National programs in the pnc case
India national programs prenatal antenatal care PNC community medicine ICMR WHO
National Programs in Prenatal Care (PNC) - India
I. Antenatal Care (ANC) - Essential Components under National Guidelines
- Early registration of all pregnancies within the first trimester (before 12 weeks)
- Minimum 4 ANC visits (WHO now recommends 8):
- 1st visit: within 12 weeks (registration + first check-up)
- 2nd visit: 14-26 weeks
- 3rd visit: 28-34 weeks
- 4th visit: 36 weeks to term
- Associated services: height, weight, BP, anaemia check, abdominal examination, breast examination, folic acid (1st trimester), IFA supplementation from 12 weeks, tetanus toxoid injection, anaemia treatment
- Minimum investigations: urine for pregnancy confirmation, Hb estimation, urine for albumin and sugar
- Name-based tracking of all pregnant women for assured service delivery
- Identification of high-risk pregnancies and danger signs
- Malaria prophylaxis in endemic zones (as per NVBDCP guidelines)
- Counselling: diet, rest, tobacco cessation, institutional delivery, birth preparedness, complication readiness
- Information on JSY and other government scheme entitlements
- RTI/STI identification and referral; HIV/AIDS counselling
II. Key National Programs in PNC (India)
1. Janani Suraksha Yojana (JSY) - 2005
- Launched: 12th April, 2005 (modification of the earlier National Maternity Benefit Scheme)
- Objective: Reduce maternal and neonatal mortality by promoting institutional deliveries, especially in Below Poverty Line (BPL) families
- 100% centrally sponsored scheme under NRHM
- Provides cash assistance integrated with institutional ANC, delivery, and immediate postpartum care
- Two categories of states:
- Low Performing States (LPS): UP, Uttarakhand, MP, Jharkhand, Bihar, Rajasthan, Chhattisgarh, Odisha, Assam, J&K - all women regardless of BPL status
- High Performing States (HPS): Only BPL women + SC/ST women
- Cash assistance scale (from 2012-13):
| Category | Rural (Mother's pkg) | ASHA pkg | Total | Urban (Mother's pkg) | ASHA pkg | Total |
|---|---|---|---|---|---|---|
| LPS | Rs. 1400 | Rs. 600 | Rs. 2000 | Rs. 1000 | Rs. 400 | Rs. 1400 |
| HPS | Rs. 700 | Rs. 600 | Rs. 1300 | Rs. 600 | Rs. 400 | Rs. 1000 |
- ASHA acts as a link health worker responsible for making available institutional ANC, postnatal care, and escorting pregnant women to health centres
2. Janani Shishu Suraksha Karyakram (JSSK) - 2011
- Launched: 1st June, 2011
- Objective: Eliminate out-of-pocket expenses for pregnant women delivering in public health institutions
- Entitlements:
- Absolutely free delivery (including caesarean section)
- Free drugs and consumables
- Free diet: up to 3 days for normal delivery, up to 7 days for C-section
- Free diagnostics and free blood
- Free transport: home to institution, between facilities (referral), and drop-back home
- Extended to sick newborns in public facilities up to 30 days after birth
- Scheme extended to cover complications during ANC, PNC and sick infants
- Estimated to benefit over 12 million pregnant women per year
3. Pradhan Mantri Surakshit Matritva Abhiyan (PMSMA) - 2016
- Launched: June 2016 by the Ministry of Health & Family Welfare
- Objective: Provide fixed-day, free-of-cost, assured, quality ANC to all pregnant women
- Minimum ANC package (investigations + drugs) provided on the 9th of every month at designated government health facilities
- Involves private sector volunteers providing specialist care at government facilities
- Achievements: ~2.20 crore ANC check-ups by ~6,000 volunteers at >17,000 government facilities; >11.66 lakh high-risk pregnancy cases identified nationally
4. SUMAN (Surakshit Matritva Aashwasan) - 2019
- Launched: 10th October, 2019
- Objective: Assured, dignified, respectful, and quality healthcare at no cost with zero tolerance for denial of services for every woman and newborn at public health facilities
- Expected outcome: "Zero preventable maternal and newborn deaths and high quality of maternity care delivered with dignity and respect"
5. LaQshya Programme - 2017
- Launched by MOHFW in 2017
- Objective: Improve quality of care in labour rooms and maternity OTs in public health facilities
- Evidence-based approach to improve maternal and newborn care and provide respectful care during the intrapartum and postpartum periods
- Implementation: infrastructure upgradation, essential equipment availability, adequate staffing
III. Postnatal Care (PNC) Components under National Guidelines
- Early breastfeeding initiation within 1 hour of birth
- Postnatal home visits on days 0, 3, 7, and 42 for home/sub-centre deliveries
- Ensure visits on days 3 and 7 for institutional deliveries
- Management of postpartum complications
Summary Table
| Program | Year Launched | Key Focus |
|---|---|---|
| JSY | 2005 | Cash incentive for institutional delivery (BPL women) |
| JSSK | 2011 | Free delivery, free drugs/diagnostics/transport at public facilities |
| PMSMA | 2016 | Free ANC on 9th of every month, high-risk identification |
| SUMAN | 2019 | Dignified, respectful, zero-denial maternity care |
| LaQshya | 2017 | Quality improvement in labour rooms and maternity OTs |
- Park's Textbook of Preventive and Social Medicine, pp. 514-517 and pp. 4785-4815
Explain the role and responsibilities of ASHAs in India's prenatal programs
Role and Responsibilities of ASHAs in India's Prenatal Programs
Who is an ASHA?
- Must be a resident of the same village she serves
- A woman (married/widow/divorced), preferably aged 25-45 years
- Minimum 8th standard education, with communication skills and leadership qualities
- Adequate representation from disadvantaged population groups
- General norm: 1 ASHA per 1,000 population; in tribal, hilly, and desert areas, the norm is relaxed to 1 ASHA per habitation
Core Roles and Responsibilities
1. Health Awareness and Education
- Nutrition, basic sanitation, and hygienic practices
- Healthy living and working conditions
- Existing health services and the need for timely utilization of health and family welfare services
2. Counselling in Prenatal and Maternal Health
- Birth preparedness and importance of safe delivery
- Breastfeeding and complementary feeding
- Immunization and contraception
- Prevention of reproductive tract infections (RTI) and sexually transmitted infections (STI)
- Care of the young child
3. Community Mobilization for ANC and PNC
- Antenatal check-ups at sub-centres and PHCs
- Postnatal check-ups
- Supplementary nutrition programs
- Immunization services at anganwadi centres and outreach sessions
4. Escorting Pregnant Women to Facilities
5. Village Health Planning
6. Primary Medical Care and Drug Depot
- Provides primary care for minor ailments (diarrhoea, fevers), first-aid for minor injuries
- Acts as a DOTS provider under the Revised National Tuberculosis Control Programme (RNTCP)
- Serves as a depot holder for essential supplies: ORS, IFA tablets, chloroquine, disposable delivery kits, oral pills, and condoms
- A drug kit (containing AYUSH and allopathic formulations) is provided to every ASHA
7. Disease Surveillance
- Reports births and deaths in her village to the sub-centre/PHC
- Reports unusual health problems and disease outbreaks in the community
8. Sanitation Promotion
- Promotes construction of household toilets under the Total Sanitation Campaign
ASHA's Role in Specific Prenatal Programs
Under Janani Suraksha Yojana (JSY)
- Making available institutional ANC and postnatal care
- Escorting pregnant women to health centres for delivery
- Facilitating cash assistance to beneficiaries
| Component | Amount |
|---|---|
| Cash incentive per delivery | Not less than Rs. 200 |
| Referral transport assistance | Not less than Rs. 250 |
| Balance payment at institution | Paid at hospital/health institution |
Under Home Based Newborn Care (HBNC)
- Institutional delivery: 6 visits (Day 3, 7, 14, 21, 28, 42)
- Home delivery: 7 visits (Day 1, 3, 7, 14, 21, 28, 42)
- C-section delivery: Full 5 visits from Day 7 to Day 42
- Recording of birth weight in the Mother and Child Protection Card
- Immunization with BCG, first OPV, Hep-B, and DPT/pentavalent vaccine
- Birth registration
- Both mother and newborn being safe until the 42nd day
- Twin deliveries: Rs. 500; triplets: Rs. 750
- Low birth weight babies followed up for 2 years (Rs. 50/month incentive)
- SNCU-discharged babies followed up for 1 year
Integration with the Health System (the "Triad")
ASHA - Anganwadi Worker (AWW) Integration
- AWW organizes Health Days (once/twice a month) at the anganwadi centre, where ASHA mobilizes women, adolescent girls, and children for orientation on: nutritious food, care during pregnancy, importance of ANC, and institutional delivery
- AWW acts as depot holder for ASHA's drug kits
- ASHA supports AWW in mobilizing pregnant and lactating women for nutrition supplements
- ASHA brings beneficiaries to anganwadi centres on immunization and health check-up days
ASHA - ANM Integration
- ANM holds weekly/fortnightly meetings with ASHA to review activities
- ANM informs ASHA of outreach session dates and guides beneficiary mobilization
- ANM guides ASHA on motivating pregnant women for: full IFA course, tetanus toxoid injections, ANC visits
- ANM educates ASHA on danger signs of pregnancy and labour so she can identify and refer cases timely
- ANM guides ASHA in motivating couples to adopt family planning
Summary: ASHA's Prenatal Role at a Glance
| Phase | ASHA's Key Function |
|---|---|
| Pre-pregnancy | Family planning counselling, eligible couple registration |
| Early pregnancy | Early registration of pregnancy, first ANC facilitation |
| Throughout pregnancy | ANC visit mobilization, IFA compliance, TT injection follow-up, danger sign identification, JSY registration |
| At delivery | Escort to facility, ensure institutional delivery |
| Postnatal (0-42 days) | HBNC visits, breastfeeding support, newborn immunization tracking, birth registration |
| Post-delivery | Long-term follow-up for LBW and SNCU-discharged newborns |
- Park's Textbook of Preventive and Social Medicine, pp. 514-521, 997-998
Epidemology
Epidemiological Methods & Study Designs
Classification of Epidemiological Studies
EPIDEMIOLOGICAL STUDIES
│
├── OBSERVATIONAL
│ ├── DESCRIPTIVE
│ │ ├── Cross-sectional (Prevalence) studies
│ │ ├── Longitudinal studies
│ │ ├── Case reports / Case series
│ │ └── Ecological (Correlational) studies
│ │
│ └── ANALYTICAL
│ ├── Case-Control (Retrospective) study
│ └── Cohort (Prospective / Longitudinal) study
│
└── EXPERIMENTAL
├── Randomized Controlled Trial (RCT)
├── Field trial
└── Community trial
1. Descriptive Epidemiology
Key variables studied:
- Person: Age, sex, ethnicity, marital status, occupation, social class, behaviour, stress, migration
- Place: Country, urban vs. rural, endemic zones, geographical clustering
- Time: Secular (long-term) trends, seasonal variation, epidemic patterns
Cross-Sectional Studies (Prevalence Studies)
- Based on a single examination of a cross-section of population at one point in time
- Also called a "photograph" of the population
- Provides prevalence data (not incidence)
- More useful for chronic than short-lived (acute) diseases
- Example: studying the distribution of hypertension in a population along with age, sex, body weight, salt intake simultaneously
- Limitation: Cannot establish time sequence (i.e., cannot prove causation); provides little information about natural history or incidence
Longitudinal Studies
- Observations are repeated in the same population over a prolonged period via follow-up examinations
- Compared to a "cine film" (vs. cross-sectional = photograph)
- Useful for:
- Studying natural history and future outcome of disease
- Identifying risk factors
- Finding incidence rate (new cases over time)
- More time-consuming and difficult to organize than cross-sectional studies
Ecological (Correlational) Studies
- Compare disease rates and exposure levels across populations or groups, not individuals
- Useful for generating hypotheses but subject to the ecological fallacy (group-level association may not apply to individuals)
2. Analytical Epidemiology
A. Case-Control Study (Retrospective Study)
- Both exposure and disease have occurred before the study starts
- Proceeds from effect → cause (retrospective)
- Uses a control/comparison group
The 2×2 Table (Framework)
| Suspected Risk Factor | Cases (Disease +) | Controls (Disease -) |
|---|---|---|
| Present | a | b |
| Absent | c | d |
| Total | a + c | b + d |
- Odds Ratio (OR) = ad/bc (measure of association)
- OR > 1 = exposure associated with increased disease risk
Four Basic Steps:
- Selection of cases and controls
- Matching (to control confounding)
- Measurement of exposure
- Analysis and interpretation
Selection of Cases:
- Diagnostic criteria must be pre-defined (e.g., histologically confirmed cancer)
- Eligibility criteria: Prefer newly diagnosed (incident) cases over old/prevalent cases
- Sources: Hospitals (convenient) or General population (population-based, less bias)
Selection of Controls:
- Must be free from the disease under study
- Should be comparable to cases in all relevant variables except the exposure
- Sources: Hospital controls, neighbourhood controls, relatives, etc.
Matching (Controlling Confounding):
- A confounding factor is one that is associated both with exposure and with disease, and is unequally distributed between cases and controls
- Classic example: In studying alcohol and oesophageal cancer, smoking is a confounding factor (associated with both alcohol use and oesophageal cancer)
- Types of matching:
- Group/frequency matching: Distribute matched variables equally across strata
- Pair matching: Each case is matched with one control on specific variables (e.g., age, sex, occupation)
- Caution: Do NOT match on the suspected aetiological factor itself - this eliminates the ability to study that factor
Advantages of Case-Control Studies:
- Relatively quick and inexpensive
- Suitable for rare diseases
- Can study multiple exposures simultaneously
- No risk to subjects
- No follow-up required
Disadvantages:
- Recall bias (cases recall past exposure differently than controls)
- Selection bias in choosing controls
- Cannot calculate incidence or relative risk directly (only OR)
- Difficult to validate exposure information
- Not suitable for rare exposures
B. Cohort Study (Prospective / Longitudinal Study)
- Cohorts identified before disease appears
- Study groups observed over time for disease frequency
- Proceeds from cause → effect (prospective)
Concept of a Cohort:
- Birth cohort: All persons born in the same year (e.g., birth cohort of 2010)
- Exposure cohort: Persons exposed to a drug, vaccine, or infection within a defined period
- Marriage cohort: Persons married in the same period
Framework:
| Cohort | Disease (Yes) | Disease (No) | Total |
|---|---|---|---|
| Exposed | a | b | a+b |
| Not Exposed | c | d | c+d |
- Relative Risk (RR) = [a/(a+b)] ÷ [c/(c+d)]
- RR > 1 = exposure associated with increased disease risk
Assembling the Cohort - Key Principles:
- Both cohorts must be free from the disease at study start
- Both groups should be equally susceptible to the disease
- Both groups must be comparable for all confounding variables
- Diagnostic and eligibility criteria defined beforehand
Indications for Cohort Studies:
- Good preliminary evidence of exposure-disease association (from descriptive or case-control studies)
- Exposure is rare but incidence of disease is high among exposed (e.g., industrial exposures, X-ray radiologists)
- Attrition can be minimized (stable, cooperative, accessible cohort)
- Ample funds available
Types of Cohort Sources:
- Special groups: Occupational groups, insurance policyholders (homogeneous, accessible, easy follow-up)
- Exposure groups: Workers in high-risk industries, radiologists exposed to X-rays
Data Collection in Cohort Studies:
- Cohort members - personal interviews or mailed questionnaires (e.g., Doll & Hill used mailed questionnaires to collect smoking histories from British doctors)
- Review of records - medical records (radiation dose, surgical details)
- Medical examination/special tests - BP, serum cholesterol, ECG
- Environmental surveys - exposure levels in the environment
Advantages of Cohort Studies:
- Can calculate true incidence and relative risk
- Establishes temporal sequence (exposure before disease)
- Can study multiple outcomes of a single exposure
- Less subject to bias in exposure measurement
- Provides complete data on the natural history of disease
Disadvantages:
- Expensive and time-consuming (especially for chronic diseases)
- Large numbers required
- Attrition (loss to follow-up) can bias results
- Not suitable for rare diseases
- Exposure status or habits may change during follow-up
Case-Control vs. Cohort - Key Comparison
| Feature | Case-Control | Cohort |
|---|---|---|
| Direction | Retrospective (effect → cause) | Prospective (cause → effect) |
| Starting point | Disease (cases) | Exposure status |
| Measure of association | Odds Ratio (OR) | Relative Risk (RR) |
| Incidence measurable? | No | Yes |
| Time & cost | Less | More |
| Suitable for rare disease? | Yes | No |
| Suitable for rare exposure? | No | Yes |
| Bias risk | Recall bias, selection bias | Attrition bias |
| Classic example | Thalidomide and birth defects | Doll & Hill study on smoking & lung cancer |
3. Experimental Studies (Interventional)
Randomized Controlled Trial (RCT)
- Gold standard for testing interventions (drugs, vaccines, procedures)
- Participants randomly allocated to treatment or control group
- Randomization controls for both known and unknown confounders
- Can be blinded (single, double, triple blind) to reduce bias
Field Trials
- Conducted in the general community rather than clinical settings
- Used to evaluate preventive measures (e.g., vaccine efficacy in healthy people)
Community Trials
- The unit of randomization and intervention is a community, not an individual
- Used when the intervention must be applied at a population level (e.g., water fluoridation)
Evidence Hierarchy (Pyramid)
▲ STRONGEST
│
│ Systematic Reviews & Meta-analyses
│ Randomized Controlled Trials (RCTs)
│ Cohort Studies
│ Case-Control Studies
│ Cross-Sectional Studies
│ Case Reports / Case Series
│ Expert Opinion / Editorials
▼ WEAKEST
Key Measures Used in Epidemiological Studies
| Measure | Formula | Used In |
|---|---|---|
| Incidence Rate | New cases / Population at risk × time | Cohort |
| Prevalence | All cases / Total population at a point in time | Cross-sectional |
| Relative Risk (RR) | Incidence in exposed / Incidence in unexposed | Cohort |
| Odds Ratio (OR) | (a×d) / (b×c) | Case-control |
| Attributable Risk | Incidence in exposed - Incidence in unexposed | Cohort |
| Population Attributable Risk | Incidence in total pop. - Incidence in unexposed | Cohort |
Search for recent examples of each study design in PubMed
"cross-sectional study"[pt] OR "cross-sectional"[tiab]
"case-control study"[MeSH Terms]
"cohort study"[MeSH Terms] AND "prospective studies"[MeSH Terms]
"randomized controlled trial"[pt] AND "double-blind"[tiab]
"systematic review"[pt] AND "meta-analysis"[pt]
"cohort study" AND "prospective"
"case-control study" AND "risk factor"
"cross-sectional study" AND "prevalence"
PMID: 40081632
PMID: 40520452
PMID: 39794615
PMID: 42297908
PMID: 39531790
Recent PubMed Examples of Each Study Design
1. Cross-Sectional Study (Prevalence Study)
- Enrolled 9,673 US adults from the NHANES database (2011-2020) at a single point in time
- Measured TyG-BMI (an insulin resistance surrogate) and depression prevalence (PHQ-9 scale) simultaneously
- Applied multivariate logistic regression to assess association
- Single examination of a population snapshot (one time point)
- Measures prevalence, not incidence
- Exposure (TyG-BMI) and outcome (depression) measured simultaneously
- Cannot establish temporal sequence - which came first, insulin resistance or depression, cannot be determined
2. Case-Control Study (Retrospective)
- Cases: 13,554 patients diagnosed with microscopic colitis (MC) in Sweden (1981-2017), sourced from Swedish pathology registers
- Controls: 64,886 controls randomly selected from the general population, matched for birth year, sex, county of residence, and calendar year
- Looked backwards at prior cholecystectomy rates in both groups
- Calculated Adjusted Odds Ratios (aOR) using conditional logistic regression
- Both exposure (cholecystectomy) and outcome (MC) had already occurred
- Proceeds effect → cause (retrospective)
- Uses matched controls to isolate the exposure variable
- Matching variables: birth year, sex, county, calendar year (to control confounding)
- Outcome measure: Odds Ratio
3. Prospective Cohort Study
- Enrolled 103,449 participants from the UK Biobank (aged 40-69, recruited 2006-2010), all free of acute pancreatitis at baseline
- Measured Mediterranean Diet (MedDiet) adherence via 24-h dietary recalls at the start
- Followed participants for a mean 10.4 years, identifying incident acute pancreatitis (AP) cases through electronic medical records
- Used Cox proportional hazards models to calculate Hazard Ratios (HR)
- Also assessed interaction with genetic risk (polygenic risk score)
- Cohort was identified before disease appeared (no AP at baseline)
- Proceeds cause → effect (exposure measured first, then disease tracked)
- True incidence (371 new cases over 10.4 years) was measured
- Measure of association: Relative Risk / Hazard Ratio (not Odds Ratio)
- Long follow-up period - characteristic of cohort studies for chronic/non-communicable diseases
4. Randomized Controlled Trial (RCT)
- 28 adults with Type 1 diabetes were randomly allocated to receive either weekly semaglutide (up to 1 mg) OR placebo as adjunct to an automated insulin delivery (AID) system
- Double-blind design: neither participants nor assessors knew the allocation
- Crossover design: each participant received both interventions in different periods (acts as their own control)
- Primary outcome: % time spent in glucose target range (3.9-10.0 mmol/L) during the last 4 weeks of each intervention
- Investigator controls the exposure (not just observes)
- Participants randomly assigned to intervention or control (controls confounding)
- Double blinding eliminates observer and performance bias
- The gold standard for testing therapeutic interventions
- ClinicalTrials.gov registered: NCT05205928
5. Systematic Review & Meta-Analysis
- Searched PubMed, EMBASE, and Scopus up to April 2025
- Identified 226 articles comprising 1.5 million incident cancers from prospective studies across 25 cancer types
- Pooled data from multiple individual studies using meta-analytic methods to calculate summary effect estimates
- BMI was positively associated with risk of 19 cancers and inversely associated with 3
- New associations identified: leukaemia, non-Hodgkin lymphoma, bladder cancer, glioma
- Associations varied by region and sex (e.g., stronger for postmenopausal breast cancer in East Asia)
- Genetic (Mendelian randomization) findings were consistent with observational associations
- Systematically searched multiple databases with pre-defined criteria
- Pooled data across studies to generate a single summary estimate with greater statistical power
- Represents the top of the evidence hierarchy - synthesizes the best available evidence
- Can detect associations and subgroup differences not visible in individual studies
Summary Table
| Study Design | Example Paper | PMID | Key Measure | Direction |
|---|---|---|---|---|
| Cross-sectional | TyG-BMI & depression (NHANES) | 39531790 | Prevalence OR | Simultaneous |
| Case-control | Cholecystectomy & microscopic colitis | 40081632 | Odds Ratio 2.36 | Retrospective (effect → cause) |
| Prospective cohort | Mediterranean diet & pancreatitis | 40520452 | Hazard Ratio 0.60 | Prospective (cause → effect) |
| RCT (double-blind crossover) | Semaglutide in T1DM | 39794615 | Mean difference +4.8% TIR | Randomized/Experimental |
| Systematic Review + Meta-analysis | Adiposity & 25 cancer types | 42297908 | Pooled RR/HR across 226 studies | Highest evidence level |
Get me singhi pdf of 3rd yr rguhs examination
- Copyright infringement - these are commercially published books/materials protected under copyright law
- Distributing exam-related materials that may include previous question papers in ways not authorized by the publisher or university
- Explain any topic from your 3rd year MBBS syllabus (PSM/Community Medicine, Pharmacology, Pathology, Microbiology, Forensic Medicine, ENT, Ophthalmology) using authoritative medical textbooks in my library
- Answer practice questions and explain the reasoning behind correct answers
- Summarize high-yield topics for RGUHS 3rd year examinations based on the standard curriculum
- Search PubMed for evidence-based content on any clinical topic you're studying
Create a study guide for a specific 3rd year subject
RGUHS 3rd year MBBS community medicine PSM syllabus topics high yield exam 2024
Community Medicine (PSM) - 3rd Year MBBS
Short Notes Study Guide | RGUHS
Syllabus coverage: Based on RGUHS Phase III Part I curriculum + high-yield topics for university theory exams. Reference: Park's Textbook of Preventive and Social Medicine
UNIT 1: EPIDEMIOLOGY
1.1 Study Designs (Short Note)
| Type | Key Feature | Direction | Measure |
|---|---|---|---|
| Cross-sectional | Single time point, prevalence | Simultaneous | Prevalence |
| Case-Control | Effect → Cause | Retrospective | Odds Ratio |
| Cohort | Cause → Effect | Prospective | Relative Risk |
| RCT | Randomized intervention | Experimental | Risk difference |
1.2 Screening (Short Note) ⭐ High Yield
| Disease + | Disease - | |
|---|---|---|
| Test + | a (TP) | b (FP) |
| Test - | c (FN) | d (TN) |
- Sensitivity = a/(a+c) × 100 — ability to detect true positives ("Positive in Disease" = PID)
- Specificity = d/(b+d) × 100 — ability to exclude true negatives ("Negative in Health" = NIH)
- PPV = a/(a+b) — probability that a positive test = true disease
- NPV = d/(c+d) — probability that a negative test = truly disease-free
- Important health problem
- Natural history known
- Recognisable latent or early symptomatic stage
- Suitable test available
- Test acceptable to population
- Agreed policy on whom to treat
- Facilities for diagnosis and treatment available
- Recognised treatment for disease
- Cost-benefit favourable
- Case-finding continuous process
1.3 Measures of Disease Frequency (Short Note) ⭐ Very High Yield
- High incidence + short duration = low prevalence (e.g., common cold)
- Low incidence + long duration = high prevalence (e.g., diabetes, leprosy)
1.4 Epidemic Investigation (Short Note)
- Verify the diagnosis
- Confirm the epidemic
- Define a case (case definition)
- Find cases systematically (active case search)
- Tabulate by person, place, time
- Plot epidemic curve
- Formulate hypothesis
- Test hypothesis
- Control and prevention measures
- Point source (common source): Single exposure, sharp rise and fall within one incubation period - e.g., food poisoning
- Propagated (person-to-person): Multiple waves, each separated by one incubation period - e.g., measles in a school
- Mixed: Starts as common source, then person-to-person spread
UNIT 2: BIOSTATISTICS
2.1 Measures of Central Tendency (Short Note) ⭐ High Yield
| Measure | Definition | When to use | Affected by extreme values? |
|---|---|---|---|
| Mean | Sum/n | Normal distribution | Yes |
| Median | Middle value | Skewed distribution | No |
| Mode | Most frequent value | Qualitative/nominal data | No |
- ±1 SD covers 68.27% of values
- ±2 SD covers 95.45% of values
- ±3 SD covers 99.73% of values
- Positive skew (right): Mean > Median > Mode (tail on right)
- Negative skew (left): Mean < Median < Mode (tail on left)
2.2 Statistical Tests (Short Note) ⭐ High Yield
| Test | Used when | Data type |
|---|---|---|
| Student's t-test | Comparing 2 means (small samples) | Continuous |
| ANOVA (F-test) | Comparing 3+ means | Continuous |
| Chi-square (χ²) | Comparing proportions / association | Categorical |
| Paired t-test | Before/after same group | Continuous |
| Correlation (r) | Relationship between 2 variables | Continuous |
2.3 Sampling Methods (Short Note)
| Method | Description |
|---|---|
| Simple random | Each unit has equal probability of selection |
| Systematic | Every nth unit (k = N/n) |
| Stratified | Population divided into strata; random sample from each |
| Cluster | Natural groups (villages) selected; all in selected cluster studied |
| Multistage | Combination of above methods |
| Purposive/Judgement | Non-probability; investigator selects |
UNIT 3: DEMOGRAPHY & VITAL STATISTICS
3.1 Vital Statistics - Key Definitions ⭐ Very High Yield
| Indicator | Formula | India value (NFHS-5 2019-21) |
|---|---|---|
| Crude Birth Rate (CBR) | Live births per 1000 mid-year population | ~20 |
| Crude Death Rate (CDR) | Deaths per 1000 mid-year population | ~6 |
| Infant Mortality Rate (IMR) | Deaths under 1 year per 1000 live births | 35.2 |
| Neonatal Mortality Rate (NMR) | Deaths in 0-28 days per 1000 live births | 25.5 |
| Perinatal Mortality Rate | (Stillbirths + deaths <7 days) per 1000 births | - |
| Maternal Mortality Ratio (MMR) | Maternal deaths per 100,000 live births | 97 |
| Total Fertility Rate (TFR) | Average children per woman | 2.0 |
| Replacement TFR | TFR needed for population replacement | 2.1 |
3.2 Demographic Cycle (Transition) (Short Note) ⭐ High Yield
| Stage | Birth Rate | Death Rate | Population Growth | Example |
|---|---|---|---|---|
| I - High stationary | High | High | Stable (low) | Pre-industrial societies |
| II - Early expanding | High | Falling | Rapid increase | India 1921-1951 |
| III - Late expanding | Falling | Low | Slowing | India currently |
| IV - Low stationary | Low | Low | Stable (low) | Developed countries |
| V - Declining | Low | Low | Declining | Some European countries |
UNIT 4: ENVIRONMENT & HEALTH
4.1 Water - Standards & Purification (Short Note) ⭐ High Yield
- Storage / Sedimentation (removes 75-90% bacteria)
- Coagulation / Flocculation (alum 5-40 mg/L)
- Filtration (slow sand filter - removes 98-99% bacteria)
- Disinfection (chlorination)
4.2 Air Pollution (Short Note)
| Pollutant | Source | Health Effect |
|---|---|---|
| CO | Incomplete combustion | Cherry-red appearance, COHb, death |
| SO₂ | Coal/oil combustion | Bronchospasm, acid rain |
| NO₂ | Traffic, industry | Pulmonary oedema (brown fumes) |
| Particulate matter (PM₂.₅) | Vehicles, industry | Pneumoconiosis, lung cancer |
| Lead | Petrol (leaded), paint | Encephalopathy, anaemia |
| Ozone | Photochemical smog | Eye/lung irritation |
4.3 Solid Waste Management (Short Note)
- Yellow bag: Anatomical/pathological waste - incineration
- Red bag: Contaminated recyclable waste - autoclaving
- Blue/White container: Sharps - puncture-proof, shredding/encapsulation
- Black bag: General waste - landfill
UNIT 5: NUTRITION
5.1 Protein-Energy Malnutrition (PEM) (Short Note) ⭐ Very High Yield
| Feature | Kwashiorkor | Marasmus |
|---|---|---|
| Cause | Protein deficiency (adequate calories) | Overall calorie deficiency |
| Age | 1-5 years | < 1 year |
| Weight | Moderately reduced | Severely reduced (<60% expected) |
| Oedema | Present (pitting) | Absent |
| Appearance | Moon face, pot belly, skin lesions, flaky paint dermatosis | "Old man face", baggy pants, skin and bones |
| Hair | Reddish/brown, flag sign, easily pluckable | Sparse |
| Fatty liver | Present | Absent |
| Serum albumin | Very low | Normal/slightly low |
| Appetite | Poor | Good |
5.2 Vitamin Deficiency Diseases (Short Note) ⭐ High Yield
| Vitamin | Deficiency Disease | Key Features |
|---|---|---|
| A (Retinol) | Xerophthalmia | Night blindness, Bitot's spots, keratomalacia |
| B1 (Thiamine) | Beriberi | Dry (peripheral neuropathy), Wet (cardiomyopathy), Wernicke-Korsakoff |
| B2 (Riboflavin) | Ariboflavinosis | Cheilosis, angular stomatitis, corneal vascularisation |
| B3 (Niacin) | Pellagra | 4 D's: Dermatitis, Diarrhoea, Dementia, Death. Maize diet |
| B12 | Megaloblastic anaemia | Macrocytic anaemia, subacute combined degeneration of cord |
| C (Ascorbic acid) | Scurvy | Perifollicular haemorrhage, bleeding gums, corkscrew hairs |
| D (Calciferol) | Rickets (children) / Osteomalacia (adults) | Craniotabes, bow legs, Harrison's sulcus |
| K | Haemorrhagic disease of newborn | Prolonged PT |
5.3 Iodine Deficiency Disorders (IDD) (Short Note)
- Spectrum: Goitre, cretinism, deaf-mutism, hypothyroidism, mental retardation
- Most sensitive indicator of IDD: Urinary iodine excretion
- Prevention: Iodized salt (30 ppm at production, 15 ppm at consumer level)
- National Iodine Deficiency Disorders Control Programme (NIDDCP): All edible salt to be iodized in India
UNIT 6: MATERNAL & CHILD HEALTH
6.1 Antenatal Care Schedules (Short Note) ⭐ High Yield
- 1st: Within 12 weeks
- 2nd: 14-26 weeks
- 3rd: 28-34 weeks
- 4th: 36 weeks to term
- TT-1: Early pregnancy; TT-2: 4 weeks after TT-1; TT-booster: if previously immunized
- IFA: 1 tablet daily from 12 weeks (100 mg elemental iron + 500 mcg folic acid)
6.2 Immunization Schedule (Short Note) ⭐ Very High Yield
| Age | Vaccines |
|---|---|
| Birth | BCG, OPV-0, Hep-B₁ |
| 6 weeks | OPV-1, Penta-1 (DPT+HepB+Hib), IPV-1, Rota-1, fIPV-1 |
| 10 weeks | OPV-2, Penta-2, Rota-2 |
| 14 weeks | OPV-3, Penta-3, IPV-2, Rota-3, fIPV-2 |
| 9 months | MR-1, JE-1 (endemic areas), Vit A-1 |
| 16-24 months | MR-2, DPT booster-1, OPV booster, JE-2, Vit A-2 |
| 5-6 years | DPT booster-2 |
| 10 years | Td |
| 16 years | Td |
UNIT 7: NATIONAL HEALTH PROGRAMS
7.1 Key National Programs at a Glance ⭐ Very High Yield
| Program | Year | Key Feature |
|---|---|---|
| RNTCP (Revised National TB Control Programme) → now NTEP | 1997 / 2020 | DOTS strategy; Nikshay portal; TB free India by 2025 |
| NVBDCP (National Vector Borne Disease Control Programme) | 2003 (merged) | Covers malaria, dengue, filaria, kala-azar, JE, chikungunya |
| NACP (National AIDS Control Programme) | Phase I: 1992 | ART, ICTC, PPTCT |
| NLEP (National Leprosy Eradication Programme) | 1983 | MDT; elimination achieved <1/10,000 in 2005 |
| NPCB (National Programme for Control of Blindness) | 1976 | Cataract surgery, school eye screening |
| NHM (National Health Mission) | 2013 (NRHM 2005) | ASHA, free drugs, JSY, JSSK |
| NPCDCS | 2010 | NCD screening (diabetes, hypertension, cancer) |
7.2 RNTCP / NTEP - Short Notes ⭐ High Yield
- Category I (new cases): 2(HRZE)/4(HR) - 6 months
- Category II (previously treated): 2(HRZES)/1(HRZE)/5(HRE) - 8 months
- NTEP (2020): All new cases get 4-drug fixed dose combination (FDC): HRZE for 2 months, HR for 4 months
- Sputum smear microscopy (ZN stain, fluorescence microscopy)
- CBNAAT (Cartridge Based Nucleic Acid Amplification Test) - rapid diagnosis + detects RIF resistance
- Culture: Gold standard (LJ medium)
7.3 Malaria - Short Notes ⭐ High Yield
- P. vivax: Chloroquine + Primaquine (14 days)
- P. falciparum: Artemisinin-based Combination Therapy (ACT) + Primaquine (single dose)
UNIT 8: HEALTH EDUCATION & COMMUNICATION
8.1 Health Education Methods (Short Note)
- Assess the problem and community needs
- Identify target population
- Set objectives
- Select appropriate methods and media
- Implement
- Evaluate
8.2 Socioeconomic Status (SES) Scales (Short Note) ⭐ High Yield
| Scale | Components | Update |
|---|---|---|
| B.G. Prasad (urban/rural) | Per capita monthly income | Updated periodically using CPI |
| Kuppuswamy (urban) | Education + Occupation + Income | Updated using CPI (for income) |
| Uday Pareek (rural) | Standard of living, education, occupation, caste, land, housing, economic status | Rural specific |
- Class I: Upper; Class II: Upper middle; Class III: Middle; Class IV: Lower middle; Class V: Lower
UNIT 9: OCCUPATIONAL HEALTH
9.1 Occupational Lung Diseases (Short Note) ⭐ High Yield
| Disease | Causative dust | Occupation |
|---|---|---|
| Silicosis | Free silica (SiO₂) | Mining, stone cutting, glass industry |
| Anthracosis (Coal workers' pneumoconiosis) | Coal dust | Coal mining |
| Asbestosis | Asbestos fibres | Asbestos mining, lagging, shipbuilding |
| Bagassosis | Bagasse (sugarcane waste) | Sugar industry |
| Byssinosis | Cotton dust | Cotton textile workers |
| Farmer's lung | Thermophilic actinomycetes (mouldy hay) | Farmers |
| Siderosis | Iron oxide | Welders, iron miners |
UNIT 10: NON-COMMUNICABLE DISEASES
10.1 Epidemiology of Hypertension (Short Note) ⭐ High Yield
- Normal: < 120/80 mmHg
- Pre-hypertension: 120-139/80-89
- Stage 1 HTN: 140-159/90-99
- Stage 2 HTN: ≥160/≥100
10.2 Epidemiology of Diabetes Mellitus (Short Note)
- Fasting plasma glucose ≥ 126 mg/dL
- 2-hr post-glucose ≥ 200 mg/dL (OGTT)
- Random plasma glucose ≥ 200 mg/dL + symptoms
- HbA1c ≥ 6.5%
QUICK REVISION TABLE: Exam Frequently Asked Short Notes
| Topic | Key Fact to Remember |
|---|---|
| Incubation period of cholera | Few hours to 5 days |
| Herd immunity threshold for measles | 95% |
| Cold chain temperature | +2°C to +8°C |
| Replacement level TFR | 2.1 |
| Safe residual chlorine | 0.5 mg/L |
| Optimal fluoride level | 0.5-0.8 mg/L (India) |
| IMR definition | Deaths <1 year per 1000 live births |
| MMR definition | Maternal deaths per 100,000 live births |
| Sensitivity formula | TP/(TP+FN) × 100 |
| Specificity formula | TN/(TN+FP) × 100 |
| Chi-square test used for | Comparison of proportions (categorical data) |
| Kwashiorkor vs Marasmus - oedema | Kwashiorkor = oedema present |
| Pellagra associated diet | Maize diet (niacin deficiency) |
| Nikshay portal | National TB notification system |
| ASHA norm | 1 per 1000 population |
| VVM discard criteria | Inner square darker than outer circle |
| JSY launched | April 2005 |
| JSSK launched | June 2011 |
| PMSMA | Free ANC on 9th of every month |
Tip: This guide covers ~80% of expected short note questions in RGUHS 3rd year theory papers. For LAQs (Long Answer Questions), expand on Epidemiology (study designs + epidemic investigation), National Health Programs (RNTCP/NTEP, Malaria, Immunization), and Biostatistics (statistical tests + sampling). Ask me to expand any section!
Generate a PDF study guide of this short notes for offline access
ls /home/daytona/workspace/ 2>/dev/null && echo "---" && python3 -c "import repo…
mkdir -p /home/daytona/workspace/psm-study-guide && echo "dir created"
~/psm-study-guide/generate_pdf.py
from reportlab.lib.pagesizes import A4
from reportlab.lib.styles import getSampleStyleSheet, ParagraphStyle
from reportlab.lib.units import cm
from reportlab.lib.colors import HexColor, white, black
from reportlab.platypus import (
SimpleDocTemplate, Paragraph, Spacer, Table, TableStyle,
HRFlowable, KeepTogether, PageBreak
)
from reportlab.lib.enums import TA_LEFT, TA_CENTER, TA_RIGHT
from reportlab.lib import colors
OUTPUT = "/home/daytona/workspace/psm-study-guide/PSM_ShortNotes_RGUHS_3rdYear.pdf"
# ── Colours ──────────────────────────────────────────────────────────────────
C_NAVY = HexColor("#1a3560")
C_TEAL = HexColor("#0d7377")
C_ORANGE = HexColor("#e05e00")
C_YELLOW = HexColor("#fff4cc")
C_LIGHTBLUE= HexColor("#e8f4f8")
C_GREY = HexColor("#f5f5f5")
C_DARKGREY = HexColor("#555555")
C_RED = HexColor("#c0392b")
C_GREEN = HexColor("#1e7a3c")
C_WHITE = white
# ── Styles ────────────────────────────────────────────────────────────────────
def make_styles():
base = getSampleStyleSheet()
styles = {}
styles['cover_title'] = ParagraphStyle('cover_title',
fontName='Helvetica-Bold', fontSize=26, textColor=C_WHITE,
alignment=TA_CENTER, spaceAfter=8, leading=32)
styles['cover_sub'] = ParagraphStyle('cover_sub',
fontName='Helvetica', fontSize=13, textColor=C_WHITE,
alignment=TA_CENTER, spaceAfter=4, leading=18)
styles['h1'] = ParagraphStyle('h1',
fontName='Helvetica-Bold', fontSize=14, textColor=C_WHITE,
alignment=TA_LEFT, spaceBefore=10, spaceAfter=4,
leftIndent=0, leading=18,
backColor=C_NAVY, borderPad=6)
styles['h2'] = ParagraphStyle('h2',
fontName='Helvetica-Bold', fontSize=11, textColor=C_TEAL,
spaceBefore=10, spaceAfter=3, leading=14)
styles['h3'] = ParagraphStyle('h3',
fontName='Helvetica-BoldOblique', fontSize=10, textColor=C_ORANGE,
spaceBefore=6, spaceAfter=2, leading=13)
styles['body'] = ParagraphStyle('body',
fontName='Helvetica', fontSize=9, textColor=black,
spaceBefore=2, spaceAfter=2, leading=13, leftIndent=10)
styles['bullet'] = ParagraphStyle('bullet',
fontName='Helvetica', fontSize=9, textColor=black,
spaceBefore=1, spaceAfter=1, leading=12,
leftIndent=20, bulletIndent=10)
styles['note'] = ParagraphStyle('note',
fontName='Helvetica-Oblique', fontSize=8.5, textColor=C_DARKGREY,
spaceBefore=2, spaceAfter=2, leading=12, leftIndent=10)
styles['highlight'] = ParagraphStyle('highlight',
fontName='Helvetica-Bold', fontSize=9, textColor=C_RED,
spaceBefore=1, spaceAfter=1, leading=12, leftIndent=10)
styles['footer'] = ParagraphStyle('footer',
fontName='Helvetica', fontSize=7.5, textColor=C_DARKGREY,
alignment=TA_CENTER)
return styles
S = make_styles()
# ── Helper: section heading block ─────────────────────────────────────────────
def unit_heading(text):
tbl = Table([[Paragraph(f' {text}', S['h1'])]], colWidths=[17.5*cm])
tbl.setStyle(TableStyle([
('BACKGROUND', (0,0), (-1,-1), C_NAVY),
('ROUNDEDCORNERS', [4,4,4,4]),
('TOPPADDING', (0,0),(-1,-1), 6),
('BOTTOMPADDING', (0,0),(-1,-1), 6),
('LEFTPADDING', (0,0),(-1,-1), 8),
]))
return tbl
def sub_heading(text):
return Paragraph(f'● {text}', S['h2'])
def sub_sub_heading(text):
return Paragraph(text, S['h3'])
def body(text):
return Paragraph(text, S['body'])
def bullet(text):
return Paragraph(f'• {text}', S['bullet'])
def note(text):
return Paragraph(f'<i>{text}</i>', S['note'])
def highlight(text):
return Paragraph(f'⭐ {text}', S['highlight'])
def spacer(h=4):
return Spacer(1, h)
def hr():
return HRFlowable(width="100%", thickness=0.5, color=C_TEAL, spaceAfter=4)
# ── Generic data table ─────────────────────────────────────────────────────────
def data_table(headers, rows, col_widths=None):
data = [headers] + rows
if col_widths is None:
n = len(headers)
col_widths = [17.5*cm / n] * n
tbl = Table(data, colWidths=col_widths, repeatRows=1)
style = TableStyle([
# header row
('BACKGROUND', (0,0), (-1,0), C_TEAL),
('TEXTCOLOR', (0,0), (-1,0), C_WHITE),
('FONTNAME', (0,0), (-1,0), 'Helvetica-Bold'),
('FONTSIZE', (0,0), (-1,0), 8.5),
('ALIGN', (0,0), (-1,0), 'CENTER'),
('BOTTOMPADDING', (0,0), (-1,0), 5),
('TOPPADDING', (0,0), (-1,0), 5),
# data rows
('FONTNAME', (0,1), (-1,-1), 'Helvetica'),
('FONTSIZE', (0,1), (-1,-1), 8),
('ROWBACKGROUNDS',(0,1), (-1,-1), [C_WHITE, C_GREY]),
('GRID', (0,0), (-1,-1), 0.4, C_DARKGREY),
('ALIGN', (0,0), (-1,-1), 'LEFT'),
('VALIGN', (0,0), (-1,-1), 'MIDDLE'),
('TOPPADDING', (0,1), (-1,-1), 4),
('BOTTOMPADDING', (0,1), (-1,-1), 4),
('LEFTPADDING', (0,0), (-1,-1), 5),
])
tbl.setStyle(style)
return tbl
# ── Yellow callout box ─────────────────────────────────────────────────────────
def callout(text, bg=None):
bg = bg or C_YELLOW
p = Paragraph(text, ParagraphStyle('cb', fontName='Helvetica', fontSize=8.5,
leading=13, leftIndent=4, rightIndent=4))
t = Table([[p]], colWidths=[17*cm])
t.setStyle(TableStyle([
('BACKGROUND', (0,0),(-1,-1), bg),
('BOX', (0,0),(-1,-1), 0.8, C_ORANGE),
('TOPPADDING', (0,0),(-1,-1), 6),
('BOTTOMPADDING', (0,0),(-1,-1), 6),
('LEFTPADDING', (0,0),(-1,-1), 8),
]))
return t
# ── Cover page ─────────────────────────────────────────────────────────────────
def cover_page():
elements = []
# big blue banner
banner_para = Paragraph(
'<b>COMMUNITY MEDICINE (PSM)</b><br/>'
'Short Notes Study Guide',
ParagraphStyle('bn', fontName='Helvetica-Bold', fontSize=22,
textColor=C_WHITE, alignment=TA_CENTER, leading=30))
banner = Table([[banner_para]], colWidths=[17.5*cm])
banner.setStyle(TableStyle([
('BACKGROUND', (0,0),(-1,-1), C_NAVY),
('TOPPADDING', (0,0),(-1,-1), 28),
('BOTTOMPADDING', (0,0),(-1,-1), 28),
]))
elements.append(banner)
elements.append(spacer(14))
meta = [
['3rd Year MBBS | RGUHS Curriculum'],
['Reference: Park\'s Textbook of Preventive & Social Medicine'],
['Units Covered: Epidemiology • Biostatistics • Demography'],
['Environment • Nutrition • MCH • National Programs'],
['Occupational Health • Non-Communicable Diseases'],
]
for m in meta:
elements.append(Paragraph(m[0], ParagraphStyle('meta',
fontName='Helvetica', fontSize=10, textColor=C_NAVY,
alignment=TA_CENTER, spaceAfter=3)))
elements.append(spacer(16))
elements.append(HRFlowable(width='80%', thickness=1.5, color=C_TEAL,
hAlign='CENTER', spaceAfter=14))
tip = (
'<b>How to use this guide:</b> Each unit covers one major PSM topic. '
'Short-note format is optimised for RGUHS theory paper revision. '
'⭐ marks denote very high-yield exam topics.'
)
elements.append(callout(tip, bg=C_LIGHTBLUE))
elements.append(PageBreak())
return elements
# ── CONTENT ───────────────────────────────────────────────────────────────────
def content():
el = []
# ── UNIT 1: EPIDEMIOLOGY ──────────────────────────────────────────────────
el += [unit_heading('UNIT 1: EPIDEMIOLOGY'), spacer()]
el += [sub_heading('1.1 Study Designs'), spacer(2)]
el.append(data_table(
['Design', 'Direction', 'Starts With', 'Measure', 'Best For'],
[
['Cross-sectional', 'Simultaneous', 'Population snapshot', 'Prevalence', 'Chronic disease distribution'],
['Case-Control', 'Retrospective\n(effect→cause)', 'Disease (cases)', 'Odds Ratio (OR)', 'Rare diseases'],
['Cohort', 'Prospective\n(cause→effect)', 'Exposure status', 'Relative Risk (RR)', 'Rare exposures'],
['RCT', 'Experimental', 'Randomised groups', 'Risk difference', 'Testing interventions'],
],
col_widths=[3.2*cm, 3.2*cm, 3.5*cm, 3.2*cm, 4.4*cm]
))
el.append(spacer(4))
el += [
highlight('Cross-sectional = "photograph" — gives prevalence only, cannot prove causation'),
bullet('Case-Control: OR = ad/bc from 2×2 table'),
bullet('Cohort: RR = [a/(a+b)] ÷ [c/(c+d)] — can measure true incidence'),
bullet('RCT: Gold standard. Randomisation controls known + unknown confounders'),
bullet('Classic cohort: Doll & Hill — smoking and lung cancer (British doctors)'),
]
el.append(spacer())
el += [sub_heading('1.2 Screening Tests ⭐'), spacer(2)]
screen_tbl = data_table(
['Measure', 'Formula', 'Mnemonic'],
[
['Sensitivity', 'TP / (TP + FN) × 100', 'PID — Positive In Disease'],
['Specificity', 'TN / (TN + FP) × 100', 'NIH — Negative In Health'],
['PPV', 'TP / (TP + FP) × 100', 'Positive test = true disease?'],
['NPV', 'TN / (TN + FN) × 100', 'Negative test = truly healthy?'],
],
col_widths=[4.5*cm, 7*cm, 6*cm]
)
el.append(screen_tbl)
el.append(spacer(4))
el += [
bullet('High cut-off → ↑ Specificity, ↓ Sensitivity'),
bullet('Low cut-off → ↑ Sensitivity, ↓ Specificity'),
highlight("Wilson's 10 criteria for a good screening programme — know all 10"),
]
el.append(spacer())
el += [sub_heading('1.3 Measures of Disease Frequency ⭐'), spacer(2)]
el += [
bullet('Incidence Rate = New cases / Population at risk × Time'),
bullet('Prevalence = All existing cases / Total population (point in time)'),
bullet('Prevalence ≈ Incidence × Duration of disease'),
bullet('High incidence + short duration → Low prevalence (e.g., common cold)'),
bullet('Low incidence + long duration → High prevalence (e.g., diabetes, leprosy)'),
bullet('Attack Rate = Cases / Population exposed × 100 (used in outbreaks)'),
bullet('SAR = New household cases / Susceptible contacts × 100'),
]
el.append(spacer())
el += [sub_heading('1.4 Epidemic Investigation (9 Steps)'), spacer(2)]
for i, step in enumerate([
'Verify the diagnosis',
'Confirm it is an epidemic',
'Define a case (case definition)',
'Find cases systematically (active case search)',
'Tabulate by Person, Place, Time',
'Plot epidemic curve',
'Formulate hypothesis',
'Test hypothesis',
'Control and prevention measures',
], 1):
el.append(bullet(f'{i}. {step}'))
el.append(spacer(4))
el.append(data_table(
['Epidemic Type', 'Curve Shape', 'Classic Example'],
[
['Point source (common source)', 'Sharp rise & fall within 1 incubation period', 'Food poisoning'],
['Propagated (person-to-person)', 'Multiple waves, each = 1 incubation period apart', 'Measles in school'],
['Mixed', 'Common source then person-to-person', 'Cholera outbreak'],
],
col_widths=[5.5*cm, 7*cm, 5*cm]
))
el.append(PageBreak())
# ── UNIT 2: BIOSTATISTICS ─────────────────────────────────────────────────
el += [unit_heading('UNIT 2: BIOSTATISTICS'), spacer()]
el += [sub_heading('2.1 Measures of Central Tendency ⭐'), spacer(2)]
el.append(data_table(
['Measure', 'Definition', 'When to Use', 'Affected by Outliers?'],
[
['Mean', 'Sum / n', 'Normal distribution', 'Yes'],
['Median', 'Middle value', 'Skewed distribution', 'No'],
['Mode', 'Most frequent value', 'Nominal/qualitative data', 'No'],
],
col_widths=[3*cm, 4.5*cm, 5.5*cm, 4.5*cm]
))
el.append(spacer(4))
el += [
body('<b>Normal Distribution:</b> Mean = Median = Mode. Bell-shaped, symmetrical.'),
bullet('±1 SD → 68.27% of values'),
bullet('±2 SD → 95.45% of values'),
bullet('±3 SD → 99.73% of values'),
body('<b>Skewed distribution:</b>'),
bullet('Positive skew (right): Mean > Median > Mode'),
bullet('Negative skew (left): Mean < Median < Mode'),
]
el.append(spacer())
el += [sub_heading('2.2 Statistical Tests ⭐'), spacer(2)]
el.append(data_table(
['Test', 'Used When', 'Data Type'],
[
["Student's t-test", 'Compare 2 means (small samples)', 'Continuous'],
['Paired t-test', 'Before/after in same group', 'Continuous'],
['ANOVA (F-test)', 'Compare 3+ group means', 'Continuous'],
['Chi-square (χ²)', 'Compare proportions / test association', 'Categorical'],
['Correlation (r)', 'Relationship between 2 variables', 'Continuous'],
],
col_widths=[5*cm, 8*cm, 4.5*cm]
))
el.append(spacer(4))
el += [
highlight('p < 0.05 = statistically significant → reject null hypothesis'),
bullet('Type I error (α): Reject true null hypothesis (false positive) — α = 0.05'),
bullet('Type II error (β): Accept false null hypothesis (false negative)'),
bullet('Power = 1 – β (ability to detect a true difference)'),
bullet('95% CI not crossing 1 (for OR/RR) = statistically significant'),
]
el.append(spacer())
el += [sub_heading('2.3 Sampling Methods'), spacer(2)]
el.append(data_table(
['Method', 'Description'],
[
['Simple random', 'Each unit has equal probability of selection'],
['Systematic', 'Every kth unit; k = N/n'],
['Stratified', 'Divide into strata; random sample from each stratum'],
['Cluster', 'Natural groups selected; all units in selected clusters studied'],
['Multistage', 'Combination of above methods'],
],
col_widths=[4.5*cm, 13*cm]
))
el.append(spacer(3))
el.append(highlight('Cluster sampling (EPI 30×7) used for national immunisation coverage surveys in India'))
el.append(PageBreak())
# ── UNIT 3: DEMOGRAPHY ────────────────────────────────────────────────────
el += [unit_heading('UNIT 3: DEMOGRAPHY & VITAL STATISTICS'), spacer()]
el += [sub_heading('3.1 Key Vital Statistics Indicators ⭐'), spacer(2)]
el.append(data_table(
['Indicator', 'Denominator', 'Multiplier', 'India (NFHS-5)'],
[
['Crude Birth Rate (CBR)', 'Mid-year population', '1000', '~20'],
['Crude Death Rate (CDR)', 'Mid-year population', '1000', '~6'],
['Infant Mortality Rate (IMR)', 'Live births', '1000', '35.2'],
['Neonatal Mortality Rate (NMR)', 'Live births', '1000', '25.5'],
['Maternal Mortality Ratio (MMR)', 'Live births', '100,000', '97'],
['Total Fertility Rate (TFR)', '—', '—', '2.0'],
],
col_widths=[5.5*cm, 4.5*cm, 2.5*cm, 5*cm]
))
el.append(spacer(4))
el += [
highlight('IMR = most sensitive indicator of overall health status of a community'),
bullet('Replacement level TFR = 2.1 (population maintains itself)'),
bullet('MMR = maternal deaths per 100,000 live births (ratio, not rate)'),
]
el.append(spacer())
el += [sub_heading('3.2 Demographic Transition'), spacer(2)]
el.append(data_table(
['Stage', 'Birth Rate', 'Death Rate', 'Growth', 'Example'],
[
['I — High stationary', 'High', 'High', 'Stable/Low', 'Pre-industrial'],
['II — Early expanding', 'High', 'Falling', 'Rapid', 'India 1921–1951'],
['III — Late expanding', 'Falling', 'Low', 'Slowing', 'India currently'],
['IV — Low stationary', 'Low', 'Low', 'Stable/Low', 'Developed countries'],
['V — Declining', 'Low', 'Low', 'Negative', 'Some European nations'],
],
col_widths=[4*cm, 2.5*cm, 2.5*cm, 3*cm, 5.5*cm]
))
el.append(spacer(3))
el.append(highlight('1921 = "Year of Great Divide" — India\'s population began rapid increase'))
el.append(PageBreak())
# ── UNIT 4: ENVIRONMENT ───────────────────────────────────────────────────
el += [unit_heading('UNIT 4: ENVIRONMENT & HEALTH'), spacer()]
el += [sub_heading('4.1 Water — Standards & Purification ⭐'), spacer(2)]
el += [
bullet('WHO safe water: Coliform count = 0 per 100 mL'),
bullet('pH 7.0–8.5 | Turbidity <1 NTU | TDS <500 mg/L'),
]
el.append(spacer(3))
el.append(data_table(
['Fluoride Level', 'Effect'],
[
['< 0.5 mg/L', 'Dental caries'],
['0.5–0.8 mg/L (India optimal)', 'Beneficial — prevents caries'],
['> 1.5 mg/L', 'Dental fluorosis'],
['> 3.0 mg/L', 'Skeletal fluorosis'],
],
col_widths=[6*cm, 11.5*cm]
))
el.append(spacer(4))
el.append(body('<b>Purification steps (slow sand filter):</b>'))
for s in ['Storage/Sedimentation → removes 75–90% bacteria',
'Coagulation/Flocculation (Alum 5–40 mg/L)',
'Filtration — slow sand filter removes 98–99% bacteria',
'Disinfection (Chlorination)']:
el.append(bullet(s))
el.append(highlight('Residual chlorine = 0.5 mg/L after 1 hour contact = safe water'))
el.append(spacer())
el += [sub_heading('4.2 Air Pollution'), spacer(2)]
el.append(data_table(
['Pollutant', 'Source', 'Health Effect'],
[
['CO (carbon monoxide)', 'Incomplete combustion', 'Cherry-red appearance, COHb, death'],
['SO₂', 'Coal/oil combustion', 'Bronchospasm, acid rain'],
['NO₂', 'Traffic, industry', 'Pulmonary oedema (brown fumes)'],
['PM₂.₅', 'Vehicles, industry', 'Pneumoconiosis, lung cancer'],
['Ozone', 'Photochemical smog', 'Eye and lung irritation'],
],
col_widths=[4*cm, 5.5*cm, 8*cm]
))
el.append(spacer(4))
el += [
bullet('London smog (1952): SO₂ + fog + temperature inversion → 4000 deaths. Cold, reducing smog.'),
bullet('LA smog: Photochemical. Warm, oxidising. NO₂ + hydrocarbons + UV → ozone.'),
]
el.append(spacer())
el += [sub_heading('4.3 Hospital / Biomedical Waste'), spacer(2)]
el.append(data_table(
['Bag Colour', 'Waste Type', 'Disposal Method'],
[
['Yellow', 'Anatomical, pathological waste', 'Incineration'],
['Red', 'Contaminated recyclable waste', 'Autoclaving'],
['Blue/White (sharps)', 'Needles, blades', 'Shredding / encapsulation'],
['Black', 'General solid waste', 'Landfill'],
],
col_widths=[3.5*cm, 8*cm, 6*cm]
))
el.append(highlight('BMW Rules: Biomedical Waste Management & Handling Rules 1998 (amended 2016)'))
el.append(PageBreak())
# ── UNIT 5: NUTRITION ─────────────────────────────────────────────────────
el += [unit_heading('UNIT 5: NUTRITION'), spacer()]
el += [sub_heading('5.1 Protein-Energy Malnutrition (PEM) ⭐'), spacer(2)]
el.append(data_table(
['Feature', 'Kwashiorkor', 'Marasmus'],
[
['Cause', 'Protein deficiency (adequate calories)', 'Overall calorie deficiency'],
['Age', '1–5 years', '< 1 year'],
['Weight', 'Moderately reduced', 'Severely reduced (<60% expected)'],
['Oedema', 'PRESENT (pitting)', 'ABSENT'],
['Appearance', 'Moon face, pot belly, flaky paint dermatosis', '"Old man face", baggy pants'],
['Hair changes', 'Reddish/brown, flag sign, easily pluckable', 'Sparse'],
['Fatty liver', 'Present', 'Absent'],
['Serum albumin', 'Very low', 'Normal/slightly low'],
['Appetite', 'Poor', 'Good'],
],
col_widths=[4*cm, 6.75*cm, 6.75*cm]
))
el.append(spacer(3))
el += [
bullet('Gomez classification (wt for age): Grade I = 75–90% | Grade II = 60–74% | Grade III = <60%'),
bullet('Wellcome Trust: Based on weight + presence/absence of oedema'),
]
el.append(spacer())
el += [sub_heading('5.2 Vitamin Deficiency Diseases ⭐'), spacer(2)]
el.append(data_table(
['Vitamin', 'Disease', 'Key Clinical Features'],
[
['A (Retinol)', 'Xerophthalmia', 'Night blindness, Bitot\'s spots, keratomalacia'],
['B1 (Thiamine)', 'Beriberi', 'Dry (neuropathy), Wet (cardiomyopathy), Wernicke-Korsakoff'],
['B2 (Riboflavin)', 'Ariboflavinosis', 'Cheilosis, angular stomatitis, corneal vascularisation'],
['B3 (Niacin)', 'Pellagra', '4 D\'s: Dermatitis, Diarrhoea, Dementia, Death. Maize diet.'],
['C (Ascorbic acid)', 'Scurvy', 'Perifollicular haemorrhage, bleeding gums, corkscrew hairs'],
['D (Calciferol)', 'Rickets / Osteomalacia', 'Craniotabes, bow legs, Harrison\'s sulcus'],
['B12', 'Megaloblastic anaemia', 'Macrocytic anaemia, subacute combined degeneration of cord'],
],
col_widths=[3.5*cm, 4.5*cm, 9.5*cm]
))
el.append(spacer(3))
el.append(highlight('Pellagra = Niacin deficiency = Maize diet — "4 D\'s"'))
el.append(PageBreak())
# ── UNIT 6: MCH ───────────────────────────────────────────────────────────
el += [unit_heading('UNIT 6: MATERNAL & CHILD HEALTH'), spacer()]
el += [sub_heading('6.1 Antenatal Care Schedule ⭐'), spacer(2)]
el.append(data_table(
['Visit', 'Timing', 'Key Activities'],
[
['1st ANC', 'Within 12 weeks', 'Registration, history, first check-up, booking investigations'],
['2nd ANC', '14–26 weeks', 'Anomaly scan, IFA compliance check'],
['3rd ANC', '28–34 weeks', 'Presentation, BP, growth assessment'],
['4th ANC', '36 weeks to term', 'Birth preparedness, mode of delivery planning'],
],
col_widths=[2.5*cm, 4*cm, 11*cm]
))
el.append(spacer(4))
el += [
highlight('WHO now recommends minimum 8 ANC contacts (not just 4)'),
bullet('3 TT doses: TT-1 (early pregnancy), TT-2 (4 weeks later), TT-booster (if previously immunised)'),
bullet('IFA: 1 tablet daily from 12 weeks — 100 mg elemental iron + 500 mcg folic acid'),
]
el.append(spacer())
el += [sub_heading('6.2 Universal Immunisation Programme (UIP) ⭐'), spacer(2)]
el.append(data_table(
['Age', 'Vaccines'],
[
['Birth', 'BCG, OPV-0, Hep-B₁'],
['6 weeks', 'OPV-1, Penta-1 (DPT+HepB+Hib), IPV-1, Rota-1, fIPV-1'],
['10 weeks', 'OPV-2, Penta-2, Rota-2'],
['14 weeks', 'OPV-3, Penta-3, IPV-2, Rota-3, fIPV-2'],
['9 months', 'MR-1, JE-1 (endemic areas), Vit A dose 1'],
['16–24 months', 'MR-2, DPT booster-1, OPV booster, JE-2, Vit A-2'],
['5–6 years', 'DPT booster-2'],
['10 & 16 years', 'Td'],
],
col_widths=[4*cm, 13.5*cm]
))
el.append(spacer(4))
el += [
bullet('Cold chain: +2°C to +8°C (OPV: –20°C)'),
bullet('VVM: Inner square LIGHTER than outer circle = usable. DARKER = DISCARD'),
highlight('Herd immunity threshold: Measles = 95% | Polio = 82–87% | Smallpox = 85%'),
]
el.append(PageBreak())
# ── UNIT 7: NATIONAL PROGRAMS ─────────────────────────────────────────────
el += [unit_heading('UNIT 7: NATIONAL HEALTH PROGRAMS'), spacer()]
el += [sub_heading('7.1 Key Programs at a Glance ⭐'), spacer(2)]
el.append(data_table(
['Program', 'Year', 'Key Focus'],
[
['JSY (Janani Suraksha Yojana)', '2005', 'Cash incentive for institutional delivery (BPL)'],
['JSSK (Janani Shishu Suraksha)', '2011', 'Free delivery, free drugs/transport at public facilities'],
['PMSMA', '2016', 'Free ANC on 9th of every month'],
['SUMAN', '2019', 'Zero-denial, dignified maternity care'],
['NTEP (formerly RNTCP)', '2020', 'TB elimination by 2025; DOTS, Nikshay portal'],
['NVBDCP', '2003', 'Malaria, dengue, filaria, kala-azar, JE, chikungunya'],
['NACP', 'Phase I: 1992', 'HIV/AIDS — ART, ICTC, PPTCT'],
['NLEP', '1983', 'Leprosy MDT; elimination achieved 2005 (<1/10,000)'],
['NHM', '2013', 'ASHA, free drugs, JSY, JSSK under rural + urban missions'],
],
col_widths=[5.5*cm, 2.5*cm, 9.5*cm]
))
el.append(spacer())
el += [sub_heading('7.2 NTEP (National Tuberculosis Elimination Programme) ⭐'), spacer(2)]
el += [
bullet('Treatment regimen (new cases): 2(HRZE) / 4(HR) — Total 6 months'),
bullet('DOTS: Directly Observed Treatment Short-course'),
bullet('Nikshay portal: National TB case notification system'),
bullet('Nikshay Poshan Yojana: Rs. 500/month nutritional support to TB patients'),
highlight('India target: Eliminate TB by 2025 (SDG global target is 2030)'),
]
el.append(spacer(4))
el.append(data_table(
['Diagnostic Test', 'Details'],
[
['Sputum smear (ZN stain)', 'AFB positive/negative; rapid, cheap'],
['CBNAAT (Xpert MTB/RIF)', 'Rapid PCR-based; detects RIF resistance in 2 hours'],
['Culture (LJ medium)', 'Gold standard; 6–8 weeks turnaround'],
['TST (Mantoux)', 'Positive >10 mm induration in immunocompetent'],
],
col_widths=[5.5*cm, 12*cm]
))
el.append(spacer())
el += [sub_heading('7.3 Malaria — Short Notes ⭐'), spacer(2)]
el.append(data_table(
['Species', 'Type', 'Incubation', 'Fever Pattern'],
[
['P. vivax', 'Benign tertian', '14 days', 'Every 48 hrs'],
['P. falciparum', 'Malignant tertian', '12 days', 'Irregular / every 48 hrs'],
['P. malariae', 'Quartan', '28 days', 'Every 72 hrs'],
['P. ovale', 'Ovale tertian', '17 days', 'Every 48 hrs'],
],
col_widths=[3.5*cm, 3.5*cm, 3.5*cm, 7*cm]
))
el.append(spacer(4))
el += [
bullet('Vector: Anopheles (female), breeds in clear unpolluted water, bites at dusk/night'),
bullet('API = Confirmed malaria cases × 1000 / Population at risk'),
bullet('Treatment: P. vivax → Chloroquine + Primaquine (14 days) | P. falciparum → ACT + Primaquine (single dose)'),
highlight('DDT still used in India under NVBDCP for indoor residual spraying (IRS)'),
]
el.append(PageBreak())
# ── UNIT 8: HEALTH EDUCATION ──────────────────────────────────────────────
el += [unit_heading('UNIT 8: HEALTH EDUCATION & SOCIAL MEDICINE'), spacer()]
el += [sub_heading('8.1 Health Education Methods'), spacer(2)]
el.append(data_table(
['Level', 'Methods'],
[
['Individual', 'Counselling, interview, home visits, bedside teaching'],
['Group', 'Lectures, group discussions, role play, demonstrations, workshops'],
['Mass / Community', 'TV, radio, newspapers, posters, folk media, exhibitions'],
],
col_widths=[3.5*cm, 14*cm]
))
el.append(spacer(4))
el += [
bullet('IEC = Information, Education, Communication'),
bullet('BCC = Behaviour Change Communication (newer, more participatory approach)'),
bullet('KAPB Survey = Knowledge, Attitude, Practices, Behaviour — baseline assessment'),
]
el.append(spacer())
el += [sub_heading('8.2 Socioeconomic Status (SES) Scales ⭐'), spacer(2)]
el.append(data_table(
['Scale', 'Setting', 'Components'],
[
['B.G. Prasad', 'Urban + Rural', 'Per capita monthly income (5 classes)'],
['Kuppuswamy', 'Urban', 'Education + Occupation + Income'],
['Uday Pareek', 'Rural', 'Education, occupation, land, housing, standard of living, caste'],
],
col_widths=[4*cm, 3.5*cm, 10*cm]
))
el.append(spacer(3))
el.append(highlight('BG Prasad scale updated periodically using Consumer Price Index (CPI)'))
el.append(PageBreak())
# ── UNIT 9: OCCUPATIONAL HEALTH ───────────────────────────────────────────
el += [unit_heading('UNIT 9: OCCUPATIONAL HEALTH'), spacer()]
el += [sub_heading('9.1 Occupational Lung Diseases (Pneumoconioses) ⭐'), spacer(2)]
el.append(data_table(
['Disease', 'Causative Agent', 'Occupation'],
[
['Silicosis', 'Free silica (SiO₂)', 'Mining, stone cutting, glass industry'],
['Anthracosis', 'Coal dust', 'Coal mining'],
['Asbestosis', 'Asbestos fibres', 'Asbestos mining, lagging, shipbuilding'],
['Bagassosis', 'Bagasse (sugarcane waste)', 'Sugar industry'],
['Byssinosis', 'Cotton dust', 'Cotton textile workers'],
["Farmer's lung", 'Thermophilic actinomycetes (mouldy hay)', 'Farmers'],
['Siderosis', 'Iron oxide', 'Welders, iron miners'],
],
col_widths=[4*cm, 6.5*cm, 7*cm]
))
el.append(spacer(3))
el.append(highlight('Silicosis = most common occupational lung disease. No cure. Prevention = dust suppression + PPE.'))
el.append(spacer())
el += [sub_heading('9.2 Key Occupational Health Acts'), spacer(2)]
el += [
bullet('ESI (Employees State Insurance) Act, 1948: Medical, sickness, maternity, disablement benefits'),
bullet('Factories Act, 1948: Safety, health, welfare of factory workers'),
bullet('Workmens Compensation Act, 1923: Compensation for work-related injury/disease'),
bullet('ESIC covers workers earning ≤ Rs. 21,000/month'),
]
el.append(PageBreak())
# ── UNIT 10: NCDs ─────────────────────────────────────────────────────────
el += [unit_heading('UNIT 10: NON-COMMUNICABLE DISEASES'), spacer()]
el += [sub_heading('10.1 Hypertension — Epidemiology ⭐'), spacer(2)]
el.append(data_table(
['Category', 'Systolic (mmHg)', 'Diastolic (mmHg)'],
[
['Normal', '< 120', '< 80'],
['Pre-hypertension', '120–139', '80–89'],
['Stage 1 HTN', '140–159', '90–99'],
['Stage 2 HTN', '≥ 160', '≥ 100'],
],
col_widths=[5*cm, 6.25*cm, 6.25*cm]
))
el.append(spacer(4))
el += [
bullet('Risk factors: Age, male sex, obesity, sedentary lifestyle, high salt, smoking, alcohol, family history'),
highlight('Hypertension = most important modifiable risk factor for stroke'),
bullet('NPCDCS: Screening for DM + HTN + cancer at HWCs (Health and Wellness Centres)'),
]
el.append(spacer())
el += [sub_heading('10.2 Diabetes Mellitus — Diagnostic Criteria (ADA/WHO)'), spacer(2)]
el.append(data_table(
['Test', 'Diabetes', 'IFG / IGT (Pre-diabetes)'],
[
['Fasting plasma glucose', '≥ 126 mg/dL', 'IFG: 100–125 mg/dL'],
['2-hr OGTT', '≥ 200 mg/dL', 'IGT: 140–199 mg/dL'],
['Random plasma glucose + symptoms', '≥ 200 mg/dL', '—'],
['HbA1c', '≥ 6.5%', 'Pre-DM: 5.7–6.4%'],
],
col_widths=[5.5*cm, 5*cm, 7*cm]
))
el.append(PageBreak())
# ── QUICK REVISION TABLE ──────────────────────────────────────────────────
el += [unit_heading('QUICK REVISION: High-Yield Numbers & Facts'), spacer()]
el.append(data_table(
['Topic', 'Key Fact'],
[
['IMR formula', 'Deaths <1 year per 1000 live births'],
['MMR formula', 'Maternal deaths per 100,000 live births'],
['India IMR (NFHS-5)', '35.2 per 1000 live births'],
['India MMR (SRS 2020)', '97 per 100,000 live births'],
['India TFR (NFHS-5)', '2.0 (below replacement)'],
['Replacement TFR', '2.1'],
['Normal distribution ±1 SD', '68.27% of values'],
['Normal distribution ±2 SD', '95.45% of values'],
['Safe residual chlorine', '0.5 mg/L after 1 hour'],
['Optimal fluoride (India)', '0.5–0.8 mg/L'],
['WHO safe water coliform', '0 per 100 mL'],
['Sensitivity mnemonic', 'PID — Positive In Disease'],
['Specificity mnemonic', 'NIH — Negative In Health'],
['p < 0.05 means', 'Statistically significant'],
['Pellagra ↔ Diet', 'Maize diet / niacin deficiency'],
['Kwashiorkor vs Marasmus — oedema', 'Kwashiorkor = oedema PRESENT'],
['ASHA norm', '1 per 1000 population (1 per habitation in tribal/hilly areas)'],
['VVM discard when', 'Inner square DARKER than outer circle'],
['JSY launched', '12 April 2005'],
['JSSK launched', '1 June 2011'],
['PMSMA day', '9th of every month'],
['India TB elimination target', '2025 (5 years ahead of SDG)'],
['Malaria vector', 'Female Anopheles mosquito'],
['P. falciparum incubation', '12 days'],
['Measles herd immunity', '95%'],
['Chi-square used for', 'Comparison of proportions (categorical data)'],
['Attack Rate used in', 'Outbreak/epidemic investigation'],
['1921 = "Year of Great Divide"', "India's population began rapid increase"],
['Silicosis cause', 'Free silica (SiO₂) — most common occupational lung disease'],
['Pellagra 4 D\'s', 'Dermatitis, Diarrhoea, Dementia, Death'],
],
col_widths=[8.5*cm, 9*cm]
))
el.append(spacer(8))
el.append(callout(
'<b>Study Tip:</b> For RGUHS 3rd year theory, focus on: '
'(1) Epidemiology — study designs, screening, measures of disease frequency; '
'(2) National Health Programs — JSY, JSSK, PMSMA, NTEP, NVBDCP; '
'(3) Biostatistics — statistical tests, normal distribution, sampling; '
'(4) MCH — immunisation schedule, ANC components; '
'(5) Nutrition — PEM differences, vitamin deficiency diseases. '
'Source: Park\'s Textbook of Preventive & Social Medicine.',
bg=C_LIGHTBLUE
))
return el
# ── Page template ─────────────────────────────────────────────────────────────
def on_first_page(canvas, doc):
pass # no header/footer on cover
def on_later_pages(canvas, doc):
canvas.saveState()
canvas.setFont('Helvetica', 7.5)
canvas.setFillColor(C_DARKGREY)
canvas.drawString(2*cm, 1.2*cm,
'Community Medicine (PSM) | 3rd Year MBBS | RGUHS Short Notes Study Guide')
canvas.drawRightString(19.5*cm, 1.2*cm, f'Page {doc.page}')
canvas.setStrokeColor(C_TEAL)
canvas.setLineWidth(0.4)
canvas.line(2*cm, 1.5*cm, 19.5*cm, 1.5*cm)
canvas.restoreState()
# ── Build ─────────────────────────────────────────────────────────────────────
def build():
doc = SimpleDocTemplate(
OUTPUT,
pagesize=A4,
leftMargin=2*cm, rightMargin=2*cm,
topMargin=2*cm, bottomMargin=2*cm,
title='PSM Short Notes — RGUHS 3rd Year MBBS',
author='Orris AI Study Guide',
subject='Community Medicine — Preventive & Social Medicine',
)
story = cover_page() + content()
doc.build(story,
onFirstPage=on_first_page,
onLaterPages=on_later_pages)
print(f"PDF created: {OUTPUT}")
if __name__ == '__main__':
build()
cd /home/daytona/workspace/psm-study-guide && python3 generate_pdf.py 2>&1
ls -lh /home/daytona/workspace/psm-study-guide/PSM_ShortNotes_RGUHS_3rdYear.pdf
PSM ShortNotes RGUHS 3rdYear
PDF Document · PDF
| Unit | Content |
|---|---|
| 1 | Epidemiology — study designs, screening (sensitivity/specificity), disease frequency, epidemic investigation |
| 2 | Biostatistics — central tendency, statistical tests, sampling methods |
| 3 | Demography — vital statistics formulas, India NFHS-5 values, demographic transition |
| 4 | Environment — water standards, fluoride levels, air pollution, biomedical waste bags |
| 5 | Nutrition — PEM (Kwashiorkor vs Marasmus), vitamin deficiency diseases |
| 6 | MCH — ANC schedule, UIP immunisation chart, VVM, cold chain |
| 7 | National Programs — JSY/JSSK/PMSMA/SUMAN, NTEP, Malaria |
| 8 | Health Education — methods, SES scales (BG Prasad, Kuppuswamy) |
| 9 | Occupational Health — pneumoconioses, key acts |
| 10 | NCDs — HTN classification, DM diagnostic criteria |
| ⭐ | Quick revision table — 30 high-yield numbers & facts |
Search for RGUHS previous year PSM questions with explanations
RGUHS 3rd year community medicine PSM previous year question papers free download
RGUHS MBBS community medicine PSM solved question papers 2019 2020 2021 2022 2023
https://rrmch.org/cms/pdf/question-bank/UG-Community-Medicin…
https://www.slideshare.net/slideshow/question-bank-of-commun…
RGUHS Community Medicine (PSM) - Previous Year Questions with Explanations
Exam pattern (RS4 CBME scheme): 2 papers × 100 marks each | Long Essay (LAQ) = 10 marks each | Short Essay = 5 marks each | Short Answer = 3 marks each | MCQ = 1 mark each | Pass: 50% aggregate, min 40% per paper
PAPER I - FREQUENTLY REPEATED QUESTIONS
LAQ 1: Enumerate the indicators of health. Describe all mortality indicators with suitable examples. What are the methods of standardization of mortality rate? (RGUHS 2012 - 10 marks)
- Mortality indicators - CBR, CDR, IMR, MMR, etc.
- Morbidity indicators - Incidence rate, prevalence rate, notification rate
- Disability indicators - Days lost due to illness, DALY
- Nutritional indicators - weight/age, height/age, BMI
- Healthcare indicators - doctor:population ratio, hospital beds:population
- Socioeconomic indicators - literacy rate, per capita income, % below poverty line
- Health policy indicators - % GDP spent on health, % primary health care budget
| Indicator | Formula | Example |
|---|---|---|
| Crude Death Rate (CDR) | Deaths per 1000 mid-year population | India CDR ~6 |
| Infant Mortality Rate (IMR) | Deaths <1 year per 1000 live births | India 35.2 (NFHS-5) |
| Neonatal Mortality Rate | Deaths 0-28 days per 1000 live births | India 25.5 |
| Perinatal Mortality Rate | Stillbirths + deaths <7 days per 1000 births | Reflects obstetric care |
| Maternal Mortality Ratio | Maternal deaths per 100,000 live births | India 97 (SRS 2020) |
| Under-5 Mortality Rate | Deaths <5 years per 1000 live births | SDG target: <25 by 2030 |
| Proportional Mortality Rate | Deaths from a cause / Total deaths × 100 | TB = X% of total deaths |
- Direct standardization: Apply observed age-specific rates to a standard population
- Indirect standardization: Apply standard age-specific rates to the actual population → gives Standardized Mortality Ratio (SMR) = (Observed deaths / Expected deaths) × 100
- SMR > 100 = higher mortality than standard
- SMR < 100 = lower mortality than standard
LAQ 2: Describe screening for diseases — definition, types, uses, criteria for selection of disease and test (RGUHS 2012 - 10 marks)
- Mass screening: Entire population screened
- Selective/High-risk screening: Only at-risk groups (e.g., smokers for lung cancer)
- Multiphasic screening: Multiple tests applied at one time
- Opportunistic screening: When patient attends for another reason
- Early detection and treatment of disease
- Interrupting spread of communicable disease
- Identifying high-risk groups for intervention
- Research and epidemiological studies
- Important health problem (high prevalence/morbidity)
- Accepted treatment for patients
- Facilities for diagnosis and treatment available
- Recognisable latent or early symptomatic stage
- Suitable test or examination available
- Test acceptable to the population
- Natural history adequately understood
- Agreed policy on whom to treat
- Cost economically balanced in relation to healthcare expenditure
- Case-finding is a continuing process
| Disease + | Disease - | |
|---|---|---|
| Test + | a (TP) | b (FP) |
| Test - | c (FN) | d (TN) |
- Sensitivity = a/(a+c) × 100 → "PID" — detects true cases
- Specificity = d/(b+d) × 100 → "NIH" — correctly excludes healthy
- PPV = a/(a+b) × 100 → increases with higher disease prevalence
- NPV = d/(c+d) × 100 → high when disease prevalence is low
LAQ 3: What is Health Education? How will you organise a Health Education session on Anaemia for village women? (RGUHS 2012 - 10 marks)
- Women will list 3 iron-rich foods by end of session
- Women will demonstrate correct IFA tablet usage
- Definition and symptoms of anaemia (pallor, fatigue, breathlessness)
- Causes: iron deficiency, hookworm, malaria, poor diet
- Iron-rich foods: green leafy vegetables, jaggery, dates, meat, eggs
- Inhibitors of iron absorption: tea, coffee, phytates
- Enhancers: Vitamin C (citrus fruits, amla)
- IFA supplementation under national programs (weekly IFA for adolescent girls under WIFS scheme)
- When to seek care
- Group discussion at anganwadi centre (max 15 women)
- Flannel graph / flip charts showing iron-rich foods
- Food demonstration (cooking iron-rich recipes)
- Role play (ASHA demonstrating IFA tablet use)
- Immediate: KAP questions post-session
- Intermediate: Repeat Hb estimation at 3 months
- Long-term: Change in anaemia prevalence
LAQ 4: Carrier of infection — types, examples, control measures (RGUHS 2012 - 10 marks)
| Type | Definition | Example |
|---|---|---|
| Incubatory carrier | Infectious during incubation period (before symptoms) | Measles, hepatitis A |
| Convalescent carrier | Harbours organism after clinical recovery | Typhoid, cholera |
| Healthy/Contact carrier | Never had clinical disease | Meningococcal meningitis, diphtheria |
| Immune carrier | Has immunity but carries organism | Diphtheria (Schick negative) |
| Temporary carrier | Carrier state for days/weeks | Cholera |
| Chronic carrier | Carrier for months/years | Typhoid (Salmonella typhi in gallbladder), HBsAg+ |
- Detection: Stool cultures, serological tests, contact tracing
- Treatment: Appropriate antibiotics (e.g., ampicillin for typhoid carriers; cholecystectomy in biliary carriers)
- Notification: Report to health authorities
- Health education: Personal hygiene, hand washing
- Restriction: Carriers excluded from food-handling jobs (typhoid carriers)
- Follow-up: Repeated cultures to confirm clearance
PAPER II - FREQUENTLY REPEATED QUESTIONS
LAQ 5: Epidemiology, clinical features, prevention and control of Measles (RGUHS 2013 - 10 marks)
- Source: Cases (infected persons); no carrier state
- Mode of transmission: Droplet infection (most important), direct contact
- Incubation period: 10-14 days (average 12 days)
- Infectious period: 4 days before to 5 days after rash appears
- Herd immunity threshold: 95% (highly infectious, R₀ = 12-18)
- Seasonality: Winter-spring in temperate countries; no seasonal pattern in tropics
- Prodromal stage (3-4 days): Fever, cough, coryza, conjunctivitis
- Koplik's spots: Pathognomonic - small white spots on buccal mucosa (appear before rash)
- Rash: Maculopapular, starts at hairline/forehead, spreads downwards; fades in order of appearance; brownish discolouration (Pastia's lines)
- Vaccination: MR vaccine at 9 months (MR-1) and 16-24 months (MR-2) under UIP; 95% coverage needed for herd immunity
- Vitamin A supplementation: At time of vaccination reduces severity
- Case isolation: For 5 days after rash appearance
- Contact tracing and vaccination of susceptibles
- Measles elimination target: India aims to eliminate measles by 2023
LAQ 6: Causes of Maternal Mortality in India. Preventive and control measures for reduction of MMR (RGUHS 2013 - 10 marks)
- Haemorrhage (25%) - PPH most common (atonic uterus)
- Hypertensive disorders (eclampsia, pre-eclampsia) - 14%
- Sepsis/infection - 15%
- Unsafe abortion - 8% (India)
- Obstructed labour
- Anaemia (indirect cause - responsible for ~20% maternal deaths in India)
- ASHA mobilisation for ANC registration and institutional delivery
- Janani Suraksha Yojana (JSY) - cash incentive for institutional delivery
- JSSK - free delivery, drugs, transport
- PMSMA - free comprehensive ANC on 9th of every month
- SUMAN - zero-denial, respectful maternity care
- Minimum 4 ANC visits (WHO: 8 contacts)
- Early detection of high-risk pregnancies (anaemia, hypertension, malpresentation)
- Skilled birth attendance at every delivery
- Emergency Obstetric Care (EmOC) at FRUs
- Blood banks / storage centres at FRUs
- 24-hour delivery services at CHCs
- Maternal Death Review (MDR) - facility and community-based
- LaQshya programme - quality improvement in labour rooms
- Anaemia Mukt Bharat - IFA supplementation to prevent anaemia
FREQUENTLY REPEATED SHORT ESSAY QUESTIONS (5 marks each)
SE 1: Epidemiology and control of Malaria
- Causative agents: P. falciparum (malignant tertian, most dangerous), P. vivax, P. malariae (quartan), P. ovale
- Vector: Female Anopheles mosquito; breeds in clear, unpolluted water; bites dusk/night
- Incubation: P. vivax = 14 days | P. falciparum = 12 days | P. malariae = 28 days
- Indices: Spleen rate, parasite rate, API, ABER, SPR
- Treatment: P. vivax → Chloroquine + Primaquine (14d) | P. falciparum → ACT + Primaquine (single dose)
- Control: IRS (DDT/synthetic pyrethroids), LLINs, larval control, personal protection
SE 2: Validity of a screening test
SE 3: Demographic Cycle (Demographic Transition Theory)
SE 4: Pneumoconioses (write a short note)
- Silicosis (SiO₂) - most common
- Anthracosis (coal) | Asbestosis (asbestos) | Byssinosis (cotton) | Bagassosis (sugarcane) Prevention: Dust suppression, wet drilling, PPE, periodic medical exams, pre-employment and periodic X-rays
SE 5: Indicators of MCH care
- Maternal: MMR, % deliveries by skilled birth attendant, % with 4 ANC visits
- Child: IMR, NMR, PMR, under-5 MR
- Fertility: TFR, GFR, NRR
- Programme: % fully immunised, % institutional deliveries, JSSK coverage
SE 6: Investigation of food poisoning in a hostel (RGUHS 2009)
- Confirm diagnosis (clinical + lab)
- Define case and count cases
- Identify the food vehicle (food history, attack rates for each food item)
- Collect samples: stool, vomitus, suspected food, water
- Identify source and causative agent
- Control: Remove suspected food, treat cases, disinfect kitchen
- Preventive: Food handler training, proper food storage, cooking temperatures
SE 7: Principles of Primary Health Care (Alma Ata 1978)
- Community participation
- Appropriate technology
- Food/nutrition
- Education about health
- Water and sanitation
- Immunisation
- Control of endemic diseases
- Health care (MCH + family planning)
SE 8: Normal curve and Normal distribution
- Mean = Median = Mode
- ±1 SD = 68.27% | ±2 SD = 95.45% | ±3 SD = 99.73%
- Uses: Calculating reference ranges, statistical tests, z-scores
- Skewed = departure from normality (positively or negatively skewed)
WHERE TO FIND MORE RGUHS PYQs
| Source | What's Available | URL |
|---|---|---|
| RRMCH official question bank | RGUHS papers Jan 2008 – Dec 2013 (free PDF) | rrmch.org |
| RGUHS official site | RS4 model papers + curriculum | rguhs.ac.in |
| NRS Medical College | 2021-2022 papers with download links | nrsmc.edu.in |
| Slideshare question bank | Full topic-wise question bank for UGs + PGs | slideshare.net |
| TNMGRMU virtual library | Community Medicine Papers I & II, 2017-2026 | tnmgrmu.ac.in |
Pro tip: Ask me to write a full answer to any of these questions and I'll give you a structured, mark-specific response drawn from Park's Textbook - formatted exactly as needed for RGUHS theory papers.
Find recent 4 papers of rguhs and get answers from parks and prepare a pdf
RGUHS community medicine PSM question paper 2022 2023 2024 phase III part I PDF
RGUHS MBBS 3rd year community medicine paper 2021 2022 questions long essay short essay site:rguhs.ac.in OR site:rrmch.org OR site:nrsmc.edu.in
https://www.scribd.com/document/897813843/frdA021224A2239611…
Water sewage treatment plant
Sewage Treatment Plant
Definition of Sewage
- BOD (Biochemical Oxygen Demand): Amount of oxygen required by bacteria to stabilise decomposable organic matter aerobically. BOD ≥300 mg/L = "strong" sewage; 100 mg/L = "weak"
- COD (Chemical Oxygen Demand): Oxygen equivalent of organic matter oxidisable by a strong chemical oxidant
- Suspended Solids: 100 mg/L = weak sewage; 500 mg/L = strong sewage
Decomposition of Organic Matter in Sewage
| Process | Condition | End Products |
|---|---|---|
| Aerobic | Presence of free dissolved O₂ | CO₂, water, ammonia, nitrates, sulphates |
| Anaerobic | Absence of oxygen | Methane (CH₄), ammonia, CO₂, H₂ |
Modern Sewage Treatment Plant
SEWAGE INFLOW
│
▼
┌─────────────────────────────────┐
│ PRIMARY TREATMENT │ ← Removes SOLIDS (physical)
│ 1. Screening │
│ 2. Grit Chamber │
│ 3. Sedimentation Tank │
│ (Imhoff tank / septic tank) │
└─────────────────────────────────┘
│ Effluent
▼
┌─────────────────────────────────┐
│ SECONDARY TREATMENT │ ← Removes ORGANIC MATTER (biological)
│ 1. Trickling Filter │
│ 2. Activated Sludge Process │
└─────────────────────────────────┘
│ Treated Effluent
▼
DISPOSAL / REUSE
a. PRIMARY TREATMENT
1. Screening
- First step: sewage passed through a metal screen with vertical/inclined steel bars set 5 cm apart
- Removes large floating objects (wood, rags, garbage, dead animals)
- Prevents clogging of the treatment plant
- Screenings disposed of by trenching or burial
2. Grit Chamber (Detritus Chamber)
- Long narrow chamber, 10-20 metres in length
- Maintains constant velocity of ~1 foot/second, detention period 30 seconds to 1 minute
- Settles heavier inorganic solids: sand, gravel, broken glass, grit
- Allows lighter organic particles to pass through
- Grit removed and disposed of as fill material
3. Sedimentation (Primary Sedimentation Tank)
- Sewage passes into a large quiescent tank (detention time 1.5-2 hours)
- ~60-65% of suspended solids removed by gravity settling
- Settled material = raw sludge → goes to sludge digestion tank
- Floating material removed by skimmers
b. SECONDARY TREATMENT
1. Trickling Filter (Percolating / Biological Filter)
- A bed of coarse crushed stone or gravel (1.5-3 m deep) in a circular tank
- Sewage is sprayed over the surface through rotating sprinkler arms
- A gelatinous film (zoogloeal film) of aerobic bacteria, fungi, algae, and protozoa grows on the stones
- Organic matter in the effluent is oxidized as it trickles down through this film
- Produces a stable, odourless effluent (humus)
- Efficiency: removes 80-90% of BOD
2. Activated Sludge Process
- Sewage mixed with activated sludge (sludge rich in aerobic bacteria) in an aeration tank
- Air blown through the mixture for 4-8 hours → aerobic bacteria break down organic matter
- Mixture passes to secondary settling tank → sludge settles and most is returned to aeration tank (hence "activated") to seed new incoming sewage
- Excess sludge → sludge digestion tank → disposed as manure or dried
- Produces a very clean effluent with BOD reduction of 85-95%
c. OTHER METHODS OF SEWAGE DISPOSAL
(i) Sea Outfall
- Dilution of sewage in seawater — suitable only for coastal cities
- Self-purification by dilution, UV from sunlight, bactericidal action of seawater
- Must be discharged far enough from shore to prevent beach contamination
(ii) River Outfall
- Discharge into rivers; depends on self-purification capacity of the river
- Must satisfy the dilution factor and the oxygen sag curve criteria
- Not recommended unless river has very high dilution capacity
(iii) Sewage Farming (Land Application)
- Treated sewage used for irrigation of land (grows crops)
- Soil acts as a filter; organic matter fertilises the soil
- Only crops not eaten raw (fodder, fibre crops) should be grown on raw sewage farms
- Vegetables eaten raw must only use well-treated effluent
(iv) Oxidation Ponds (Stabilisation Ponds)
- Open, shallow ponds 1-1.5 m deep with inlet and outlet
- Requires three components: (1) algae + (2) bacteria + (3) sunlight
- Mutualistic cycle: Bacteria oxidize organic matter → produce CO₂ + minerals → algae use these with sunlight for photosynthesis → produce O₂ → bacteria use O₂ to oxidize more organic matter
- Predominantly aerobic during daylight hours; bottom layers anaerobic at night
- No odour nuisance when properly maintained
- Suitable for small communities
- Effluent can be used for land irrigation
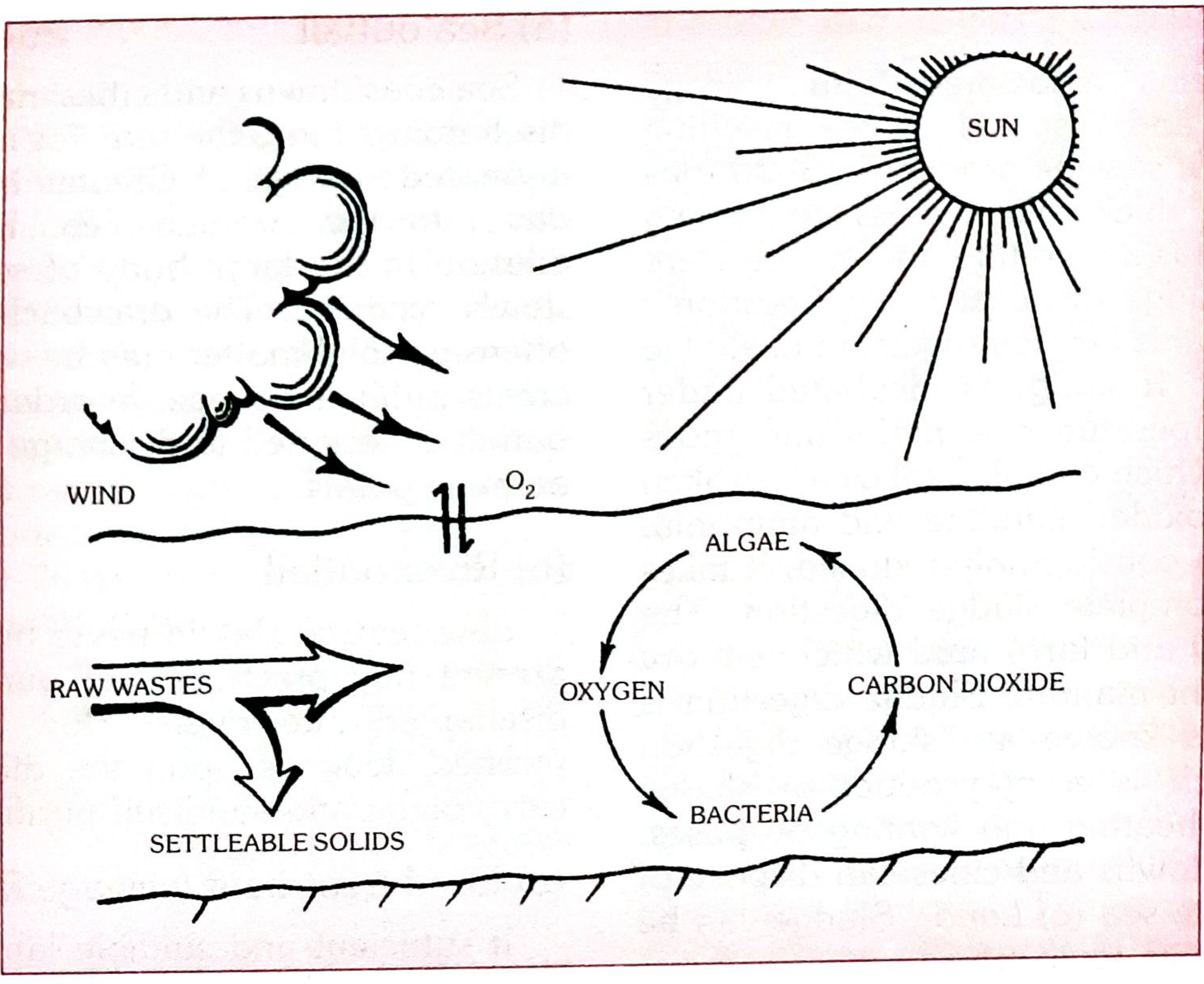
(v) Oxidation Ditches
- Use mechanical rotors for extended aeration
- For populations of 5,000-20,000
- Requires only 1 acre vs 22 acres for an oxidation pond
- Low-cost treatment method
Sludge Disposal
| Method | Details |
|---|---|
| Anaerobic digestion | Sludge digested in closed tank → produces biogas (methane) + stabilised sludge |
| Sludge drying beds | Digested sludge spread on sand beds → dried by sun and air |
| Manure / land application | Dried sludge used as agricultural fertiliser |
| Incineration | For heavily contaminated or toxic sludge |
Summary Comparison of Secondary Treatment Methods
| Feature | Trickling Filter | Activated Sludge |
|---|---|---|
| Process | Aerobic (fixed film) | Aerobic (suspended growth) |
| BOD removal | 80-90% | 85-95% |
| Land required | More | Less |
| Operation | Simple | Complex, skilled |
| Cost | Lower | Higher |
| Fly nuisance | Yes (filter flies) | No |
| Suitable for | Small/medium towns | Large cities |
Exam High-Yield Points ⭐
- BOD = primary indicator of sewage strength; normal sewage = 200-300 mg/L
- Primary treatment = physical removal of solids (screening → grit → sedimentation)
- Secondary treatment = biological oxidation of dissolved organic matter
- Imhoff tank = combined sedimentation + sludge digestion in one unit
- Trickling filter = zoogloeal film on stones; activated sludge = returned active bacteria
- Oxidation pond = algae-bacteria symbiosis + sunlight; suitable for small communities
- Sewage farming: only non-edible raw crops on raw sewage; treated effluent for vegetables
Modes of prevention flow chart
A detailed medical education flowchart titled "Modes of Prevention & Levels of Prevention" showing the natural history of disease (from left to right) mapped to prevention levels. The chart should show: Top row: Natural history stages: Pre-pathogenesis Phase (Susceptibility stage) → Pathogenesis Phase (Early disease → Advanced disease → Outcome: Recovery/Disability/Death) Below that, four rows showing prevention levels aligned to the natural history: 1. PRIMORDIAL PREVENTION (leftmost, before pre-pathogenesis): "Prevent emergence of risk factors" | Actions: Mass education, Healthy public policy, Healthy lifestyle promotion | Target: Total population 2. PRIMARY PREVENTION (pre-pathogenesis stage): Two sub-levels: - Health Promotion: Health education, Nutritional interventions, Environmental modification, Lifestyle changes, Housing improvement, Recreation, Social support - Specific Protection: Immunization, Chemoprophylaxis, Protection from occupational hazards, Use of seat belts, Fluoridation of water, Nutrition supplementation 3. SECONDARY PREVENTION (early disease stage): Early Diagnosis & Prompt Treatment: Screening tests, Case finding, Mass surveys, Selective exams | Goal: Reduce prevalence, shorten duration 4. TERTIARY PREVENTION (advanced disease/outcome stage): Two sub-levels: - Disability Limitation: Treatment to prevent complications, Adequate therapy, Prevent progression - Rehabilitation: Medical, Social, Vocational, Psychological rehabilitation | Goal: Restore function, return to society A horizontal arrow at the bottom shows the disease progression from left to right. Color code each level distinctly: green for primordial, blue for primary, orange for secondary, red for tertiary. Clean white background, clear labels, medical textbook style (Park's Textbook of Preventive and Social Medicine)
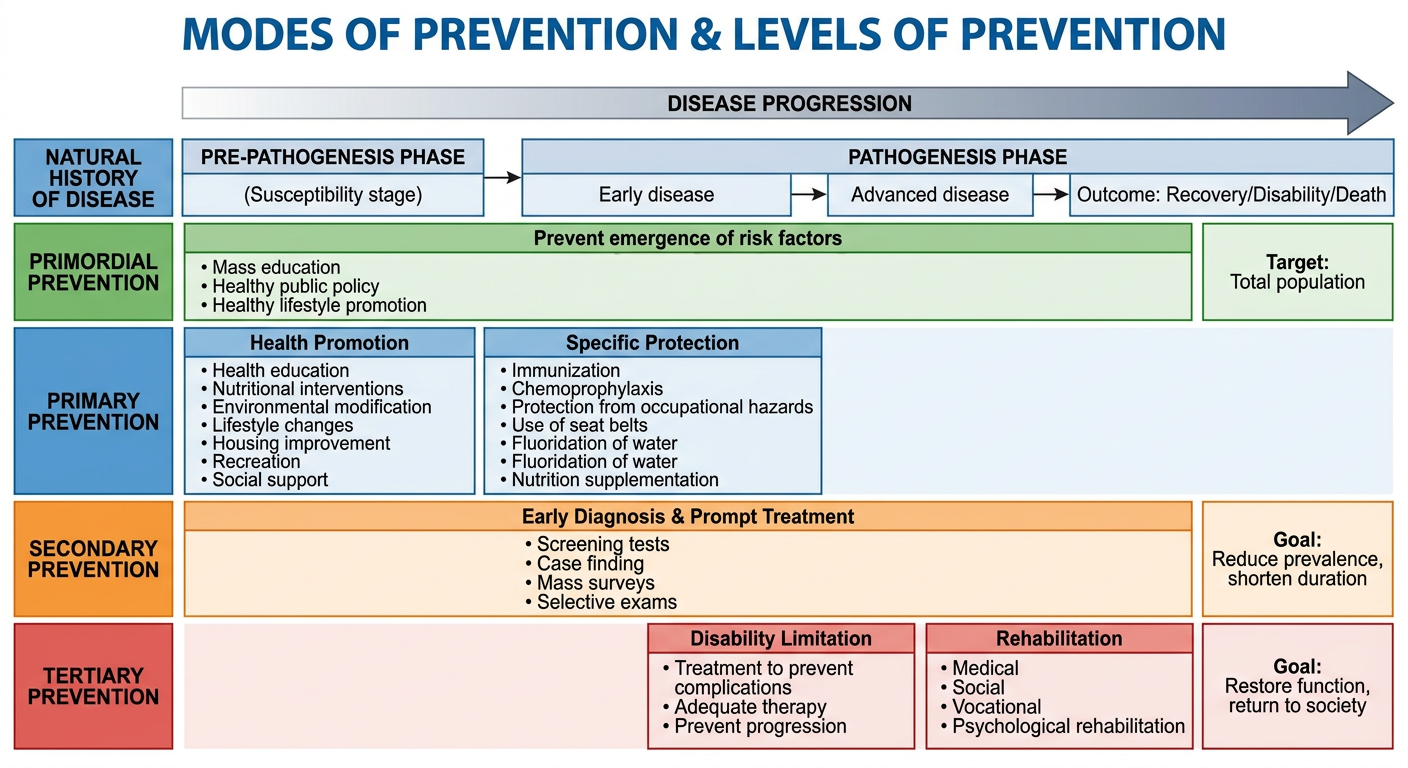
Levels & Modes of Prevention — Complete Notes
PRE-PATHOGENESIS ────────────── PATHOGENESIS PHASE ──────────────▶
(No disease yet) Early disease Advanced disease Outcome
NATURAL HISTORY OF DISEASE PHASES
| Phase | Stage | What's Happening |
|---|---|---|
| Pre-pathogenesis | Susceptibility | Agent, host, environment interact; no tissue change yet |
| Pathogenesis - Early | Sub-clinical / Presymptomatic | Tissue changes begun; disease detectable by screening |
| Pathogenesis - Advanced | Clinical disease | Signs and symptoms manifest |
| Outcome | Recovery / Disability / Death | End result of disease process |
LEVEL 1: PRIMORDIAL PREVENTION
- Mass/individual health education discouraging harmful lifestyles
- Healthy public policy (e.g., ban on tobacco advertising)
- Promoting healthy lifestyle habits in children before risk factors develop
- Socioeconomic development, food security
LEVEL 2: PRIMARY PREVENTION
(A) Health Promotion
- Health education
- Nutritional interventions (food distribution, supplementation, fortification)
- Environmental modifications (safe water, sanitation, housing, vector control)
- Lifestyle and behavioural changes
(B) Specific Protection
- Immunization (vaccines — most powerful specific protection)
- Chemoprophylaxis (e.g., anti-malarials, INH for TB contacts)
- Protection from occupational hazards (PPE, dust control)
- Use of seatbelts / crash helmets
- Fluoridation of water (dental caries prevention)
- Protection from carcinogens
- Elimination of environmental risks
LEVEL 3: SECONDARY PREVENTION
(A) Early Diagnosis
- Mass screening programmes (e.g., cervical cancer, hypertension)
- Periodic health check-ups
- Selective examinations of high-risk groups
- Case-finding (active search for cases)
- Self-examination (e.g., breast self-examination)
(B) Prompt Treatment
- Adequate treatment to cure disease / arrest progression
- Prevent complications
- Prevent spread to others (reverse communicability)
- Prevent sequelae
LEVEL 4: TERTIARY PREVENTION
(A) Disability Limitation
- Treatment of established disease to prevent further deterioration
- Prevent progression to complete disability
- Adequate therapy at clinical level
- Example: Treatment of diabetic retinopathy to prevent blindness
(B) Rehabilitation
| Type | Goal |
|---|---|
| Medical rehabilitation | Restore physical function (physiotherapy, surgery) |
| Social rehabilitation | Restore family and social relationships |
| Vocational rehabilitation | Retrain for suitable employment |
| Psychological rehabilitation | Restore dignity, confidence, mental health |
Summary Table (Park's Table 10)
| Level | Phase | Aim | Key Actions | Target |
|---|---|---|---|---|
| Primordial | Underlying socioeconomic conditions | Prevent risk factors from appearing | Public health policy, health promotion, mass education | Total population |
| Primary | Specific causal factors (pre-disease) | Reduce incidence | Immunization, health education, environmental modification, specific protection | Population + high-risk individuals |
| Secondary | Early disease | Reduce prevalence (shorten duration) | Screening, case-finding, early treatment | Individuals with early/undetected disease |
| Tertiary | Late disease + disability | Reduce complications + restore function | Disability limitation, rehabilitation | Patients with established disability |
Key Exam Points ⭐
- Primordial = newest concept; specific to NCDs and chronic diseases; prevents risk factors (not disease itself)
- Primary = prevents incidence; operates in pre-pathogenesis
- Secondary = reduces prevalence; operates in early pathogenesis; key tool = screening
- Tertiary = reduces disability; operates in late pathogenesis/outcome
- Rehabilitation = part of tertiary prevention, not separate from it
- Health promotion and specific protection are the two sub-modes of primary prevention

Answer these questions
RGUHS Community Medicine Paper I — 22 May 2023 (Q.P. Code 1035)
LONG ESSAYS (10 marks each)
Q1. A 38-year-old man — stone quarry worker — dyspnoea — "snow-storm" X-ray appearance. Describe epidemiology, preventive and control measures.
Definition
Epidemiology
| Factor | Details |
|---|---|
| Agent | Free silica / crystalline quartz (SiO₂) dust particles <5 microns |
| Host | Male workers aged 30-60 years; longer exposure = greater risk |
| Occupations at risk | Stone quarry workers, miners (coal, gold, iron), sandblasters, foundry workers, pottery/ceramic workers, tunnel workers |
| Duration | Typically 10-20 years of exposure before symptoms |
| Incubation | Chronic silicosis: >10 years; Accelerated: 5-10 yrs; Acute: <5 yrs (massive exposure) |
| India | Rajasthan, Madhya Pradesh (stone quarries, slate pencil industry) most affected |
Pathology
- Silica particles phagocytosed by macrophages → macrophage death → release of fibrogenic factors → nodular fibrosis
- Progressive massive fibrosis (PMF) in advanced disease
- X-ray: Multiple small nodular opacities (snow-storm pattern) in both lung fields; "eggshell calcification" of hilar lymph nodes
Clinical Features
- Progressive dyspnoea (insidious onset, worsens over years)
- Dry cough, chest tightness
- Silico-tuberculosis: silicosis greatly increases TB risk (3x)
- Cor pulmonale in advanced cases
Preventive & Control Measures
- Substitution: Replace silica with safer abrasives (steel grit, glass beads)
- Wet drilling / wet methods: Suppression of dust by water sprays at point of dust generation
- Enclosure and isolation: Enclose dusty processes; isolate workers
- Local exhaust ventilation (LEV): Exhaust systems to capture dust at source
- General dilution ventilation: Fresh air circulation in enclosed mines
- Respirators/dust masks (NIOSH-approved)
- Regular replacement of filter elements
- Pre-employment medical examination + chest X-ray
- Periodic medical examination (every 6-12 months)
- Lung function tests (spirometry)
- Early removal from exposure if disease detected
- Mines Act 1952; Factories Act 1948
- Workmen's Compensation Act
- Dust exposure limits: Threshold Limit Value (TLV) for silica dust
- Workers educated on hazards, use of PPE, importance of periodic check-ups
- No specific cure; treatment of complications
- Anti-TB drugs if silico-TB develops
- Bronchodilators for symptom relief
- Whole-lung lavage in selected cases
Q2. Define epidemiology. Classify epidemiological study designs. Describe steps in conducting a case-control study using smoking and lung cancer as an example.
Definition of Epidemiology
Classification of Epidemiological Study Designs
EPIDEMIOLOGICAL STUDIES
│
├── OBSERVATIONAL (no intervention by investigator)
│ │
│ ├── Descriptive
│ │ ├── Case reports / Case series
│ │ └── Cross-sectional (prevalence study)
│ │
│ └── Analytical
│ ├── Case-Control (retrospective)
│ └── Cohort (prospective / retrospective)
│
└── EXPERIMENTAL (investigator intervenes)
├── Randomized Controlled Trial (RCT)
├── Field trial
└── Community trial
Case-Control Study — Steps (Smoking & Lung Cancer)
| Step | Details |
|---|---|
| 1. Define the problem | "Is smoking associated with lung cancer?" |
| 2. Select CASES | Newly diagnosed histologically confirmed lung cancer patients from hospitals. Include only incident (new) cases. |
| 3. Select CONTROLS | People without lung cancer from same hospital (other diagnoses) or community. Must be similar in age, sex, socioeconomic status. |
| 4. Matching | Match cases and controls for age (±5 yrs), sex, hospital to control confounding |
| 5. Measure exposure | Interview both groups: detailed smoking history (duration, quantity, type), past occupational exposure, diet — using standardized questionnaire |
| 6. Blinding | Interviewer should be blind to case/control status to avoid interviewer bias |
| 7. Calculate OR | Odds Ratio (OR) = ad/bc using 2×2 table |
| 8. Statistical analysis | Chi-square test; 95% confidence interval around OR |
| 9. Interpret | OR >1 = association; assess dose-response relationship |
| 10. Conclusion | Doll & Hill (1950) — classic case-control study confirming smoking-lung cancer link. OR ≈ 9-14 for heavy smokers |
| Lung Cancer (Cases) | No Cancer (Controls) | |
|---|---|---|
| Smoker | a | b |
| Non-smoker | c | d |
SHORT ESSAYS (8 marks each)
Q3. Different types of disinfection with suitable examples
Types of Disinfection
| Type | Definition | Example |
|---|---|---|
| Concurrent (Immediate) | Applied as soon as infectious material is discharged from the body; agent destroyed as it is released | Disinfection of sputum, faeces, vomit, contaminated linen during illness; handwashing after patient contact |
| Terminal | Applied after the patient has recovered, died, or been transferred; final cleaning of the room/environment | Cleaning and disinfection of ward after TB patient is discharged; fumigation of isolation room |
| Precurrent (Prophylactic) | Routine disinfection before potential contamination occurs | Chlorination of drinking water, pasteurization of milk, handwashing before procedures |
| Agent | Example |
|---|---|
| Natural agents | Sunlight (UV rays kill bacteria in linen), air/drying |
| Physical agents | Heat (boiling, autoclaving, hot air oven), burning/incineration |
| Chemical agents | Chlorine compounds (bleaching powder), phenol, formaldehyde, glutaraldehyde, alcohol (70%), iodine |
Q4. Define an epidemic. Classify epidemics with suitable examples.
Classification of Epidemics
| Type | Mechanism | Example |
|---|---|---|
| Common source | All cases from same source of exposure | Cholera from contaminated water supply |
| Propagated (serial) | Person-to-person spread; epidemic curve rises slowly with multiple peaks | Measles, influenza |
| Mixed | Starts as common source, then propagated spread | Cholera starting from water → person-to-person |
| Type | Feature | Example |
|---|---|---|
| Point source | All exposed at same time/place; sharp single peak in epidemic curve; incubation period = time from peak to end | Food poisoning at a wedding feast |
| Continuous source | Prolonged exposure from same source; plateau pattern | Contaminated well used over weeks |
| Intermittent source | Repeated exposure at intervals; multiple small peaks | Contaminated water supply with intermittent failures |
- Explosive epidemic: Sudden rise, all cases within one incubation period (e.g., food poisoning, chemical poisoning)
- Slow/gradual epidemic: Rises over weeks/months (e.g., AIDS, hepatitis B)
Q5. Define overcrowding. Role in impact on health and disease.
Health Effects of Overcrowding
| Category | Effect |
|---|---|
| Respiratory infections | TB, influenza, meningococcal disease — droplet spread facilitated by close proximity |
| Communicable diseases | Scabies, tinea (skin-to-skin contact); typhus (louse-borne); plague (rat-borne) |
| Mental health | Psychological stress, aggression, sleep deprivation, anxiety |
| Child health | Increased infant mortality, malnutrition, stunting |
| Domestic accidents | Burns, falls — more common in overcrowded homes |
| Sanitation | Shared toilets → faeco-oral disease transmission (cholera, typhoid, dysentery) |
| Nutrition | Inadequate food due to poverty associated with overcrowding |
| Social effects | Juvenile delinquency, domestic violence, sexual abuse |
Q6. Describe incineration of biomedical waste.
Types of Incinerators
| Type | Features |
|---|---|
| Single-chamber incinerator | Simple, basic; inadequate for complete combustion |
| Double-chamber (pyrolytic) incinerator | Primary + secondary chambers; most commonly recommended for hospitals |
| Rotary kiln | Large-scale; handles all waste types; temperature 900-1200°C |
Process (Double-chamber):
- Primary chamber (800-900°C): Waste is combusted in limited oxygen → pyrolytic decomposition
- Secondary chamber (900-1200°C): Gases from primary chamber fully oxidized → destroys toxic organic compounds, dioxins
- Flue gas treatment: Scrubbers, filters to remove pollutants before discharge
- Residual ash: Sent to secured landfill
Biomedical Waste Categories Suitable for Incineration (BMW Rules 2016):
- Yellow bag: Anatomical waste, soiled dressings, pathological waste
- Red bag: Contaminated recyclable waste (if non-recyclable)
- NOT suitable: Radioactive waste, cytotoxic waste, pressurised containers
Advantages
- 90-95% volume reduction
- Complete pathogen destruction
- Can generate energy (waste-to-energy)
Disadvantages
- Releases dioxins, furans, heavy metals if not properly operated
- High installation and running costs
- Requires trained operators
- Air pollution if inadequate flue gas treatment
Q7. Describe the natural history of disease with suitable examples.
Phases of Natural History
- No disease yet; interaction of agent, host, and environment
- Risk factors present (e.g., smoking, obesity, hypertension)
- Stimulus for disease not yet active in host
- Example (TB): M. tuberculosis in environment + susceptible host; exposure not yet occurred
| Sub-stage | Description | Example (TB) |
|---|---|---|
| Early pathogenesis | Agent enters host; no symptoms; detectable by screening (sub-clinical) | Tuberculin test positive; primary complex on X-ray |
| Advanced disease | Clinical signs and symptoms appear | Fever, cough, haemoptysis, weight loss |
| Outcome | Recovery / Disability / Death | Cure with treatment; cavitation → disability; death if untreated |
Key Concepts
- Iceberg phenomenon: Only tip visible (clinical cases); submerged base = sub-clinical/inapparent cases. Most infections show this (polio, TB, hepatitis)
- Spectrum of disease: From inapparent → mild → moderate → severe → fatal
- Herd immunity: Related to the proportion of population susceptible
- Prepathogenesis = point for primary prevention; early pathogenesis = secondary prevention
- Pre-pathogenesis: Smoking, obesity, hypertension, hyperlipidaemia present
- Early pathogenesis: Atherosclerosis developing; stress ECG abnormal
- Advanced: Angina, MI symptoms
- Outcome: Recovery with thrombolytics / permanent cardiac damage / death
Q8. Enumerate nutritional assessment methods. Describe any one in detail.
Methods of Nutritional Assessment (ABCD)
| Category | Methods |
|---|---|
| A — Anthropometric | Weight, height, BMI, MUAC, skinfold thickness, head/chest circumference, weight-for-age, height-for-age, weight-for-height |
| B — Biochemical | Serum albumin, haemoglobin, serum iron, ferritin, serum retinol (Vit A), urinary iodine, serum zinc |
| C — Clinical | Physical examination for signs of deficiency (pallor, Bitot's spots, goitre, oedema, wasting) |
| D — Dietary | 24-hour dietary recall, food frequency questionnaire, diet history, food balance sheets, duplicate meal method |
Anthropometric Assessment in Detail
| Grade | % of median (NCHS) | Classification |
|---|---|---|
| Normal | >90% | Normal |
| Grade I | 75-90% | Mild PEM |
| Grade II | 60-74% | Moderate PEM |
| Grade III | <60% | Severe PEM |
- Stunting = chronic malnutrition (<95% of median height-for-age)
- Wasting = acute malnutrition (<90% of median weight-for-height)
- <18.5 = Underweight; 18.5-24.9 = Normal; ≥25 = Overweight; ≥30 = Obese
- <12.5 cm = Severe acute malnutrition (SAM) in children 6-59 months
- 12.5-13.5 cm = Moderate acute malnutrition (MAM)
Q9. Describe the process of communication. Enumerate communication barriers.
Process of Communication (Berlo's SMCR Model)
SOURCE → MESSAGE → CHANNEL → RECEIVER → FEEDBACK
│ │ │ │
Encoder Content Medium Decoder
- Source (Communicator): Health worker, doctor, teacher with knowledge, attitude, communication skills
- Message: The health information encoded into words, symbols, or images; must be clear, accurate, relevant, simple
- Channel: Medium of transmission — interpersonal (face-to-face), mass media (TV, radio), print (posters, leaflets), electronic
- Receiver (Audience): Must decode and understand the message; influenced by education, culture, beliefs
- Feedback: Response from receiver back to source — confirms understanding; allows correction
Types of Communication
- Interpersonal: One-to-one counselling (most effective for behaviour change)
- Group communication: Health talks, demonstrations
- Mass communication: Radio, TV, newspapers (reaches many but less personal)
Communication Barriers
| Type | Examples |
|---|---|
| Physical barriers | Distance, noise, poor lighting, crowded environment |
| Psychological barriers | Fear, anxiety, lack of trust, mental preoccupation, prejudice |
| Semantic barriers | Use of technical/medical jargon, language differences, ambiguous words |
| Cultural barriers | Taboos, customs, beliefs that conflict with health messages |
| Educational barriers | Illiteracy, low health literacy — cannot read printed materials |
| Perceptual barriers | Selective perception — people hear what they want to hear |
| Organisational barriers | Hierarchical differences between health worker and patient |
| Socio-economic barriers | Poverty, social status differences |
Q10. Identify the causes and solutions for population explosion in India.
Causes
| Category | Cause |
|---|---|
| High birth rate | TFR 2.0 (still above replacement in several states); son preference; early marriage; desire for large families |
| Declining death rate | Medical advances, vaccines, sanitation improvements → infant/child mortality fall without corresponding fall in births |
| Low age at marriage | Child marriages (despite legal age 18F/21M) → longer reproductive period |
| Illiteracy | Especially female illiteracy → poor use of contraception, low women's autonomy |
| Poverty | Children seen as economic assets / old-age security |
| Religious/cultural factors | Opposition to family planning in some communities |
| Low contraceptive use | Unmet need for family planning still 9.4% (NFHS-5) |
| Low status of women | Lack of decision-making power over reproduction |
Solutions
| Category | Measure |
|---|---|
| Family planning services | Free contraceptives at PHC/SC; basket of choices (condoms, OCP, IUCD, sterilization); Mission Parivar Vikas for high-fertility districts |
| Female education | Beti Bachao Beti Padhao; Kasturba Gandhi Schools; educated women = lower TFR (1.6 vs 3.4) |
| Late marriage | Strict enforcement of PCPNDT Act; legal minimum marriage age |
| Male participation | Promote NSV (no-scalpel vasectomy); male condom promotion |
| Incentives/disincentives | Cash incentives for small family norm; two-child norm |
| Poverty alleviation | MGNREGS, social security → reduce demand for children |
| Media & IEC | Small family norm promotion through mass media |
| Status of women | SHGs, economic empowerment, political participation |
SHORT ANSWERS (3 marks each)
Q11. List three aims of epidemiology
- To describe the distribution and magnitude of health and disease problems in the community (who, when, where)
- To identify the determinants (causes and risk factors) of disease in order to explain its distribution
- To provide data for planning, implementing, and evaluating public health interventions for prevention and control of disease
Q12. Draw a pie chart with a suitable example
| Cause | % |
|---|---|
| Preterm birth complications | 35% |
| Birth asphyxia | 25% |
| Neonatal sepsis | 15% |
| Pneumonia | 10% |
| Diarrhoea | 8% |
| Other | 7% |
Preterm (35%)
___________
/ * \
| 35% PIE | ← Draw circle; divide by proportional sectors
| CHART | Each sector angle = (% × 360°) / 100
\___________/
Preterm: 126° | Asphyxia: 90° | Sepsis: 54°
Pneumonia: 36° | Diarrhoea: 29° | Other: 25°
- Draw a circle; divide into sectors proportional to angle (% × 3.6°)
- Label each sector with name and percentage
- Title: "Causes of Infant Mortality in India"
- Used for: Displaying parts of a whole; best when categories are 3-7
Q13. Enumerate the dimensions of health
- Physical dimension — Biological soundness; organs functioning normally
- Mental dimension — Ability to think clearly, manage emotions, cope with stress
- Social dimension — Ability to make and maintain relationships; social functioning
- Spiritual dimension — Sense of purpose, meaning, inner peace, moral values
- Emotional dimension — Ability to express and control emotions appropriately
- Vocational dimension — Ability to perform productive work/occupation
Q14. Methods for prevention and control of noise pollution
| Method | Examples |
|---|---|
| Source control (Engineering) | Machinery silencers, vibration dampeners, low-noise technology, proper maintenance |
| Path control | Sound barriers/walls along highways, insulating materials in walls/floors, distance between source and receiver |
| Receiver protection | Ear muffs/ear plugs (PPE) for workers; audiometric testing |
| Legislative | Noise Pollution (Regulation and Control) Rules 2000 (India); permissible limits: 90 dB for industrial, 45 dB residential (day) |
| Land use planning | Buffer zones between industrial and residential areas; airports away from cities |
| Traffic management | Speed limits, honking bans in silence zones (hospitals, schools) |
| Green belts | Planting trees to absorb sound between roads and buildings |
Q15. Common nutritional disorders in India
| Disorder | Cause | Affected Group |
|---|---|---|
| PEM (Protein-Energy Malnutrition) | Inadequate calories + protein; kwashiorkor / marasmus | Children under-5 |
| Iron deficiency anaemia | Inadequate dietary iron; most common nutritional deficiency in India | Women of reproductive age, children |
| Vitamin A deficiency | Low dietary intake; Bitot's spots → night blindness → xerophthalmia | Under-5 children |
| Iodine deficiency disorders (IDD) | Low iodine; goitre, cretinism | Himalayan, sub-Himalayan belts |
| Vitamin D deficiency (rickets) | Low sunlight exposure + low dietary calcium | Infants, children |
| Vitamin B12 / Folate deficiency | Megaloblastic anaemia; vegetarian diets | All age groups |
| Zinc deficiency | Growth retardation, impaired immunity | Children |
| Fluorosis | Excess fluoride in groundwater (dental + skeletal) | Endemic fluoride belt (Rajasthan, AP, Punjab) |
Q16. Define herd immunity with an example
| Disease | R₀ | HIT needed |
|---|---|---|
| Measles | 12-18 | 92-95% |
| Polio | 5-7 | 80-86% |
| Smallpox | 5-7 | 80-85% |
| COVID-19 | 2-3 | 50-67% |
Q17. Enumerate the contents of health education
- Nutrition and food hygiene — balanced diet, safe food preparation, breastfeeding
- Personal hygiene — handwashing, oral hygiene, skin care, menstrual hygiene
- Environmental sanitation — safe water, latrine use, garbage disposal, vector control
- Maternal and child health — ANC, immunization, family planning, birth spacing
- Communicable disease prevention — TB, malaria, HIV/AIDS, STIs
- Non-communicable disease prevention — no tobacco, physical activity, healthy diet
- First aid and home remedies — ORS for diarrhoea, wound care, emergency response
- Use of health services — when to visit PHC, immunization schedule, screening
- Family planning — methods, benefits of small family, responsible parenthood
- Occupational health — hazards, PPE use, safe working practices
Q18. How do you manage microbiology laboratory waste?
| Waste Type | Colour Code | Treatment |
|---|---|---|
| Microbiological/infectious cultures, stocks | Yellow bag | Autoclaving/incineration |
| Contaminated sharps (needles, syringes) | White/translucent puncture-proof container | Autoclave → shredding |
| Solid plastic waste (tubes, petri dishes) | Red bag | Autoclaving → recycling |
| Chemical waste (reagents, solvents) | Black bag | Chemical treatment / secured landfill |
| Liquid waste (culture media, body fluids) | Drain after disinfection with 1% hypochlorite (30 min contact) |
- Segregation at point of generation (colour-coded containers)
- Disinfection: Autoclaving (121°C, 15 psi, 30 min) for all microbiology waste
- Sharps safety: Needle-stick prevention, needle destroyers, puncture-proof containers
- Labelling: Biohazard symbol on all containers
- Transport: Leak-proof, sealed bags to treatment area
- Final disposal: Incineration or CBWTF (Common Biomedical Waste Treatment Facility)
- Record keeping: Log of waste quantity, treatment method, disposal site
Q19. List the functions of the World Health Organization (WHO)
- Normative/standard-setting: Establishes international health standards, guidelines, and nomenclature (ICD codes, drug standards, TLVs)
- Epidemiological surveillance: Global disease monitoring; International Health Regulations (IHR 2005); alerts for outbreaks (e.g., COVID-19, Ebola)
- Research coordination: Promotes and coordinates biomedical and health research globally
- Technical assistance: Provides technical support to member countries for health systems strengthening
- Health promotion: Campaigns (World No Tobacco Day, World Health Day, vaccination weeks)
- Emergency response: Humanitarian health aid in disasters, conflicts, epidemics (WHO GOARN)
- Training: Human resources development; fellowships; capacity building
- Maternal & child health: Policies for immunization, nutrition, reproductive health
- Eradication programmes: Smallpox (eradicated 1980); polio eradication; NTD programmes
- Publication: Weekly Epidemiological Record; World Health Statistics; global health reports
Q20. Sathya and Jyothi — married 2 years — Reproductive health services at PHC
| Service | Details |
|---|---|
| Family planning counselling | Basket of contraceptive choices, spacing methods |
| Contraceptive services | Free supply of condoms, oral contraceptive pills (OCPs), emergency contraception |
| IUCD insertion | Copper-T insertion by trained ANM/MO |
| Antenatal care (ANC) | 4 antenatal visits; TT injection; IFA tablets; BP, Hb monitoring; USS referral |
| Safe delivery | Normal deliveries conducted by trained staff; JSY benefits |
| Postnatal care (PNC) | Visits at 48 hours, 7 days, 42 days for mother and newborn |
| Immunization | Full immunization for children; TT for pregnant women |
| Nutritional supplementation | IFA (Iron-Folic Acid), Vitamin D, calcium tablets in pregnancy |
| STI/RTI diagnosis & treatment | Syndromic management of STIs; partner notification |
| PMSMA services | Free ANC on 9th of every month |
| Screening | Anaemia, hypertension, gestational diabetes, cervical cancer (VIA) |
| JSSK entitlements | Free drugs, diagnostics, diet, transport for delivery |
| Referral | Complicated cases referred to CHC/DH with JSSK transport |
| ASHA support | Accompanies women; registers pregnancies; provides counselling |