Asbestosis full details for md exams 15marks answer
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Asbestosis: 15-mark MD exam answer
Definition
Asbestosis is a chronic, diffuse interstitial fibrosing lung disease caused by inhalation and retention of asbestos fibers, especially after prolonged occupational exposure and long latency. It is a form of pneumoconiosis.
Etiology and risk exposures
Common high-risk occupations:
- Mining and milling of asbestos
- Shipyard work
- Insulation work
- Construction, demolition, asbestos cement industry
- Brake/lining manufacture and repair
- Textile and roofing industries
Risk is related to:
- Fiber burden (intensity x duration)
- Fiber type (amphiboles are more fibrogenic and biopersistent than chrysotile)
- Time since first exposure (typically decades)
Pathogenesis
- Inhaled fibers deposit at respiratory bronchioles/alveolar ducts.
- Fibers migrate into interstitium and trigger macrophage alveolitis.
- Incomplete clearance leads to persistent inflammation.
- Macrophages release cytokines and oxidants (TNF-alpha, IL-1, growth factors, ROS) causing fibroblast activation and collagen deposition.
- Progressive peribronchiolar fibrosis extends to diffuse interstitial fibrosis and honeycombing in advanced disease.
Key concept: disease may progress even after exposure stops due to retained fibers.
Pathology
Gross:
- Predominantly lower-lobe, subpleural fibrosis
- Small stiff lungs in advanced stage
- Pleural thickening/plaques may coexist
Microscopy:
- Early peribronchiolar fibrosis with chronic interstitial inflammation
- Type II pneumocyte hyperplasia
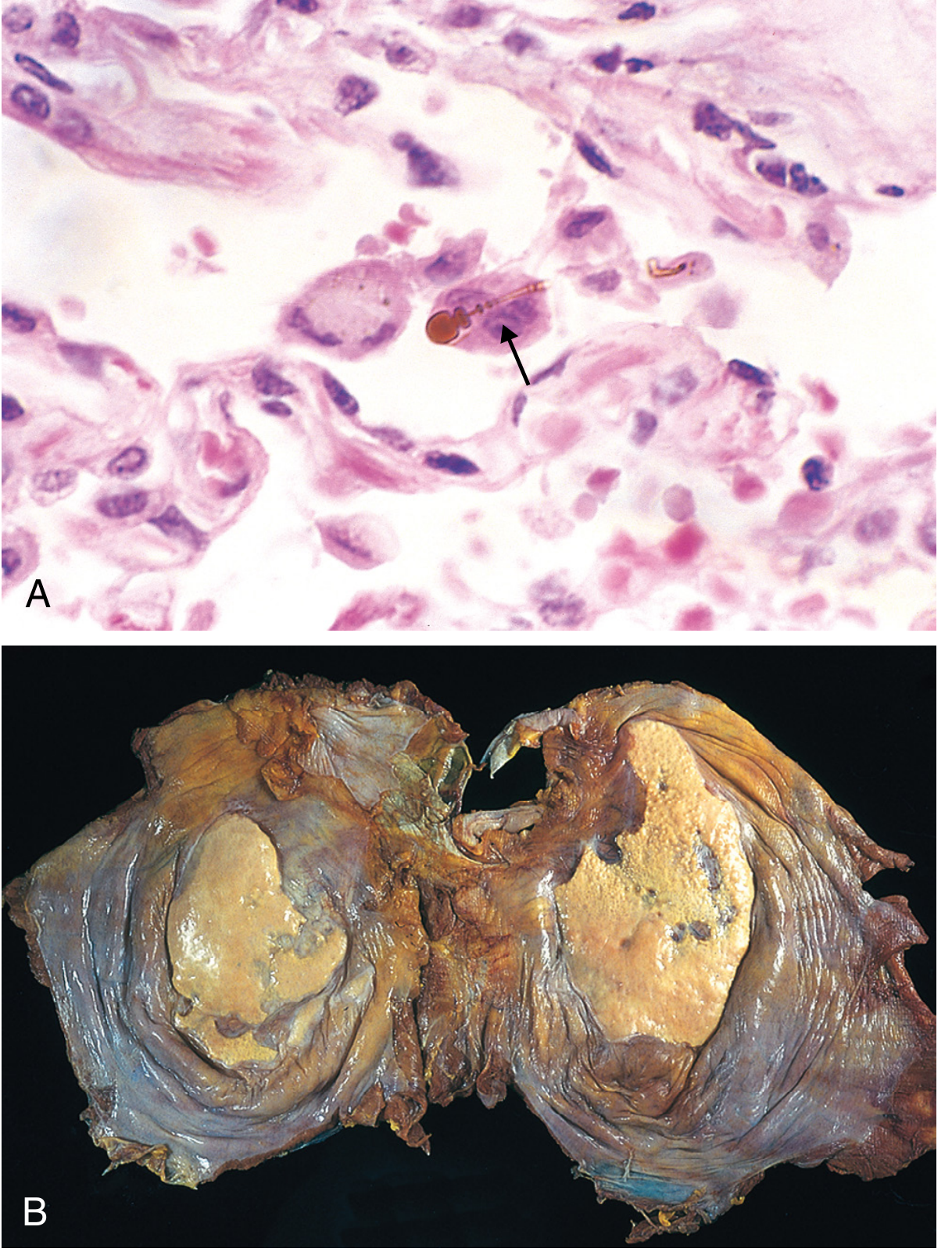
- Hallmark: asbestos bodies (ferruginous bodies): golden-brown, beaded/clubbed rods with iron-protein coating
- Advanced disease: diffuse interstitial fibrosis and honeycombing
Clinical features
- Long latency: usually 10 to 20+ years after first exposure
- Progressive exertional dyspnea (most common)
- Dry cough
- Bibasal fine end-inspiratory crackles (classically persistent)
- Clubbing in some cases
- Late: respiratory failure, pulmonary hypertension/cor pulmonale
Imaging findings
Chest X-ray:
- Bilateral lower-zone irregular/reticular opacities
- May show shaggy heart border in basal fibrosis
- Pleural plaques support asbestos exposure
HRCT (more sensitive):
- Subpleural curvilinear lines
- Intralobular/interlobular septal thickening
- Parenchymal bands
- Early honeycombing (advanced disease)
- Pleural plaques, pleural thickening, rounded atelectasis
- Better than CXR for early disease detection
Pulmonary function tests
Typical:
- Restrictive ventilatory defect (reduced FVC, TLC)
- Reduced DLCO
- Hypoxemia in advanced disease Mixed restrictive-obstructive pattern can occur, especially with airway involvement or smoking.
Diagnostic approach
Diagnosis is clinicoradiologic with exposure linkage:
- Definite occupational/environmental asbestos exposure history
- Compatible latency
- Typical imaging (especially lower-lobe interstitial fibrosis +/- pleural disease)
- PFT support (restriction +/- low DLCO)
- Exclusion of other ILDs (IPF, CTD-ILD, chronic HP, silicosis, etc.)
Histology/lung biopsy is not routinely needed if exposure plus radiology are typical; consider when diagnosis is uncertain.
Differential diagnosis
- Idiopathic pulmonary fibrosis (UIP)
- Other pneumoconioses (silicosis, coal worker pneumoconiosis)
- Chronic hypersensitivity pneumonitis
- CTD-associated ILD
- Drug/radiation-induced fibrosis
- Sarcoidosis (fibrotic stage)
Complications
- Progressive respiratory insufficiency
- Pulmonary hypertension and cor pulmonale
- Pleural disease: plaques, diffuse pleural fibrosis, benign pleural effusions
- Malignancy:
- Bronchogenic carcinoma (strongly increased with smoking; multiplicative interaction)
- Malignant mesothelioma
- Other asbestos-associated cancers (e.g., laryngeal, ovarian)
Management
No curative antifibrotic treatment is established specifically for asbestosis in standard texts.
Principles:
- Immediate cessation of further exposure
- Smoking cessation (critical)
- Vaccination (influenza, pneumococcal as indicated)
- Bronchodilators if airflow limitation
- Pulmonary rehabilitation
- Long-term oxygen therapy when hypoxemic
- Treat complications (pulmonary HTN, infections, failure)
- Surveillance for lung cancer/mesothelioma in high-risk individuals
- Occupational health notification, compensation, and preventive workplace control
Prognosis
- Variable; mild disease may remain stable
- Progressive decline can occur, including after exposure ceases
- Prognosis worsens with heavy cumulative exposure, advanced fibrosis, and malignancy
- Major causes of mortality: respiratory failure, lung cancer, mesothelioma
High-yield exam add-ons (to score better)
- Earliest pathology: peribronchiolar fibrosis at respiratory bronchioles/alveolar ducts
- Distribution: lower-lobe and subpleural predominance (unlike silicosis upper-zone tendency)
- Diagnostic hallmark: asbestos bodies on histology
- Most common pleural manifestation: pleural plaques
- Most feared malignancies: bronchogenic carcinoma and mesothelioma
- Smoking interaction: markedly magnifies lung cancer risk in exposed workers
Image (classic asbestos body + pleural plaques)
Textbook basis
- Fishman’s Pulmonary Diseases and Disorders, chapter on Asbestosis (pathology, pathogenesis, PFT, imaging, treatment/prognosis)
- Murray and Nadel’s Textbook of Respiratory Medicine, asbestos-related fibrosis section (clinical, radiology, diagnosis, natural history)
- Robbins Pathologic Basis of Disease, pneumoconioses chapter (morphology, asbestos bodies, clinicopathologic correlation)
If you want, I can also give you a 1-page last-minute revision format (definition -> etiopathogenesis -> clinicoradiology -> diagnosis -> management -> complications) for quick recall before exam.
This is a shared conversation. Sign in to Orris to start your own chat.