Retrosternal goiter with ct images
Reading File
Finding Sources
Finding Sources
Searching PubMed
retrosternal goiter CT imaging
Reading File
Reading File
Finding Sources
Searching the Web
retrosternal goiter CT imaging features radiology diagnosis 2024
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Reading File
Reading Web Page
substernal retrosternal goiter CT imaging features
Loading Image
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
I now have comprehensive textbook content and multiple CT images. Let me compile the full answer.
Retrosternal Goiter - CT Imaging
Definition and Terminology
Retrosternal goiter (also called substernal, intrathoracic, or cervicomediastinal goiter) refers to an enlarged thyroid gland with extension below the thoracic inlet. The most commonly used definitions are:
- Any goiter extending below the thoracic inlet (in surgical position)
- Any goiter where more than 50% of the gland lies below the thoracic inlet
A primary intrathoracic goiter is a distinct and rarer entity - it originates from ectopic thyroid tissue within the mediastinum and has no connection to the cervical thyroid gland.
The Swiss anatomist Haller first described intrathoracic thyroid extension in 1749, and Klein performed the first reported removal in 1820. - Scott-Brown's Otorhinolaryngology Head & Neck Surgery
Why CT is the Imaging Modality of Choice
CT is the single most important imaging tool for retrosternal goiter. - Fishman's Pulmonary Diseases and Disorders
Key reasons:
- Ultrasound cannot evaluate the intrathoracic portion (it cannot scan past the sternum)
- CT allows full assessment of inferior extent, shape, mediastinal compartment, and mass effect on adjacent structures
- Critical rule: If the distal extent of a goiter cannot be palpated, a CT scan is mandatory to assess intrathoracic extension. - Scott-Brown's Otorhinolaryngology
- CT gives better anatomic delineation than ultrasound for preoperative planning
CT Protocol
| Protocol | Indication |
|---|---|
| Non-contrast CT | First-line; best for confirming substernal thyroid identity (iodine content causes spontaneous hyperattenuation) |
| Contrast-enhanced CT | Preferred when suspecting locally advanced malignancy, invasion of adjacent structures, or bulky nodal metastases |
| Scan range | Must extend from skull base to tracheal bifurcation - not just the neck |
- Sabiston Textbook of Surgery
CT Findings
Characteristic Features
1. Spontaneous Hyperattenuation on Non-Contrast CT
Because of its iodine content, substernal thyroid tissue appears spontaneously hyperattenuating (bright) compared to surrounding muscle on a non-contrast scan - without needing IV contrast. This is the most useful distinguishing feature from other mediastinal masses. - Fishman's Pulmonary Diseases
2. Continuity with Cervical Thyroid
A visible connection from the intrathoracic mass to the cervical thyroid gland confirms the diagnosis in most cases.
3. Heterogeneous Attenuation
Cystic areas, calcifications, and foci of colloid or hemorrhage create a heterogeneous appearance typical of multinodular goiter.
4. Location - Anterior vs. Posterior Mediastinum
- Most goiters extend into the anterior mediastinum, anterior to the trachea
- Extension into the posterior mediastinum (paratracheal, paraesophageal) is less common but surgically significant - requires lateral thoracotomy in most cases
- Primary intrathoracic goiters often lie in the right paratracheal or posterior mediastinal position
CT Images
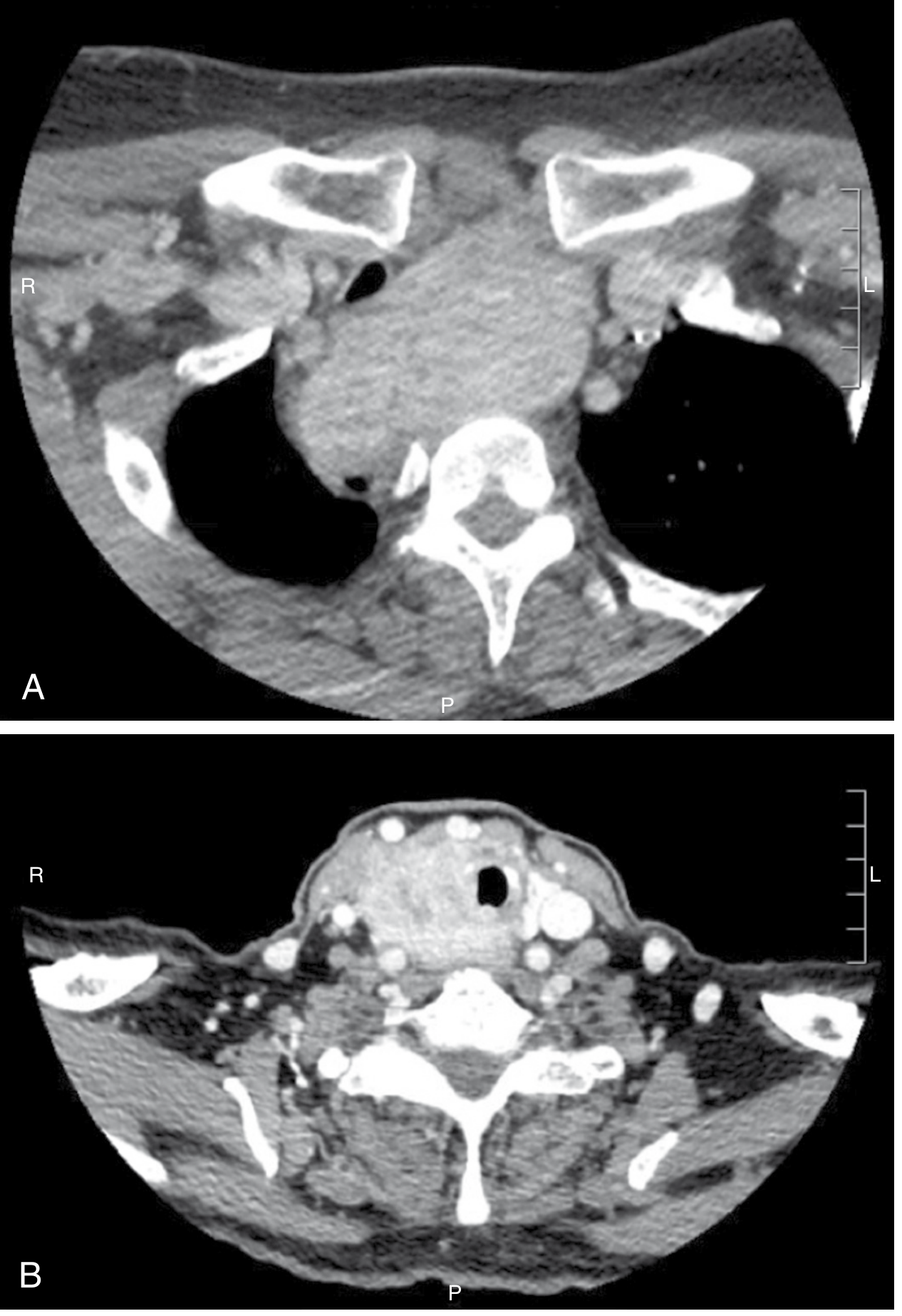
Figure 1 - Axial CT: Substernal thyroid with tracheal compression
(From Radiopaedia: axial CT at the thoracic inlet showing heterogeneous bilateral thyroid tissue with marked tracheal narrowing)

Figure 2 - Coronal CT: Classic substernal extension
(From Fischer's Mastery of Surgery - coronal reconstruction showing thyroid goiter descending from the neck into the superior mediastinum)

Coronal reconstruction of CT scan demonstrating substernal extension of thyroid goiter. The mass originates from the cervical thyroid and descends into the superior-anterior mediastinum. - Fischer's Mastery of Surgery
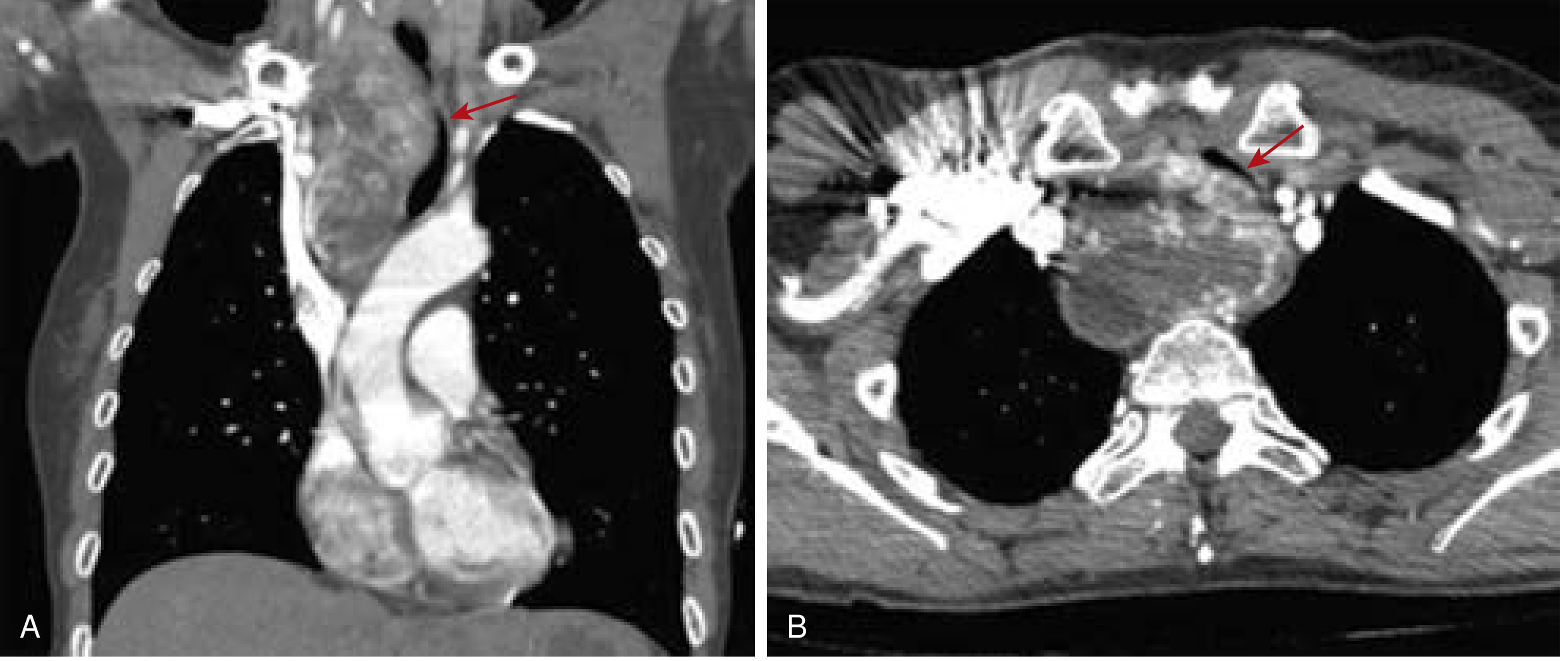
Figure 3 - Contrast CT: Tracheal deviation and compression
(From Sabiston Textbook of Surgery - two-panel contrast CT)
(A) Contrast-enhanced CT demonstrating a left-sided substernal goiter extending into the posterior mediastinum, crossing to the right side, with tracheal compression and deviation of both trachea and esophagus. (B) Contrast-enhanced CT of a locally advanced follicular thyroid cancer with invasion into the tracheal wall and esophagus, and obliteration of the right internal jugular vein. - Sabiston Textbook of Surgery
Figure 4 - Coronal and Axial CT: Right-sided substernal goiter with tracheal deviation
(From Current Surgical Therapy - 68-year-old woman presenting with stridor)
A 68-year-old woman with incidental goiter on workup for dyspnea. No palpable thyroid mass, but mild inspiratory stridor. CT shows a large right-sided substernal thyroid with (A) tracheal deviation to the left (coronal) and (B) severe narrowing of tracheal lumen (axial). - Current Surgical Therapy 14e
Figure 5 - Sagittal CT: Primary intrathoracic goiter
(From Scott-Brown's Otorhinolaryngology - parasagittal view)
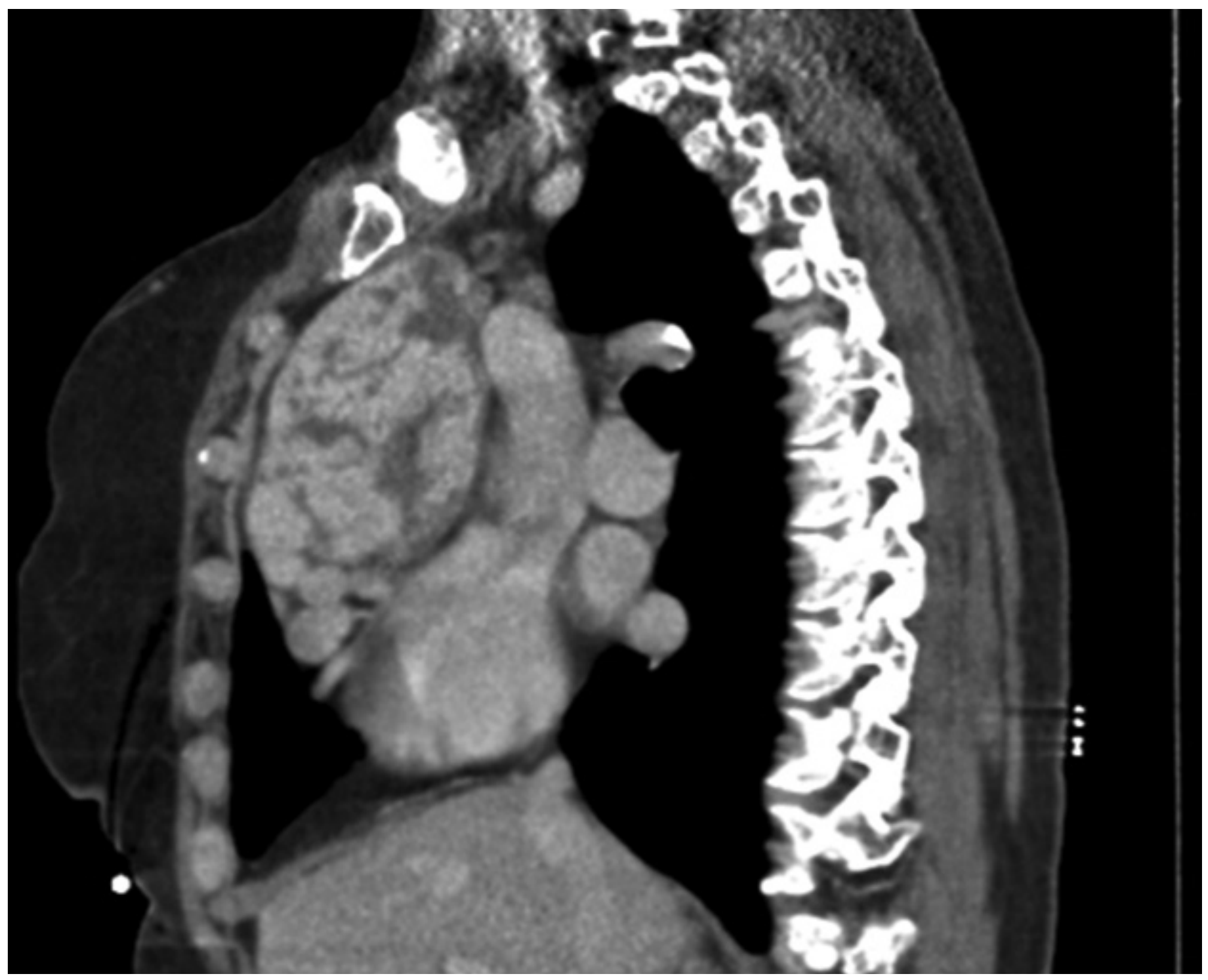
Sagittal CT/MRI demonstrating a primary intrathoracic goiter as a large posterior mediastinal mass adjacent to the vertebral column - with no direct continuity to the cervical thyroid gland. - Scott-Brown's Otorhinolaryngology
CT Features Predicting Need for Sternotomy
The following CT features suggest a thoracic (sternal) approach will be needed rather than a standard transcervical incision:
| CT Finding | Surgical Implication |
|---|---|
| Extension below the aortic arch | Sternotomy likely required |
| Extension into the posterior mediastinum | Lateral thoracotomy often needed |
| Primary intrathoracic goiter (no cervical connection), especially right-sided | Higher sternotomy risk |
| Large total thyroid volume | Harder transcervical delivery |
| Extension below the tracheal carina | Highest risk for sternotomy |
| Features suggesting malignancy (irregular margins, invasion, nodes) | Sternotomy + wider resection |
- Scott-Brown's Otorhinolaryngology; Radiopaedia
The majority of anterior substernal goiters - even large ones - can still be removed via a transcervical approach alone in experienced centers, using full neck extension and blunt digital dissection.
Mass Effect on Adjacent Structures
CT systematically assesses:
- Trachea: Deviation (usually away from the dominant lobe), compression, luminal narrowing - the most common complication
- Esophagus: Displacement (usually posterior and contralateral)
- Great vessels: SVC, brachiocephalic vein compression - presents as dilated chest wall veins (Pemberton's sign physiology)
- Recurrent laryngeal nerve: Not directly visible but its course is traced; hoarseness is a clinical correlate
- Vascular anomalies: CT identifies lusoria artery and other variants that alter surgical anatomy
From Schwartz's Principles of Surgery: "Retrosternal extension of a large goiter may result in impeded flow in the superior vena cava, leading to dilated veins over the chest wall."
Differential Diagnosis of Superior Mediastinal Mass on CT
When a superior/anterior mediastinal mass is found, CT differentials include:
| Diagnosis | CT Clue |
|---|---|
| Retrosternal goiter | Hyperattenuating on non-contrast; continuity with cervical thyroid |
| Thymoma | Anterior mediastinum; no cervical connection; soft tissue attenuation |
| Lymphoma | Homogeneous, bulky anterior/middle mediastinal nodes |
| Teratoma | Fat/calcium/teeth on CT (classic) |
| Aortic aneurysm | Vascular; pulsatile; contrast fills lumen |
| Parathyroid adenoma | Tiny, near thyroid; sestamibi scan confirmatory |
Role of Other Imaging Alongside CT
| Modality | Role |
|---|---|
| Ultrasound | First-line for accessible cervical thyroid; cannot image intrathoracic component |
| MRI | Useful adjunct; better soft tissue delineation; no radiation; T1/T2 hyperintense thyroid |
| Nuclear scintigraphy (I-123/Tc-99m) | Useful for ectopic tissue or primary intrathoracic goiter with no cervical connection; intra-thoracic goiters often show limited iodine avidity |
| FDG-PET/CT | Only for suspected malignancy, RAI-refractory differentiated thyroid cancer |
Key Clinical Points
- 80% of retrosternal goiters are euthyroid; up to 30% have subclinical TSH suppression
- Risk of malignancy in intrathoracic goiters is up to 11% - this is one indication for surgery even in asymptomatic patients
- Surgical management is the definitive treatment; transcervical approach suffices in the vast majority
- Radioiodine (¹³¹I) can reduce goiter size 30-45% over 1-2 years, but is contraindicated with compressive symptoms (risk of acute swelling)
- Pemberton's sign: Arms raised above head causes facial congestion/flushing/SVC compression - a bedside sign of significant substernal extension
Sources: Sabiston Textbook of Surgery; Fischer's Mastery of Surgery 8th ed.; Scott-Brown's Otorhinolaryngology Head & Neck Surgery; Fishman's Pulmonary Diseases and Disorders; Current Surgical Therapy 14e; Schwartz's Principles of Surgery 11th ed.; Radiopaedia - Substernal goiter
This is a shared conversation. Sign in to Orris to start your own chat.