Please tell me the specification of NADH, NADPH, FADH, FADPH, all terms from biochemistry.
Reading File
Finding Sources
Finding Sources
Searching the Web
NADH NADPH FADH2 biochemistry specification structure function comparison
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
I now have all the information needed for a thorough, authoritative answer. Let me compose it.
NADH, NADPH, FADH2 - Complete Biochemical Specifications
Note on "FADPH": This is not a standard biochemistry term. You likely mean FADH2 (fully reduced FAD). There is no "FADPH" in established biochemistry nomenclature. This answer covers NADH, NADPH, and FADH2, plus their oxidized counterparts for context.
1. NAD+ / NADH
Full Name
Nicotinamide Adenine Dinucleotide (oxidized = NAD+; reduced = NADH)
Vitamin Precursor
Niacin (Vitamin B3) - either nicotinic acid or nicotinamide (the amide form is nutritionally equivalent as it is deaminated in vivo).
Structure
NAD+ is a dinucleotide made of:
- Nicotinamide (pyridine ring with an amide substituent) - the active redox-capable portion
- Ribose (nicotinamide-ribose = nicotinamide mononucleotide)
- Pyrophosphate bridge
- Ribose-adenine (adenosine monophosphate portion)
The structure shown below (NAD+/NADP+ comparison from Basic Medical Biochemistry, 6th ed.):
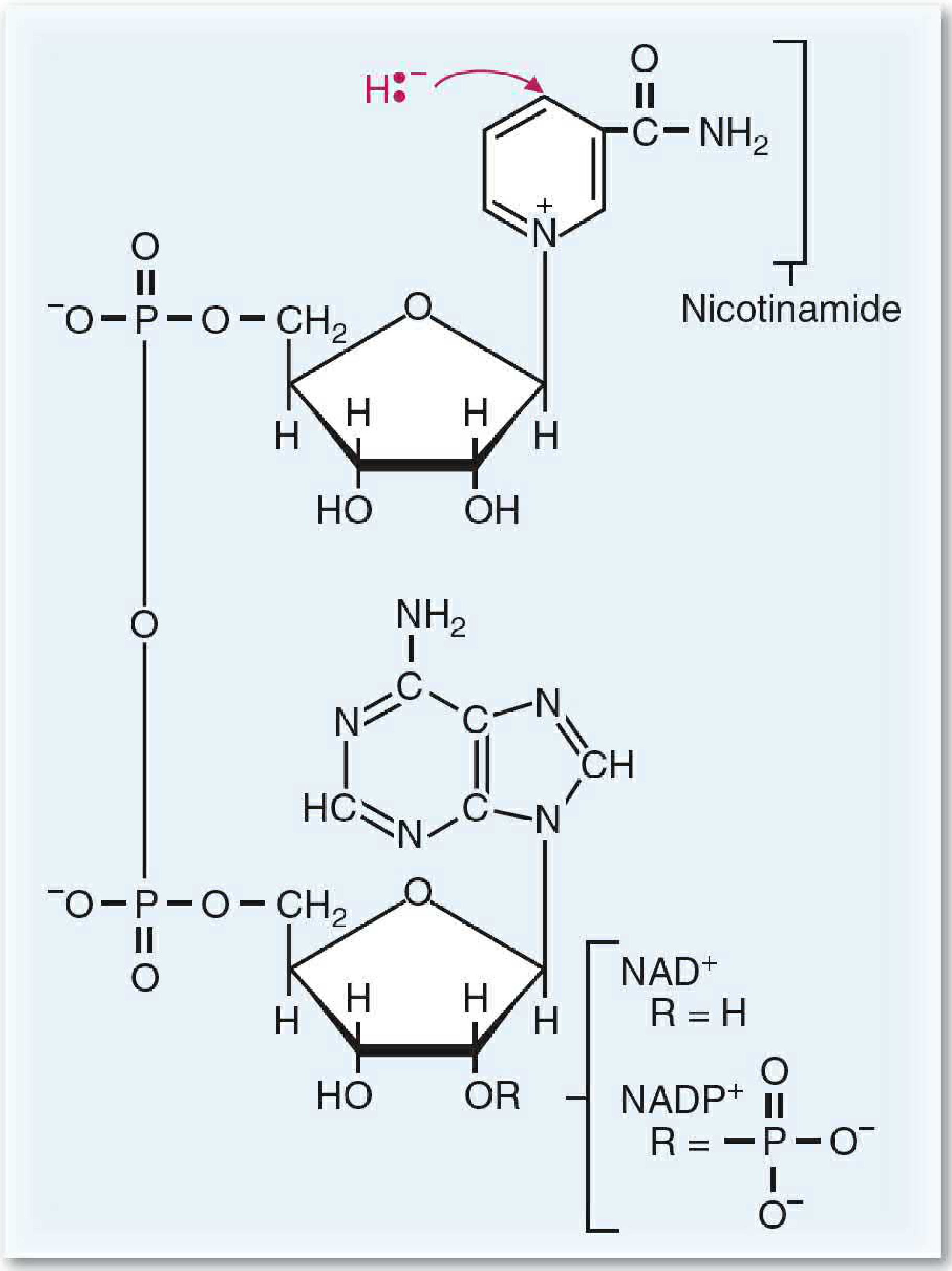
Electron Transfer Mechanism
NAD+ accepts 2 electrons as a hydride ion (H:-) at the C-4 (para) position of the nicotinamide ring, plus releases 1 H+ into solution:
NAD+ + 2H+ + 2e- → NADH + H+
NADH and NADPH (but not NAD+ and NADP+) absorb light at 340 nm - this is used in laboratory enzyme assays. - Tietz Textbook of Laboratory Medicine, 7th Ed.
Solubility / Binding
- Freely diffusible coenzyme (not permanently bound to enzymes)
- Acts as a dissociable substrate in dehydrogenase reactions
Key Metabolic Role - CATABOLISM
NAD+ is the primary electron acceptor in catabolic (energy-releasing) pathways:
| Pathway | Where NADH is generated |
|---|---|
| Glycolysis | G3P dehydrogenase |
| Pyruvate dehydrogenase | Pyruvate → Acetyl-CoA |
| TCA/Krebs cycle | Isocitrate-, α-ketoglutarate-, malate dehydrogenases |
| Beta-oxidation (fatty acids) | 3-hydroxyacyl-CoA dehydrogenase |
| Amino acid catabolism | Various dehydrogenases |
ATP Yield
- ~2.5 ATP per NADH oxidized in the mitochondrial electron transport chain (ETC)
- Electrons enter at Complex I (NADH dehydrogenase), pumping 10 protons total - Medical Physiology
Steady-state NAD+/NADH ratio
- Cytoplasm: ~1,000:1 (strongly favors oxidative/catabolic use of NAD+)
2. NADP+ / NADPH
Full Name
Nicotinamide Adenine Dinucleotide Phosphate (oxidized = NADP+; reduced = NADPH)
Structure
Identical to NAD+/NADH except for an additional phosphate group esterified to the 2'-OH of the adenosine ribose unit (shown in blue in the diagram above).
The structure from Lippincott's Biochemistry, 8th ed.:
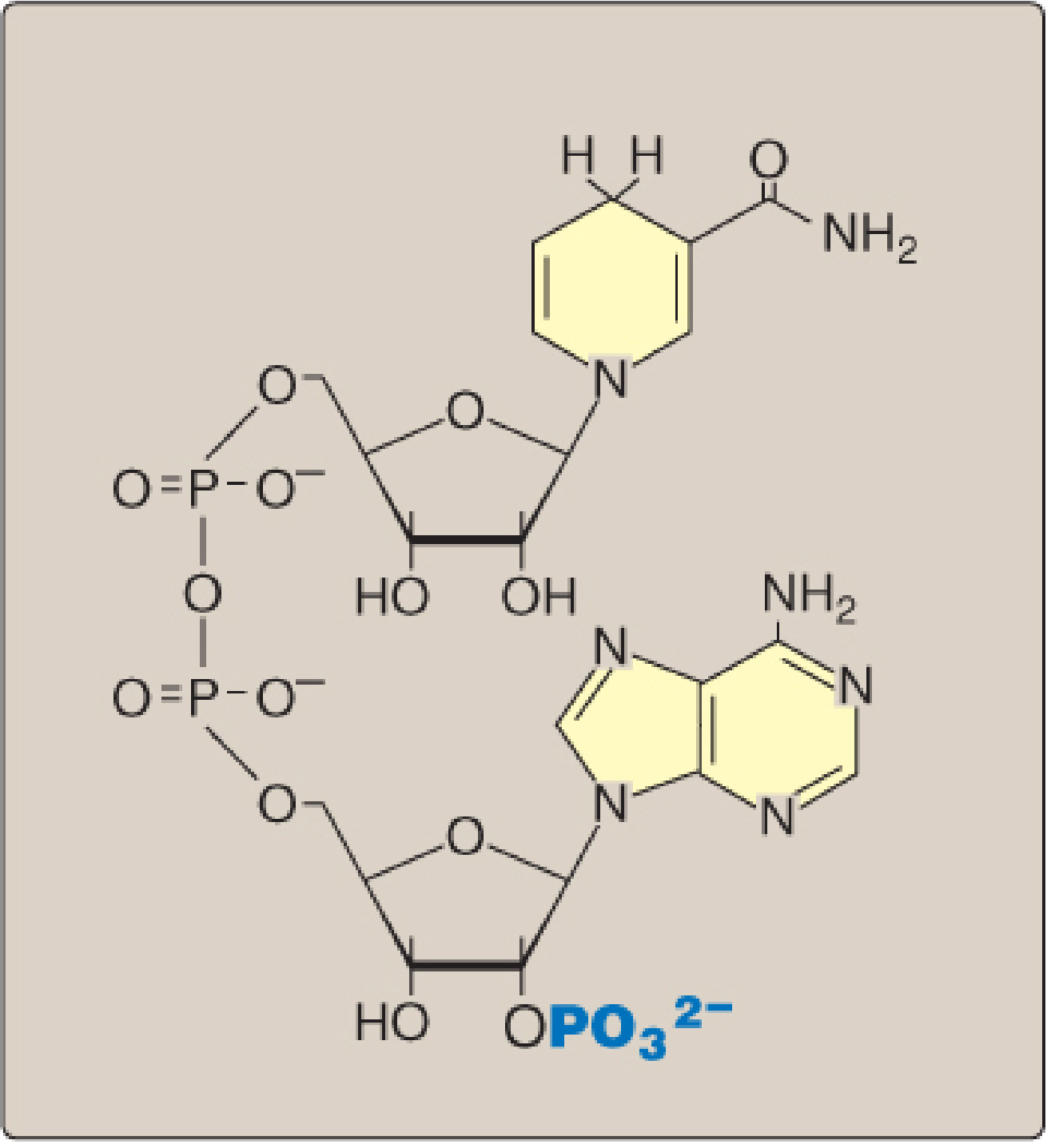
"The coenzyme NADPH differs from nicotinamide adenine dinucleotide (NADH) only by the presence of a phosphate group on one of the ribose units." - Lippincott's Biochemistry, 8th ed., p.430
Why the Extra Phosphate Matters
This seemingly small structural change allows NADPH to bind NADPH-specific enzymes that have unique roles - the cell can keep NAD+ and NADP+ pools functionally separate.
Electron Transfer Mechanism
Same as NAD+ - accepts a hydride ion (H:-) at the nicotinamide C-4 position.
Key Metabolic Role - ANABOLISM & ANTIOXIDANT DEFENSE
NADPH is the primary electron donor in anabolic (biosynthetic) and detoxification reactions:
| Function | Details |
|---|---|
| Fatty acid synthesis | Provides reducing equivalents for FAS enzyme complex |
| Cholesterol synthesis | Required for mevalonate pathway |
| Glutathione reduction | Regenerates GSH from GSSG via glutathione reductase |
| Cytochrome P450 reactions | Drug detoxification, steroid hydroxylation |
| Pentose phosphate pathway | Glucose-6-phosphate dehydrogenase regenerates NADPH |
| Phagocyte oxidative burst | NADPH oxidase generates superoxide (bactericidal) |
Steady-state NADP+/NADPH ratio
- Cytoplasm of hepatocytes: ~0.1:1 (strongly favors the reductive/anabolic role of NADPH) - Lippincott's, 8th ed.
ATP yield
NADPH is not used in oxidative phosphorylation to make ATP. It donates electrons directly to biosynthetic enzymes, not the ETC.
3. FAD / FADH2
Full Name
Flavin Adenine Dinucleotide (oxidized = FAD; reduced = FADH2)
- Also written as FAD(2H) in some texts to reflect the radical mechanism.
Vitamin Precursor
Riboflavin (Vitamin B2)
Structure
FAD consists of:
- Isoalloxazine ring (the flavin moiety, derived from riboflavin) - the redox-active part
- Ribitol (5-carbon sugar alcohol)
- Pyrophosphate bridge
- Adenosine (ribose + adenine)
The structure from Basic Medical Biochemistry, 6th ed.:
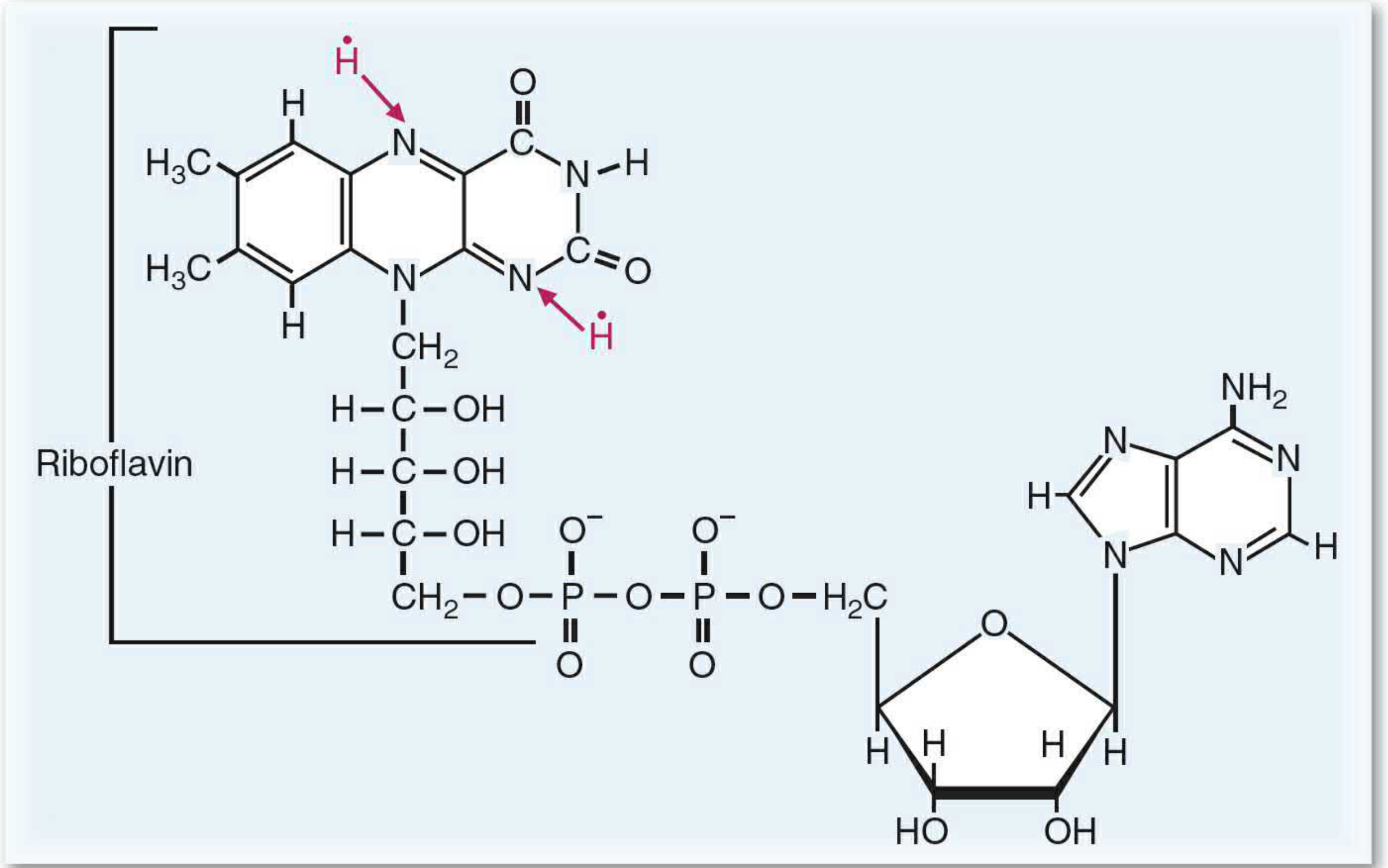
Electron Transfer Mechanism
Unlike NAD+, FAD accepts 2 electrons as two separate hydrogen atoms (one at a time, as radicals), donated from separate atoms on the substrate:
FAD + 2H• → FADH2
This is used for reactions involving formation of a double bond or a disulfide, where electrons are donated singly. - Basic Medical Biochemistry, 6th ed.
Binding
A key difference from NAD+/NADPH: FAD is tightly (covalently or very tightly non-covalently) bound to its enzymes as a prosthetic group, not freely diffusible. This is because FADH2 is susceptible to reaction with molecular oxygen (O2), unlike NADH.
Key Metabolic Roles
| Pathway | Enzyme | Why FAD and not NAD+ |
|---|---|---|
| TCA cycle | Succinate dehydrogenase (Complex II) | Oxidizes C-C single to double bond |
| Beta-oxidation | Acyl-CoA dehydrogenase | Introduces double bond into acyl chain |
| Pyruvate dehydrogenase complex | Dihydrolipoyl dehydrogenase (E3 subunit) | Regenerates oxidized lipoamide |
| Electron transport chain | Complex II | Entry point for FADH2 electrons |
ATP Yield
- ~1.5 ATP per FADH2 oxidized in the ETC
- Electrons enter at Complex II (bypassing Complex I), pumping fewer protons - hence lower ATP yield than NADH - Harper's Biochemistry, 32nd ed.
Head-to-Head Comparison Table
| Property | NADH | NADPH | FADH2 |
|---|---|---|---|
| Full name | Nicotinamide Adenine Dinucleotide (reduced) | Nicotinamide Adenine Dinucleotide Phosphate (reduced) | Flavin Adenine Dinucleotide (reduced) |
| Vitamin precursor | Niacin (B3) | Niacin (B3) | Riboflavin (B2) |
| Oxidized form | NAD+ | NADP+ | FAD |
| Structural difference | - | Extra 2'-phosphate on adenosine ribose | Isoalloxazine ring; ribitol chain |
| Electron transfer | 2e- as hydride (H:-) | 2e- as hydride (H:-) | 2e- as 2 hydrogen atoms (radical mechanism) |
| Enzyme binding | Freely diffusible | Freely diffusible | Tightly bound prosthetic group |
| Primary metabolic role | Catabolism (ETC substrate) | Anabolism, antioxidant defense | Catabolism (ETC substrate) |
| ETC entry point | Complex I | Not used in ETC | Complex II |
| ATP yield (ETC) | ~2.5 ATP | Not applicable | ~1.5 ATP |
| NAD(P)+/NAD(P)H ratio (cytosol) | ~1,000:1 | ~0.1:1 | N/A (enzyme-bound) |
| Key pathways | Glycolysis, TCA, β-oxidation | Pentose-P pathway, FA synthesis, GSH regeneration | TCA (succinate DH), β-oxidation |
What About "FADPH"?
FADPH does not exist as a standard biochemical molecule. It is not recognized in any major biochemistry textbook or nomenclature system. You may have encountered it as a typographical error or confusion with:
- FADH2 (fully reduced FAD, described above)
- FMNH2 (Flavin Mononucleotide - reduced; FMN = riboflavin + one phosphate, used in Complex I)
- NADPH (a different molecule entirely)
If you saw "FADPH" in a specific context (e.g., a textbook or question), please share it and I can clarify.
Sources: Lippincott's Illustrated Reviews Biochemistry 8th ed.; Basic Medical Biochemistry - A Clinical Approach 6th ed.; Harper's Illustrated Biochemistry 32nd ed.; Medical Physiology (Boron & Boulpaep); Tietz Textbook of Laboratory Medicine 7th ed.

photo-1784097178020.jpg
Diagnoses
analyse_media
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
I have a good picture now. Let me compile the full clinical analysis.
Clinical Image Analysis
Image findings: The photo shows a clenched fist (dorsal view) with a single small, dark brown hyperpigmented macule/flat spot at the dorsal hand near the base of the index finger / first web space. The knuckles appear structurally normal, no gross swelling or deformity is visible.
Differential Diagnoses
Based on what is visible - a small, flat, dark brown/hyperpigmented lesion on the dorsum of the hand - the main possibilities from most to least likely are:
1. Post-Inflammatory Hyperpigmentation (PIH) - Most Likely
A localized darkening of skin following minor trauma (scratch, knock, insect bite). Extremely common in darker skin tones (Fitzpatrick types IV-VI), where melanocytes respond vigorously to any inflammation. The lesion is flat (macular), well-defined, and brownish - classic for PIH.
- No treatment needed in most cases; fades over months
- SPF protection speeds resolution
2. Simple Lentigo / Solar Lentigo
A benign, discrete hyperpigmented macule that can appear at any age on any body part, including the dorsum of the hand. Unlike freckles, color does not depend on sun exposure. - Andrews' Diseases of the Skin
- Benign, no treatment required unless for cosmetic reasons
- Can be confirmed with dermatoscopy
3. Dermatofibroma (small, early)
A small benign fibrous nodule; early lesions may appear as flat pigmented macules before developing into a firm papule. Common on the extremities.
4. Knuckle Pad (Garrod Pad) - Less likely here
Knuckle pads are well-defined, round, plaque-like fibrous thickenings on the extensor aspects of the PIP joints. They are flesh-colored to slightly brown, 10-15 mm in diameter, and slightly raised. They are associated with Dupuytren contracture and can follow repeated trauma or knuckle cracking. - Andrews' Diseases of the Skin, p.704
Compare the textbook image of true knuckle pads (below) - these are much more prominent raised plaques than what is shown in your image:
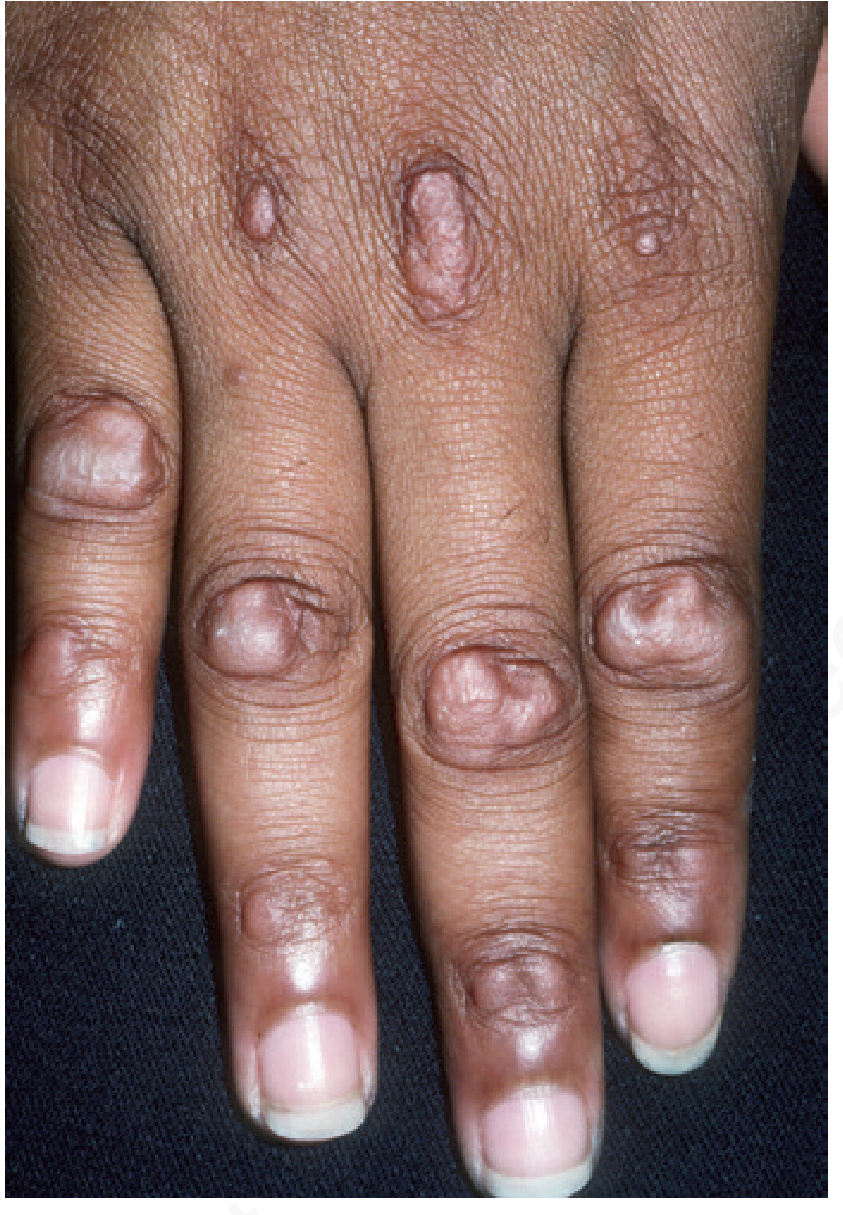
The lesion in your image appears smaller and flatter than classical knuckle pads.
5. Seborrheic Keratosis (early)
Can begin as a flat hyperpigmented macule before progressing to the characteristic "stuck-on" waxy plaque. More common in adults over 40. - Textbook of Family Medicine, 9th ed.
6. Melanocytic Nevus (mole)
A benign cluster of melanocytes. If the lesion is well-established, non-growing, and uniform in color and border, this is entirely benign.
When to See a Dermatologist
Seek evaluation if the lesion:
- Is new and growing rapidly
- Has irregular borders, multiple colors, or diameter >6 mm (ABCDE rule)
- Bleeds, itches, or crusts without a clear cause
- Has been present for years and recently changed
Important disclaimer: This is a general educational assessment based on a photo. It is not a medical diagnosis. A definitive diagnosis requires in-person clinical examination by a licensed healthcare provider, and possibly dermatoscopy or biopsy. Please consult a doctor or dermatologist for a proper evaluation.
This is a shared conversation. Sign in to Orris to start your own chat.