A 25-year-old man comes to an outpatient clinic complaining of low-grade fever and sore throat, and he receives an injection of intramuscular penicilin for pre sumed streptococcal pharyngitis. He is otherwise healthy and takes no regular medications. Within 20 minutes, he begins to complain of swelling of his face and difficulty breathing. He looks dyspneic and frightened. His heart rate is 130 bpm, blood pressure 90/47 mm Hg, and respiratory rate 28 breaths per minute and shallow. His face and lips are edematous, and he can barely open his eyes because of swelling. He is wheezing diffusely, and he has multiple raised urticarial lesions on his skin. An ambulance has been called.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have excellent, comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
Anaphylaxis - Penicillin-Induced
Diagnosis
This patient has anaphylaxis - a severe, life-threatening, systemic hypersensitivity reaction. The diagnosis is clinical. He meets the criteria definitively:
- Known allergen exposure (IM penicillin) within 20 minutes
- Multi-system involvement:
- Cutaneous/mucosal: facial and lip angioedema, urticaria, periorbital edema
- Respiratory: dyspnea, wheezing (bronchospasm), tachypnea (RR 28, shallow)
- Cardiovascular: hypotension (BP 90/47), tachycardia (HR 130)
This is a Type I IgE-mediated hypersensitivity reaction (Gell and Coombs Classification).
Immunologic Mechanism
Sensitization phase (prior exposure):
- Penicillin (a hapten) binds to serum proteins, forming a penicillin-protein conjugate that acts as a complete antigen.
- This is processed by antigen-presenting cells and presented to Th2 CD4+ T cells.
- Th2 cytokines (IL-4, IL-13) drive B-cell class switching to produce penicillin-specific IgE antibodies.
- These IgE antibodies bind to high-affinity FcεRI receptors on mast cells and basophils throughout the body - the patient is now sensitized.
Effector/Elicitation phase (current exposure):
- Re-exposure to penicillin (IM injection) introduces penicillin-protein conjugates into circulation rapidly (parenteral route bypasses GI barriers).
- Penicillin cross-links two adjacent IgE-FcεRI complexes on the mast cell surface.
- This cross-linking triggers mast cell degranulation - an explosive release of preformed and newly synthesized mediators:
| Mediator | Effect |
|---|---|
| Histamine (preformed) | Vasodilation, increased vascular permeability, bronchoconstriction, urticaria, angioedema |
| Tryptase (preformed) | Activates complement, activates kinin system |
| Leukotrienes C4/D4/E4 (newly synthesized) | Potent bronchoconstriction (10-1000x more potent than histamine), increased mucus secretion |
| Prostaglandin D2 (newly synthesized) | Vasodilation, bronchoconstriction |
| PAF (newly synthesized) | Platelet activation, vasodilation, bronchoconstriction |
| TNF-α, IL-4, IL-13 (cytokines) | Amplify inflammatory response, recruit eosinophils |
- Massive histamine release causes H1-mediated smooth muscle contraction (bronchospasm → wheezing, dyspnea) and H1/H2-mediated vasodilation + capillary leak (angioedema, urticaria, hypotension).
- The sudden loss of intravascular volume and peripheral vasodilation causes distributive shock (hypotension, tachycardia).
Parenteral administration of penicillin is particularly dangerous because the antigen enters the bloodstream directly and rapidly - bypassing any mucosal barriers. The faster the onset of symptoms after exposure, the more severe the reaction. - Rosen's Emergency Medicine, 9e
Why Penicillin is the Most Common Drug Cause
Penicillin is the most common antibiotic cause of anaphylaxis among the beta-lactam antibiotics. Key points:
- Although up to 10% of the population reports a penicillin allergy, true IgE-mediated allergy (confirmed by skin testing) exists in fewer than 10% of those who report it.
- The beta-lactam ring is the primary hapten - it opens and covalently binds lysine residues on serum proteins to form the "penicilloyl" major determinant.
- Cross-reactivity exists between penicillins and some cephalosporins (~1-2%), particularly those with similar R-group side chains.
Immediate Management (Priority Order)
This is a medical emergency. The ambulance should be directed to arrive with full resuscitation capability.
1. EPINEPHRINE - First-Line, No Exceptions
Epinephrine is the medication of choice for treatment of anaphylaxis. There are no absolute contraindications. - The Washington Manual of Medical Therapeutics
Antihistamines and corticosteroids should NOT be considered first-line medications - there is no objective evidence they improve overall outcome. - Rosen's Emergency Medicine
- Epinephrine 0.3-0.5 mg (1:1000, i.e., 1 mg/mL) IM into the anterolateral thigh (vastus lateralis) - fastest absorption compared to deltoid or subcutaneous.
- Repeat every 5-15 minutes as needed if no improvement.
- Mechanism: α1 agonism reverses vasodilation and angioedema; β1 increases cardiac output; β2 relieves bronchospasm and inhibits further mediator release from mast cells.
2. Position
- Supine with legs elevated (improves venous return, counters distributive shock).
- Do NOT allow patient to stand up suddenly - "empty ventricle" syndrome can cause cardiac arrest.
3. Airway Management
- High-flow oxygen via non-rebreather mask immediately (SpO2 target ≥95%).
- The patient's face/lip angioedema and wheezing represent a threatened airway - prepare for early intubation if not improving with epinephrine. Delay can make intubation impossible as edema progresses.
- Have cricothyrotomy kit at bedside as a backup.
- Nebulized albuterol/salbutamol for persistent bronchospasm as adjunct (NOT a replacement for epinephrine).
4. IV Access and Fluids
- Establish two large-bore IV lines.
- IV crystalloid bolus: 1-2 L normal saline (or Ringer's lactate) rapidly for hypotension - massive fluid shifts occur due to capillary leak.
- Up to 5-10 L may be required in refractory cases.
5. Second-Line Medications (adjuncts only, after epinephrine)
| Drug | Dose | Rationale |
|---|---|---|
| H1 antihistamine (diphenhydramine) | 25-50 mg IV/IM | Reduces urticaria, pruritus - does NOT help hemodynamics |
| H2 antihistamine (ranitidine/famotidine) | 50 mg IV | Additive to H1 blockade for cutaneous symptoms |
| Corticosteroids (methylprednisolone) | 125 mg IV | Prevent/reduce biphasic anaphylaxis; no benefit in acute phase |
| Glucagon | 1-5 mg IV over 5 min | For patients on beta-blockers who fail epinephrine (bypasses β-receptor) |
6. Refractory Anaphylaxis (if no response to IM epinephrine)
- IV epinephrine infusion: 1-10 mcg/min titrated to response - requires continuous monitoring.
- Vasopressors (norepinephrine, vasopressin) for refractory shock.
7. Monitoring and Observation
- Continuous cardiac monitoring, pulse oximetry.
- Observe for at least 4-8 hours after stabilization because of the biphasic reaction - a second wave of anaphylaxis can occur 1-72 hours (typically 8-11 hours) after the initial reaction as newly synthesized leukotrienes are released. Reported incidence: 4-20%.
- Discharge with epinephrine autoinjector x2 (EpiPen) and instructions.
- Refer to allergist for formal evaluation, penicillin skin testing, and desensitization counseling.
Summary Table: Why Each Sign/Symptom Occurs
| Clinical Finding | Mediator Responsible |
|---|---|
| Urticaria | Histamine → dermis vasodilation + exudation |
| Angioedema (face, lips) | Histamine + bradykinin → deep dermal/submucosal edema |
| Wheezing | Leukotrienes + histamine → bronchospasm |
| Tachypnea, dyspnea | Bronchospasm + laryngeal edema |
| Hypotension (90/47) | Histamine → vasodilation + capillary leak → distributive shock |
| Tachycardia (130 bpm) | Compensatory response to hypotension + epinephrine surge |
Sources:
- Rosen's Emergency Medicine: Concepts and Clinical Practice, 9e - Chapter 106: Anaphylaxis
- Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 9e - Chapter 14
- Roitt's Essential Immunology, 13e - Chapter 14: Hypersensitivity
- The Washington Manual of Medical Therapeutics - Anaphylaxis section
Is it dangerous if headache starts 12 hrs after falling
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
I now have everything needed for a thorough, well-illustrated answer.
⚠️ Yes - A Headache Starting 12 Hours After a Fall Can Be Dangerous
Go to an emergency department immediately. A headache that begins hours after a head injury - rather than right away - is a classic warning sign of intracranial bleeding, and should never be assumed to be "just a headache."
What Could Be Happening
The skull is a fixed, rigid box. Any blood that collects inside it compresses the brain. The dangerous part is that bleeding can be slow and silent at first - you feel fine for hours, then symptoms appear as blood accumulates.
The 3 Main Types of Post-Traumatic Intracranial Bleeding
| Type | Source of Bleeding | Timing of Symptoms | Key Feature |
|---|---|---|---|
| Epidural Hematoma (EDH) | Arterial (middle meningeal artery) | Minutes to hours | Classic "lucid interval" - feel okay, then rapidly worsen |
| Subdural Hematoma (SDH) - Acute | Torn bridging veins | Within 24 hours | Often headache + confusion + weakness |
| Subdural Hematoma - Subacute/Chronic | Torn bridging veins (slow ooze) | Days to weeks later | Headache, subtle personality/memory changes |
A 12-hour delayed headache fits all three of these timelines.
Epidural Hematoma - The "Lucid Interval"
This is the most dangerous scenario. Blood from a ruptured artery (usually the middle meningeal artery from a temporal skull fracture) accumulates rapidly between the skull and dura.
"The classic presentation of an EDH is head trauma producing a decreased LOC followed by a so-called lucid interval. Although the patient's LOC is generally normal or only slightly depressed, a completely normal mental status may not return before a second episode of decreased consciousness occurs." - Rosen's Emergency Medicine, 9e
The pattern: hit head → briefly dazed → feel fine for hours → headache → rapidly deteriorates → coma. This can be fatal within hours if not surgically drained.
Subdural Hematoma - The Slow Bleed
Blood from torn bridging veins accumulates more slowly between the dura and brain.
"Subdural hematoma tends to collect more slowly than epidural hematoma because of its venous origin... Acute symptoms usually develop within 14 days of injury." - Tintinalli's Emergency Medicine, 9e
Acute SDH (symptoms within 24 hours): Headache + decreased consciousness + one-sided weakness. Mortality is 40-60% in cases requiring surgery.
Chronic SDH (symptoms weeks later): Can be subtle - mild headache, confusion, personality changes, weakness. Often seen after minor bumps in elderly or people who drink heavily.
CT Scan Appearances
Acute subdural hematoma - the crescent-shaped white (hyperdense) collection hugging the brain surface:

CT scan: Small right frontotemporal subdural hematoma (Tintinalli's Emergency Medicine)
Larger acute subdural with significant brain compression:
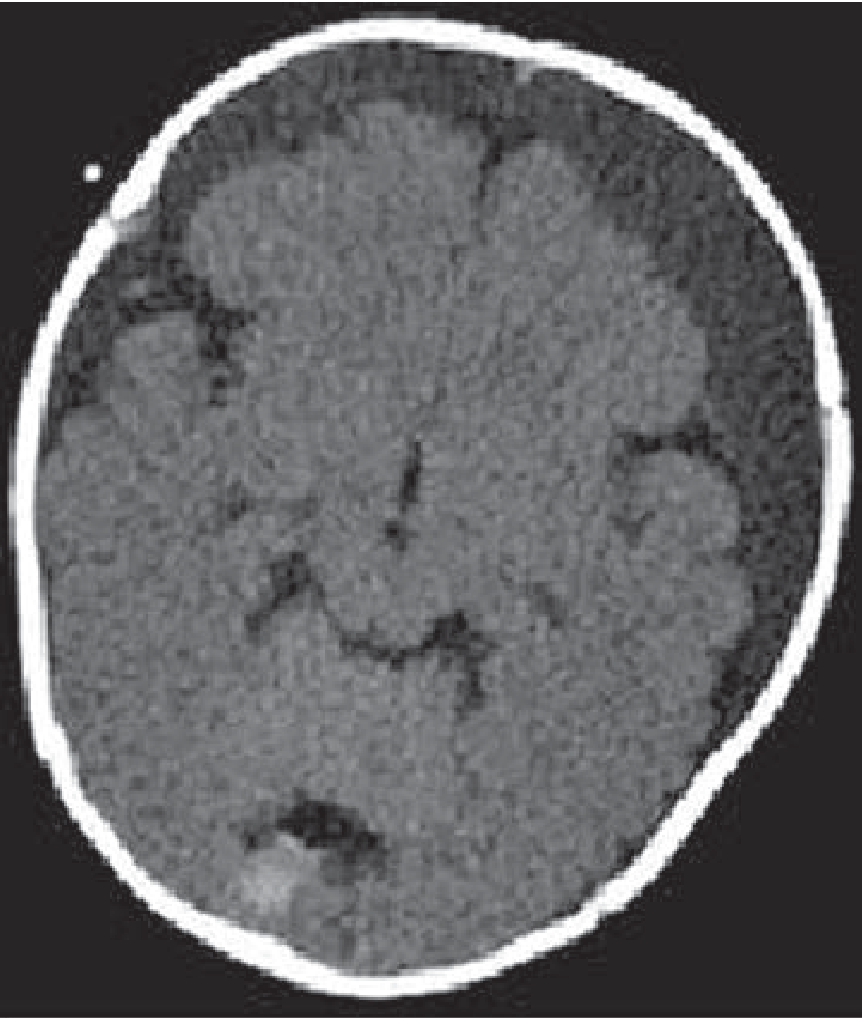
CT scan: Large acute subdural hematoma - note the significant shift and compression of brain tissue (Tintinalli's Emergency Medicine)
🚨 Red Flag Symptoms - Seek Emergency Care IMMEDIATELY
If headache after a fall is accompanied by ANY of the following, call emergency services (911/999/112) right now - do not wait:
- Headache that is getting worse over time (not staying the same or improving)
- Confusion, disorientation, or unusual behavior
- Drowsiness that is hard to fight off, or difficulty waking the person up
- Weakness or numbness on one side of the body, face drooping
- Vomiting (especially repeated vomiting)
- Seizures
- Unequal pupils (one bigger than the other)
- Slurred speech
- Loss of consciousness at any point
Even without these symptoms, a new headache 12 hours after a head injury still warrants medical evaluation that day - at minimum a call to a doctor or urgent care visit.
Who Is at Highest Risk
Some people are especially vulnerable to intracranial bleeding from even minor falls:
- Elderly people - the brain shrinks with age, stretching the bridging veins; even a seemingly minor fall can cause a bleed
- People on blood thinners (warfarin, aspirin, clopidogrel, apixaban, rivaroxaban) - bleeding is harder to stop and expands faster
- Chronic alcohol users - brain atrophy + clotting problems
- Children under 2 years old - bridging veins are more vulnerable
"Even seemingly benign falls from a standing position can result in subdural bleeding in the elderly." - Tintinalli's Emergency Medicine, 9e
Bottom Line
A headache 12 hours after a fall is not normal and should be evaluated urgently. The most dangerous cause - intracranial bleeding - can be diagnosed quickly with a CT scan of the head, which takes only minutes to perform. If caught early, surgical drainage (burr hole or craniotomy) can be lifesaving. If you or someone you know is in this situation, do not wait to see if it improves on its own.
Sources: Rosen's Emergency Medicine, 9e; Tintinalli's Emergency Medicine, 9e; Plum and Posner's Diagnosis and Treatment of Stupor and Coma
This is a shared conversation. Sign in to Orris to start your own chat.