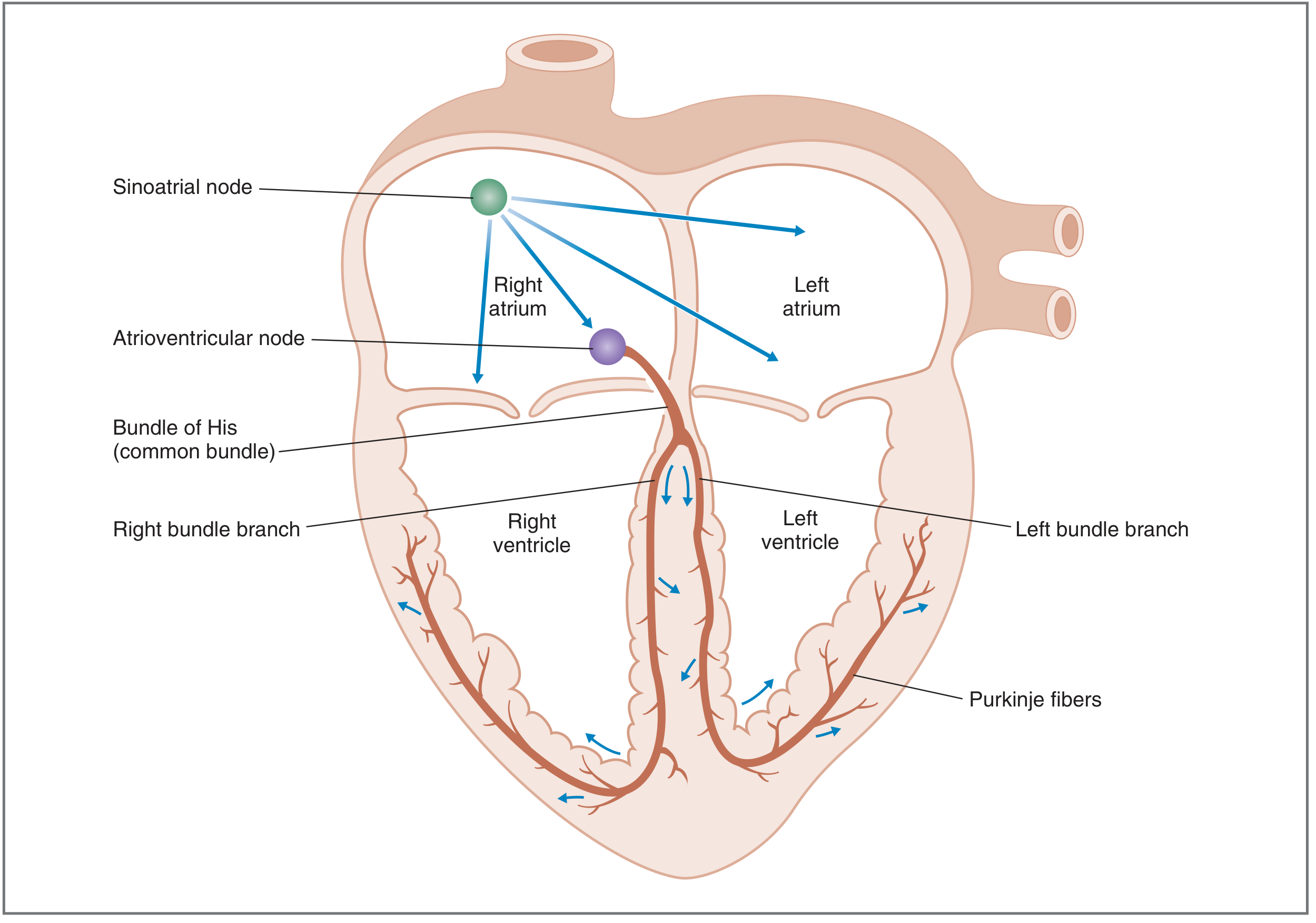
Activation sequence: SA node (right atrium) → spreads through both atria via internodal tracts → AV node (slow conduction - delay allows ventricular filling) → Bundle of His → Right & Left bundle branches → Purkinje fibers → ventricular myocardium (endocardium to epicardium)
| Diagram | Source |
|---|---|
| Q1/Q2: Nerve AP + conductances + refractory periods | Costanzo Physiology 7e |
| Q1: Na⁺ channel gate states | Costanzo Physiology 7e |
| Q4: Neuromuscular junction | Kandel - Principles of Neural Science 6e |
| Q6: Cross-bridge contraction cycle | Harrison's Internal Medicine 22e |
| Q15: Cardiac ventricular AP + ionic currents | Guyton & Hall Medical Physiology |
| Q16: Ventricular vs. pacemaker AP comparison | Ganong's Medical Physiology 26e |
| Q17: Cardiac conduction system | Costanzo Physiology 7e |
I need for all questions
Textbook Diagrams for All 32 Practical Skills Questions
Q1 — Action Potential Graph + Ionic Conductances
- AP rises from -70 mV → peak near +40 mV → repolarizes → undershoot to ~-80 mV
- Na⁺ conductance peaks first (upstroke), then falls
- K⁺ conductance rises later, causing repolarization and undershoot
- Absolute refractory period (ARP): Na⁺ channels inactivated - no new AP possible
- Relative refractory period (RRP): partial recovery - suprathreshold stimulus needed
Q1 (continued) — Na⁺ Channel Gate States (Ionic Mechanism)
Q2 — Refractory Periods
- ARP = during upstroke + most of repolarization (Na⁺ channels in state 3/inactivated)
- RRP = after return to resting potential, while K⁺ conductance still slightly elevated (hyperpolarized undershoot)
- During ARP: zero excitability, no AP possible at any stimulus strength
- During RRP: reduced excitability, supranormal stimulus required; AP will be smaller
Q3 — AP Propagation: Myelinated (Saltatory) vs. Non-myelinated
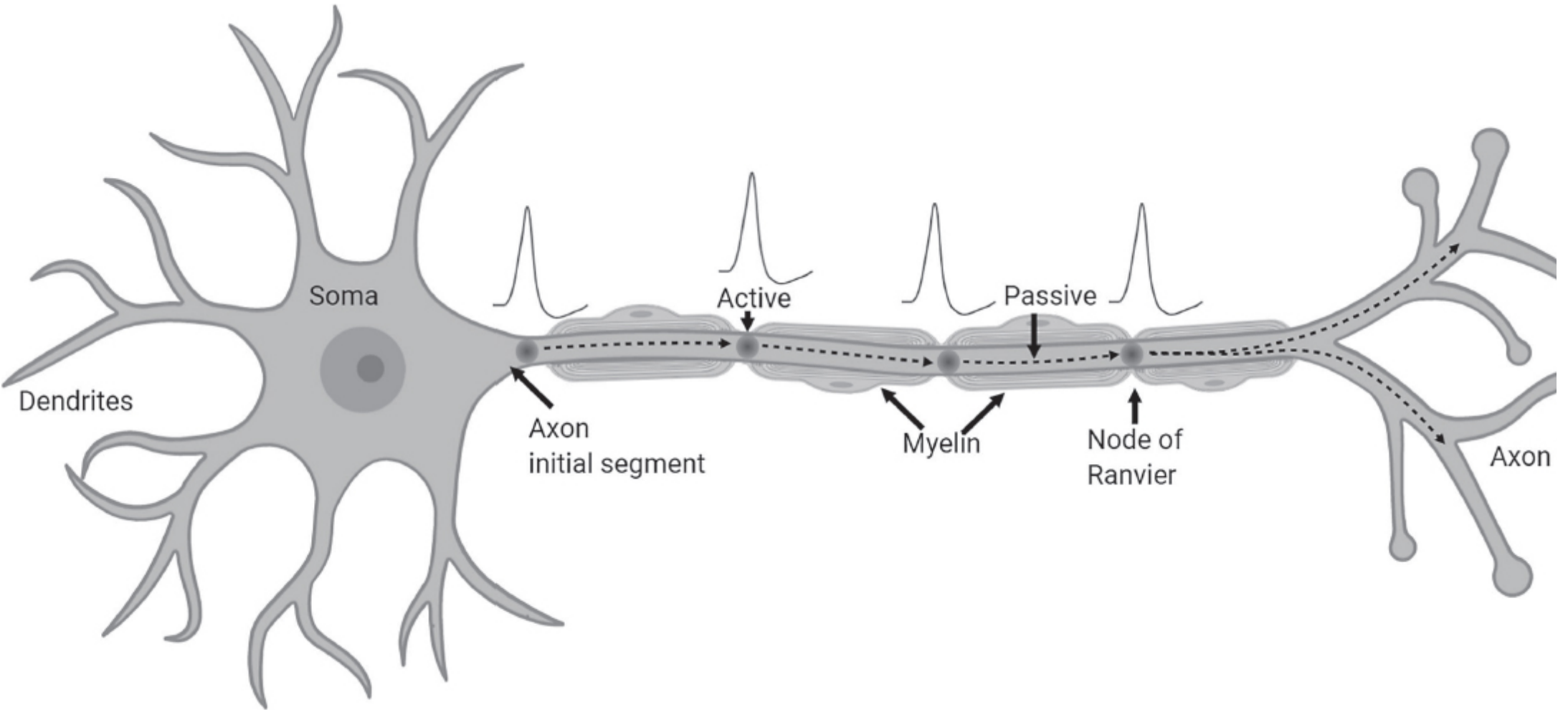
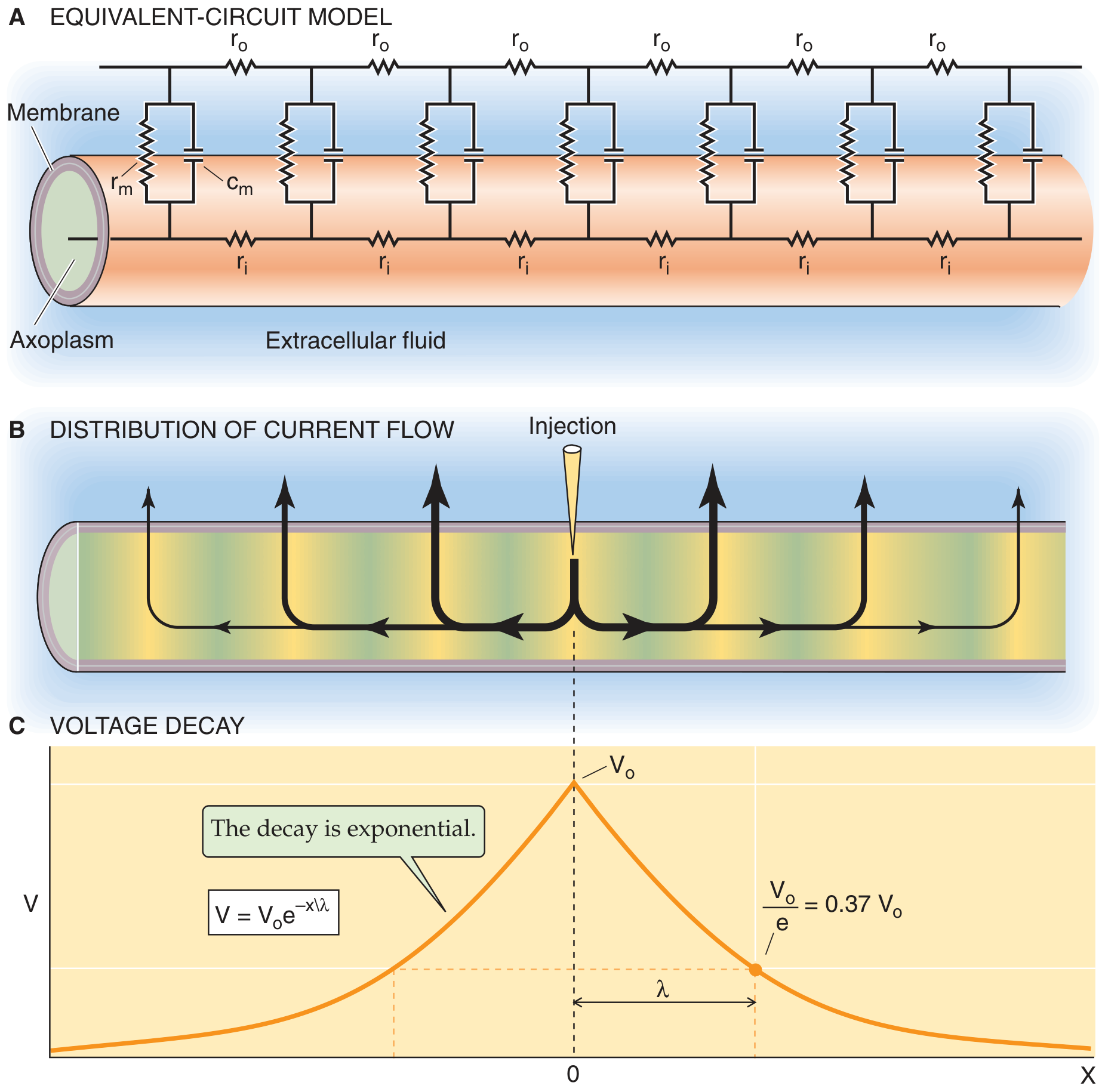
- Non-myelinated: Current leaks continuously across membrane at every point → slow, energy-costly (0.3-2 m/s). Decremental passive spread is regenerated at each point.
- Myelinated (saltatory): Myelin ↑membrane resistance + ↓membrane capacitance → current forced to flow along axoplasm and "jump" node to node. AP regenerated only at nodes of Ranvier → fast (up to 130 m/s), energy-efficient.
Q4 — Neuromuscular Junction
- AP reaches terminal → voltage-gated Ca²⁺ channels open → Ca²⁺ influx
- Ca²⁺ triggers exocytosis of ACh vesicles into synaptic cleft
- ACh binds nicotinic receptors on junctional folds → Na⁺/K⁺ channels open → EPP
- EPP spreads → AP in muscle → contraction
- AChE in cleft rapidly hydrolyzes ACh → signal terminated
Q5 — Single Twitch and Tetanus

- Single twitch: one stimulus → brief Ca²⁺ release → force rises and falls completely
- Incomplete tetanus: stimuli before full relaxation → summation → undulating elevated force
- Complete tetanus: high-frequency stimuli → Ca²⁺ continuously elevated → maximal smooth force (~4x single twitch)
Q6 — Mechanism of Muscular Contraction (Cross-Bridge Cycle)
- ATP hydrolysis: Myosin re-cocked, energized with ADP + Pi
- Active complex: Ca²⁺ binds troponin C → tropomyosin shifts → actin binding sites exposed → myosin head attaches to actin; Pi released
- Power stroke: ADP released → myosin head pivots → thin filament pulled → force/shortening (rigor complex)
- Detachment: New ATP binds → cross-bridge detaches → cycle repeats
Q7 — Spinal Cord Reflex Arc (Knee-Jerk / Stretch Reflex)
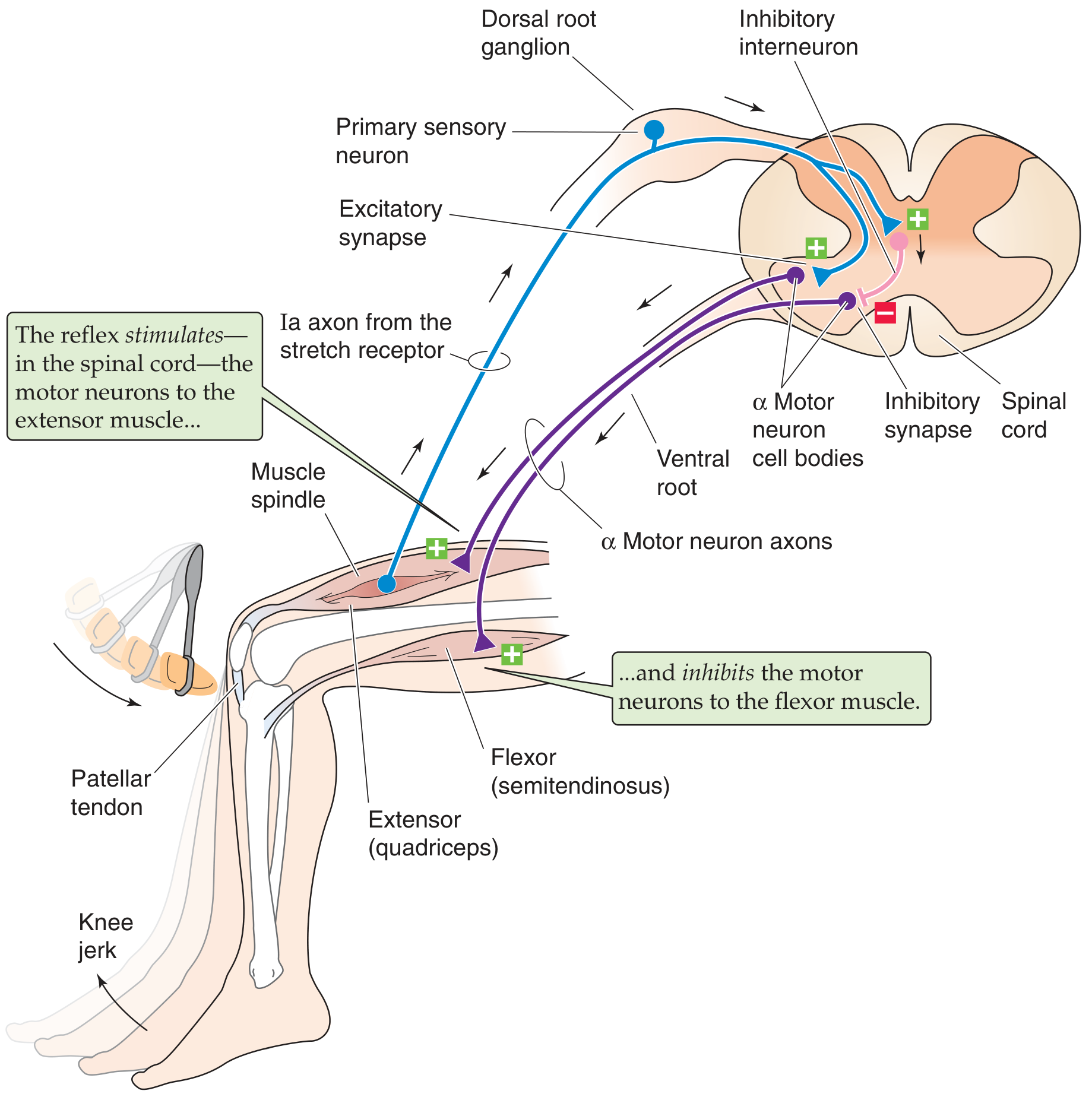
- Receptor - muscle spindle (stretch detector)
- Afferent neuron - Ia axon (primary sensory, fast)
- Nerve center - spinal cord (monosynaptic + inhibitory interneuron)
- Efferent neuron - α motor neuron (ventral root)
- Effector - quadriceps muscle (contracts); antagonist flexor (relaxed via reciprocal inhibition)
Q8 — Pre- and Postsynaptic Inhibition in CNS
Q9 — Autonomic Nervous System Organization (Sympathetic + Parasympathetic + Somatic)
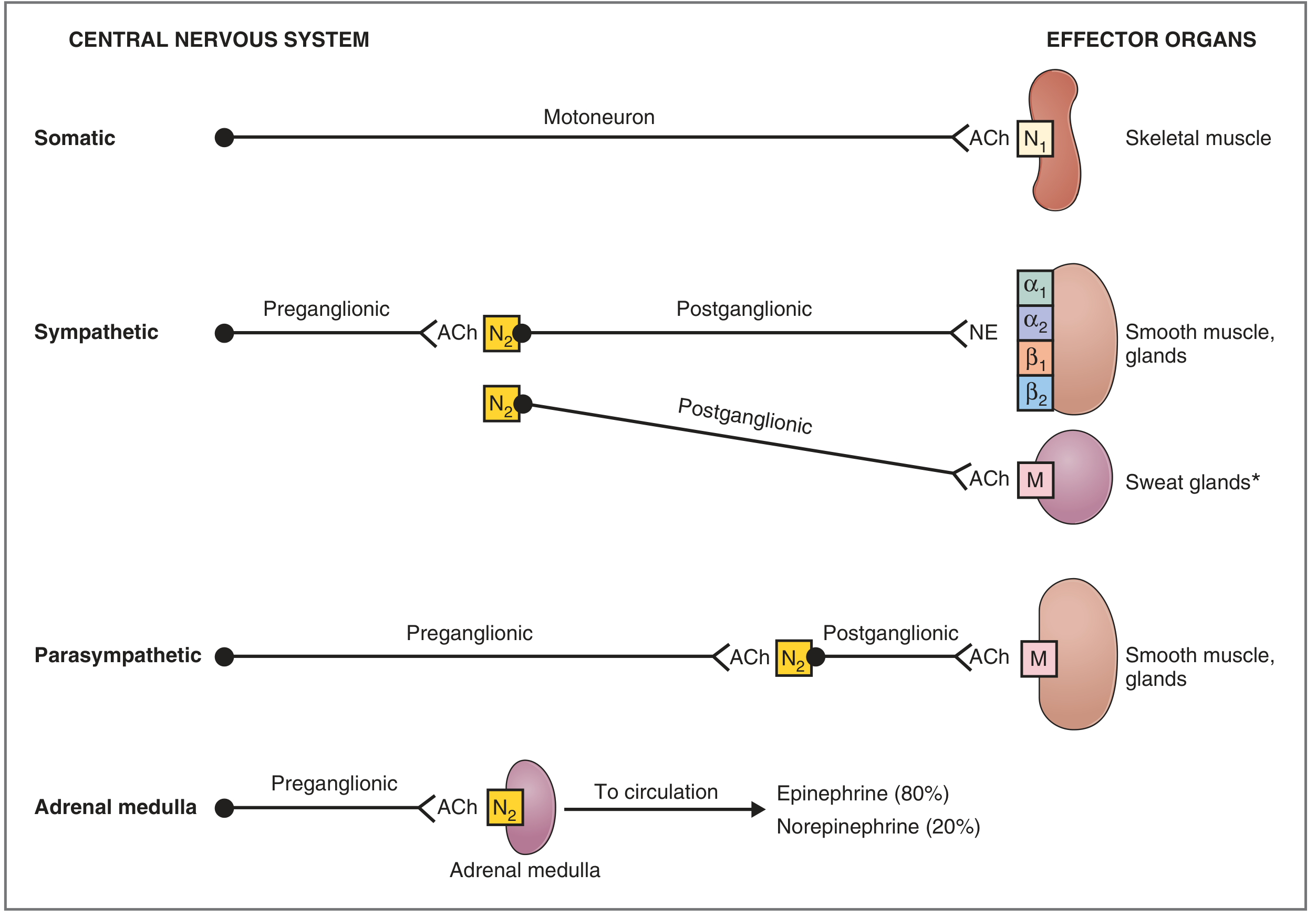
- Sympathetic: short preganglionic (T1-L2), long postganglionic, NE transmitter, α/β receptors
- Parasympathetic: long preganglionic (CN III/VII/IX/X + S2-4), short postganglionic, ACh transmitter, muscarinic receptors
- Both divisions use ACh at preganglionic synapse (nicotinic N2 receptors)
Q10 — Protein Hormone Mechanism (Cell Surface Receptors)
Q11 — Steroid Hormone Mechanism (Nuclear Receptors)
Q12 — Hypothalamic-Pituitary Axis (Feedback Regulation)
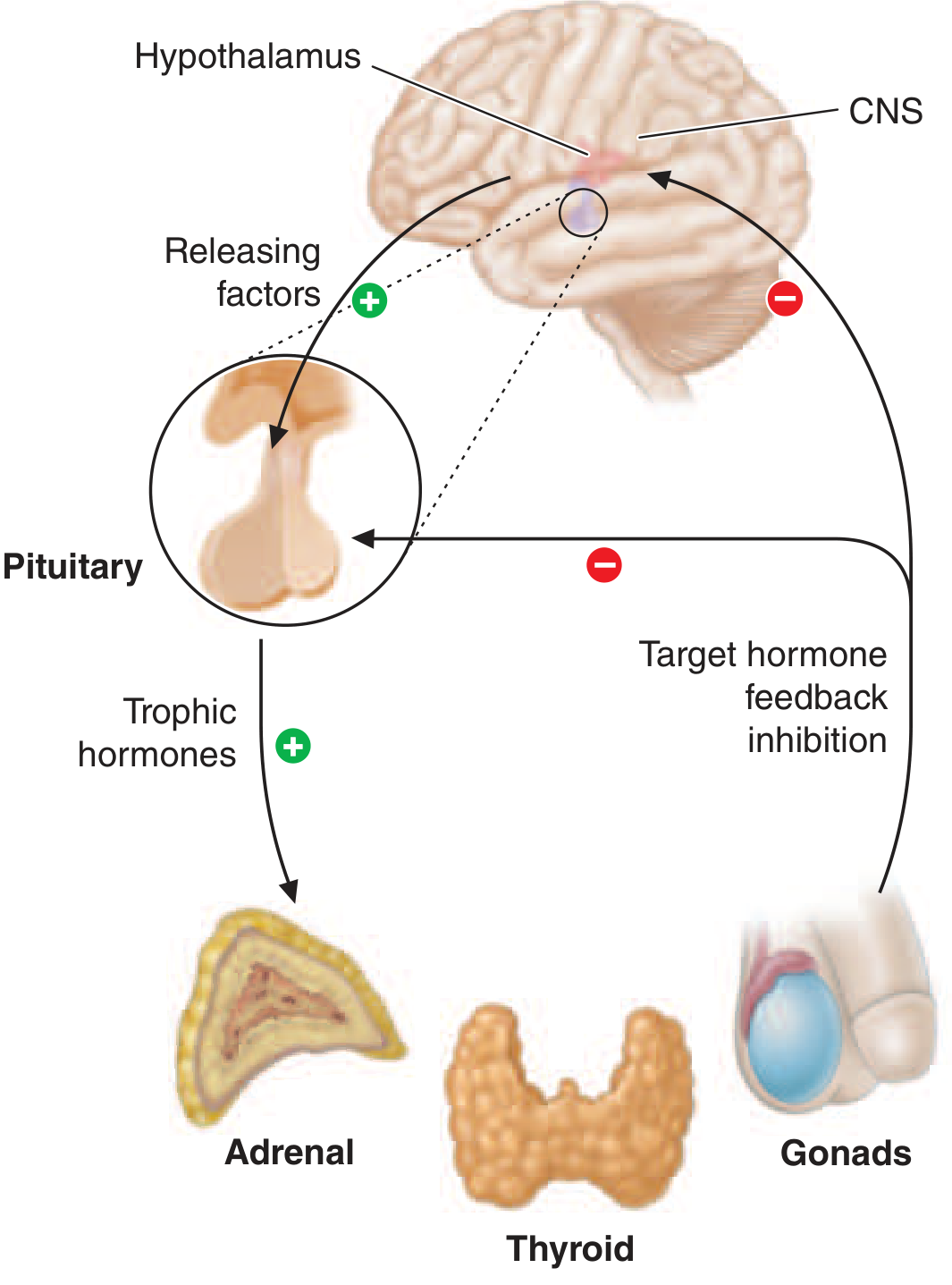
- HPA: CRH → ACTH → Cortisol (−feedback)
- HPT: TRH → TSH → T3/T4 (−feedback)
- HPG: GnRH → LH/FSH → sex steroids (−feedback)
Q13 — Blood Test Interpretation
| Parameter | Reference Range | Low = | High = |
|---|---|---|---|
| Hb ♂ | 130-170 g/L | Anemia | Polycythemia |
| Hb ♀ | 120-150 g/L | Anemia | Polycythemia |
| WBC | 4.0-9.0 ×10⁹/L | Leukopenia | Leukocytosis |
| Platelets | 150-400 ×10⁹/L | Thrombocytopenia | Thrombocytosis |
| MCV | 80-100 fL | Microcytic anemia | Macrocytic anemia |
| Neutrophils | 50-70% | Neutropenia | Bacterial infection |
| ESR | <15 mm/h (♂), <20 (♀) | — | Inflammation |
Q14 — ABO and Rh Blood Typing
| Group | RBC Antigen | Plasma Antibody |
|---|---|---|
| A | A | Anti-B |
| B | B | Anti-A |
| AB | A + B | None (universal recipient) |
| O | None | Anti-A + Anti-B (universal donor) |
Q15 — Cardiac Ventricular AP (Phases 0-4) + Ionic Currents
Q16 — Pacemaker Cell AP vs. Ventricular AP
Q17 — Cardiac Conduction System
| Structure | Rate (bpm) | Conduction Velocity |
|---|---|---|
| SA node | 60-100 | 0.05 m/s |
| AV node | 40-60 | 0.02-0.05 m/s (slowest - AV delay) |
| Bundle of His | — | 0.1-0.2 m/s |
| Bundle branches / Purkinje | 20-40 | 2-4 m/s (fastest) |
| Ventricular muscle | 20-40 | 0.3-0.5 m/s |
Q18 — ECG: Determine Pacemaker
- P wave before every QRS, upright in II → SA node (normal sinus rhythm)
- No P waves, narrow QRS → AV node (junctional rhythm, 40-60 bpm)
- No P waves, wide bizarre QRS (>0.12s) → ventricular pacemaker (idioventricular, 20-40 bpm)
Q19 — ECG: Heart Rate + Cardiac Cycle Duration
- HR = 300 ÷ (number of large squares between R-R peaks)
- e.g., 4 large squares → HR = 300/4 = 75 bpm
- Cardiac cycle duration = 60 ÷ HR (in seconds)
- e.g., 75 bpm → 0.8 s; 60 bpm → 1.0 s; 100 bpm → 0.6 s
- Paper speed 25 mm/s: 1 small square = 0.04 s; 1 large square = 0.2 s
Q20 — ECG: Electrical Axis in Frontal Plane
| Lead I | aVF | Axis |
|---|---|---|
| + | + | Normal (0° to +90°) |
| + | − | Left axis deviation (<−30°) |
| − | + | Right axis deviation (>+90°) |
| − | − | Extreme axis (±180°) |
Q21 — Sphygmogram (Arterial Pulse Curve)
Pressure
↑ Peak (systolic)
/‾‾\ /\ ← dicrotic wave
/ \_/ \___ → diastolic baseline
/ ↑ ↑
↑ dicrotic notch
anacrotic
limb
- Anacrotic limb: Rapid systolic pressure rise (ventricular ejection)
- Dicrotic notch: Aortic valve closure (end systole)
- Dicrotic wave: Aortic wall elastic recoil after valve closure
- Catacrotic limb: Gradual diastolic pressure fall
Q22 — Phlebogram (Venous/JVP Waveform)
Pressure
↑ a c v
/\ /|/\
/ X \ /\
─/ / \ V \─
x y
descent
- a wave: Atrial contraction (just before QRS)
- c wave: Tricuspid valve bulging into atrium
- x descent: Atrial relaxation + tricuspid descent
- v wave: Passive venous filling (tricuspid closed during systole)
- y descent: Tricuspid opens → blood empties into ventricle
Q23 — External Respiration: Spirometry (Lung Volumes + FEV₁)
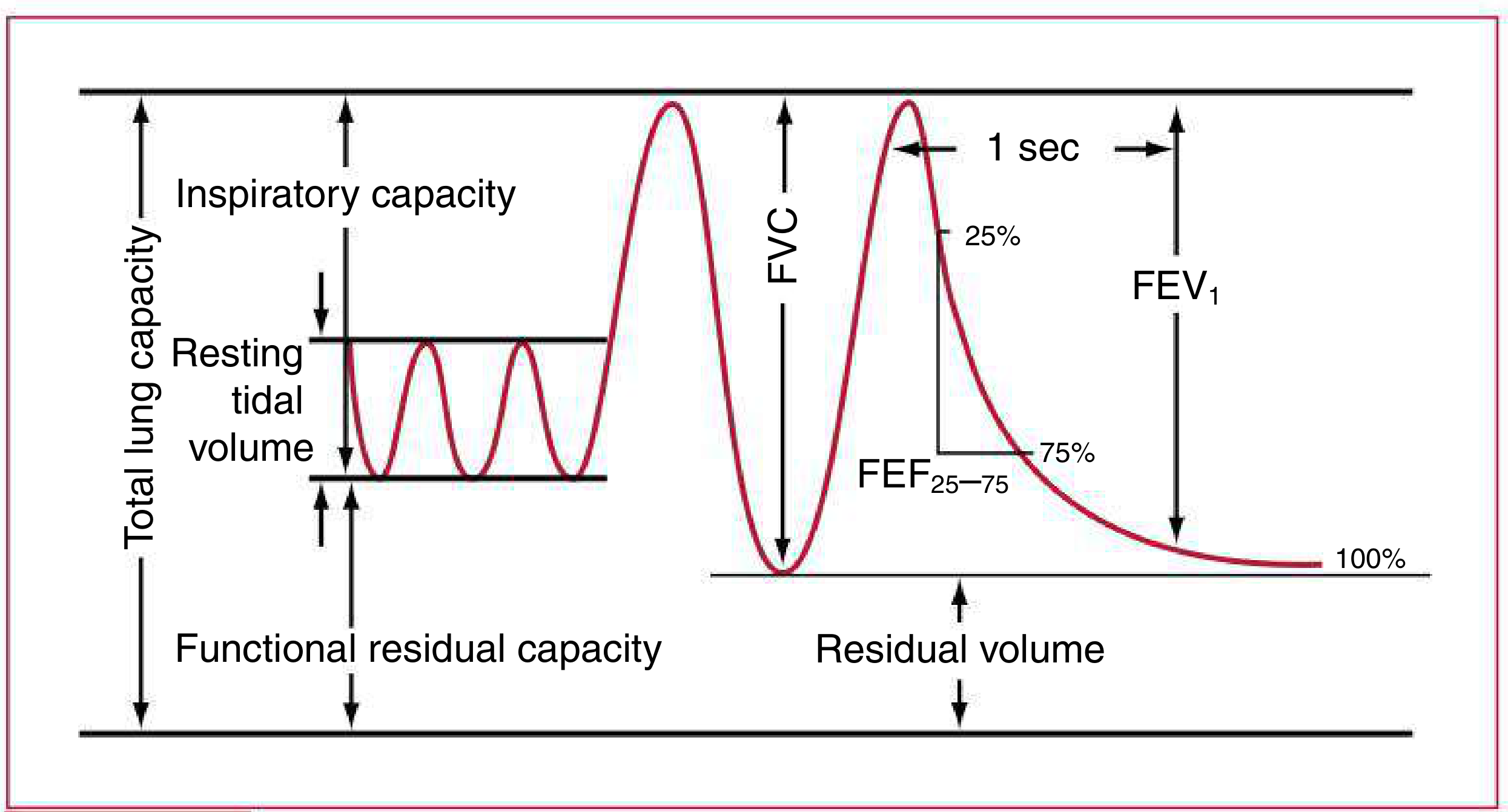
| Pattern | FEV₁/FVC | TLC | Example |
|---|---|---|---|
| Normal | >70% | Normal | — |
| Obstructive | ↓ (<70%) | ↑ or normal | Asthma, COPD |
| Restrictive | Normal or ↑ | ↓ | Fibrosis, NM disease |
Q24 — RAAS Scheme (Renin-Angiotensin-Aldosterone)
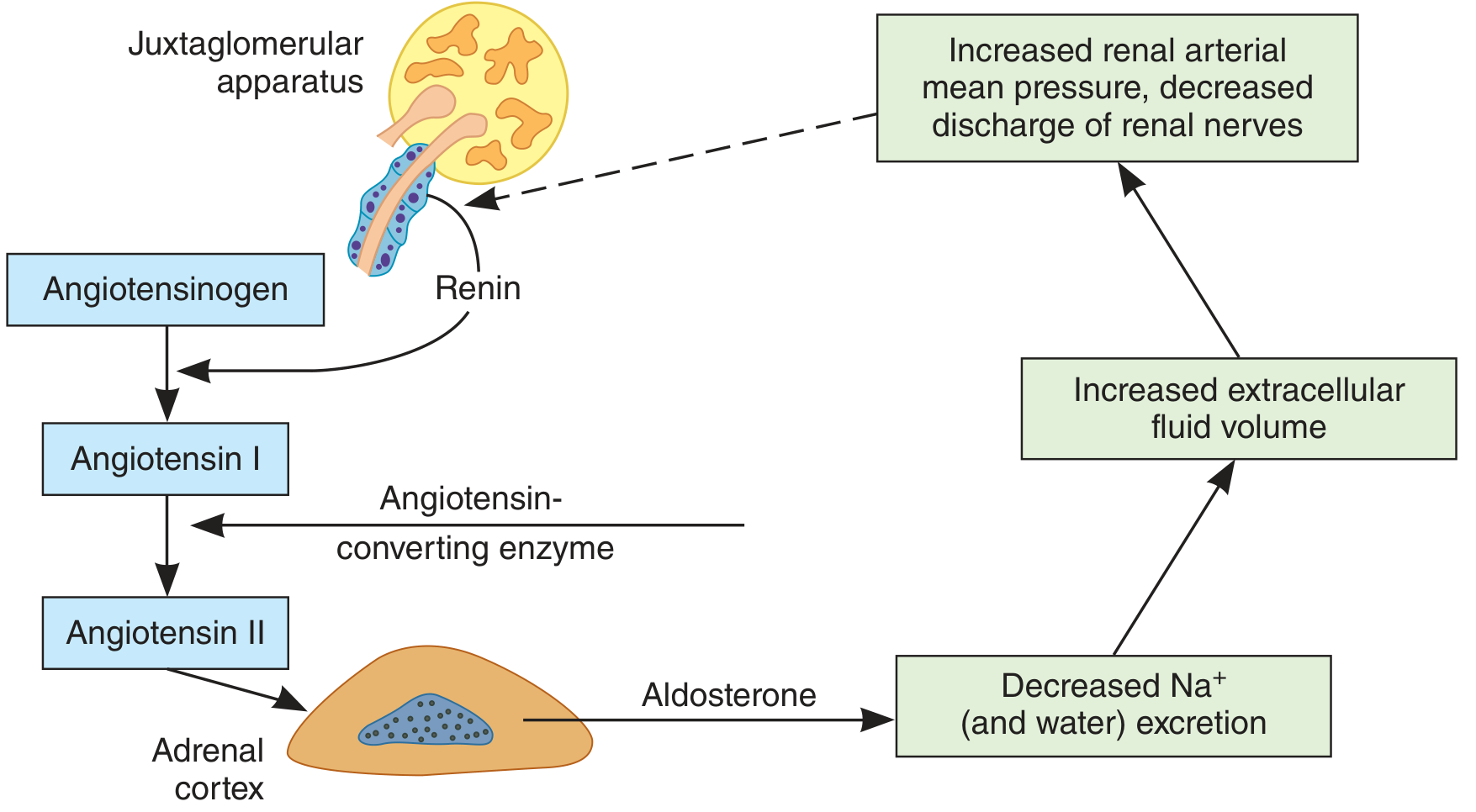
- Renin release (JGA): triggered by ↓renal perfusion pressure, ↓NaCl at macula densa, ↑sympathetic discharge
- Aldosterone effect on kidney: ↑Na⁺ + H₂O reabsorption in collecting duct → ↑ECF volume → ↑BP
- Negative feedback: restored BP/volume shuts off renin release
Q25 — Osmotic Pressure Regulation by Kidneys (ADH Feedback)
Q26 — Sensory System Structure and Function
- 1st order (peripheral receptor): Transduces adequate stimulus → generator potential → AP in afferent fiber
- 2nd order (spinal cord / brainstem): Crosses midline (decussates), ascends to thalamus
- 3rd order (thalamus → cortex): Projects to primary somatosensory cortex (postcentral gyrus) → conscious perception
- Association cortex: Integration, interpretation, memory
Q27 — Conditioned Reflex Development Rules (Pavlov)
- CS must precede UCS by short interval (0.5-5 s)
- Repeated pairing required (reinforcement)
- UCS must be biologically stronger/more significant than CS
- Subject must be healthy and attentive
- CS must be initially neutral (no strong pre-existing response)
Q28 — Thermoregulation at High Environmental Temperature
- ↑Sweating (sympathetic cholinergic to sweat glands → evaporative cooling)
- Cutaneous vasodilation → ↑blood to skin surface → ↑radiation + convection
- ↓Muscle tone → ↓metabolic heat production
- ↑Respiratory rate → ↑evaporative loss
Q29 — Thermoregulation at Low Environmental Temperature
- Cutaneous vasoconstriction → ↓blood to skin → ↓heat loss
- Shivering (involuntary skeletal muscle contractions) → ↑heat up to 5x resting
- Non-shivering thermogenesis (sympathetic → NE → brown adipose tissue → UCP1/thermogenin → uncoupled oxidative phosphorylation → heat)
- Piloerection → traps air layer (minimal in humans)
- Long-term: ↑thyroid hormone → ↑basal metabolic rate
Q30 — Conditioned vs. Unconditioned Salivary Reflexes
Q31 — Gamma Loop + Alpha vs. Gamma Motoneurons
α Motor neuron ──────────────────→ Extrafusal fibers (force)
↑
γ Motor neuron ──→ Intrafusal fibers (spindle tension set)
↓
Ia afferent fires ────→ α Motor neuron
(if muscle too long) (stretch reflex)
| Feature | α Motoneuron | γ Motoneuron |
|---|---|---|
| Target | Extrafusal fibers | Intrafusal (spindle) fibers |
| Function | Force generation | Spindle sensitivity adjustment |
| Fiber type | Large, Aα (70-120 m/s) | Smaller, Aγ (15-30 m/s) |
| Proportion | ~70% ventral horn | ~30% ventral horn |
Q32 — Hans Selye's General Adaptation Syndrome (GAS)
STRESSOR
↓
STAGE 1: ALARM
Shock phase (↓BP, ↑capillary permeability)
Counter-shock:
• Epinephrine/NE (adrenal medulla) → ↑HR, ↑BP, ↑glucose
• Cortisol ↑↑ (HPA: CRH → ACTH → cortisol)
↓ (if stress continues)
STAGE 2: RESISTANCE (Adaptation)
• Cortisol (sustained): ↑gluconeogenesis, anti-inflammatory
• Aldosterone: ↑Na⁺ retention → ↑volume → ↑BP
• GH + Glucagon: fat/protein mobilization
• Reproductive hormones suppressed
Maximum resistance to stressor; normal function maintained
↓ (if severe/prolonged)
STAGE 3: EXHAUSTION
• Adrenal cortex depleted: ↓cortisol, ↓aldosterone
• ↓Immunity, ↓glucose, organ failure
• Resembles alarm but without adaptive capacity
• Death possible if untreated
| Stage | Key Hormones | Effect |
|---|---|---|
| Alarm | Epinephrine, NE, Cortisol | Fight-or-flight mobilization |
| Resistance | Cortisol, Aldosterone, GH | Sustained adaptation |
| Exhaustion | All ↓ | Failure, organ damage |
Create a PDF study guide compiling all 32 Q&A with diagrams
ls /home/daytona/workspace/ && mkdir -p /home/daytona/workspace/physiology-study-guide