Hii
Hey! How's it going? I'm Orris. What can I help you with today?
Could you explain about adrenergic receptors
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have thorough content from Goodman & Gilman's and Barash's Clinical Anesthesia. Here is the full explanation:
Adrenergic Receptors
Adrenergic receptors (adrenoceptors) are G-protein coupled receptors (GPCRs) that respond to catecholamines - primarily epinephrine (EPI) and norepinephrine (NE). The classification into alpha (α) and beta (β) types was first proposed by Ahlquist in 1948, based on the different response patterns of these two drugs.
Structure
All adrenergic receptors share the classic heptahelical (7 transmembrane-spanning) GPCR structure. The three β-receptor subtypes share about 60% amino acid sequence identity within the membrane-spanning domains, where the catecholamine ligand-binding pockets are located. The sizes of the third and fourth intracellular loops differ among subtypes, accounting for differences in G-protein coupling.
Classification and Subtypes
α-Adrenergic Receptors
Further divided into α1 and α2, distinguished pharmacologically by their sensitivity to:
- Prazosin - more potent antagonist at α1
- Yohimbine - more potent antagonist at α2
Each is further subdivided by molecular cloning:
- α1: α1A, α1B, α1D
- α2: α2A, α2B, α2C
α1 Receptors
- Location: Postsynaptic smooth muscle of peripheral vasculature, coronary arteries, skin, uterus, intestinal mucosa, splanchnic beds; postjunctional only (no presynaptic α1 receptors have been identified)
- Signaling: Couple to Gq → activate phospholipase C → IP3 + DAG → increased intracellular Ca²⁺
- Effects:
- Vasoconstriction (resistance and capacitance vessels)
- Intestinal smooth muscle relaxation
- Positive inotropic effect in the heart
- Role in catecholamine-induced ventricular arrhythmias during ischemia/reperfusion
α2 Receptors
- Location: Both presynaptic and postsynaptic membranes
- Presynaptic α2: Act as autoreceptors - inhibit further NE release (negative feedback). DA2 receptors similarly inhibit release.
- Postsynaptic α2 effects:
- Arterial and venous vasoconstriction
- Platelet aggregation
- Inhibition of insulin release
- Inhibition of bowel motility
- Stimulation of growth hormone release
- Inhibition of ADH release
- Modulation of baroreceptor reflex (increased sensitivity), bradycardia, bronchoconstriction
- Signaling: Couple to Gi → inhibit adenylyl cyclase → decreased cAMP
β-Adrenergic Receptors
Three subtypes: β1, β2, β3
All three couple to Gs → activate adenylyl cyclase → ↑ cAMP → activate PKA → phosphorylation of cellular proteins. In addition, Gβγ subunits can directly enhance voltage-sensitive Ca²⁺ channels in skeletal and cardiac muscle.
| Subtype | Primary Location | Key Effects |
|---|---|---|
| β1 | Heart, kidney (JG cells) | ↑ HR (chronotropy), ↑ contractility (inotropy), ↑ renin release |
| β2 | Lungs (bronchi), vascular smooth muscle, liver, skeletal muscle | Bronchodilation, vasodilation, glycogenolysis, ↑ insulin secretion |
| β3 | Adipose tissue | Lipolysis (thermogenesis in brown fat) |
- β1 is the major adrenergic receptor in the human heart, primarily stimulated by NE
- β2 receptors on the presynaptic membrane actually increase NE release (positive feedback, contrast to presynaptic α2)
- β2 in cardiac myocytes can dually couple to both Gs and Gi, producing complex chronotropic effects
Receptor Location: Pre- vs. Postsynaptic
The diagram below from Barash's Clinical Anesthesia illustrates pre- and postsynaptic receptor positions at the adrenergic synapse:
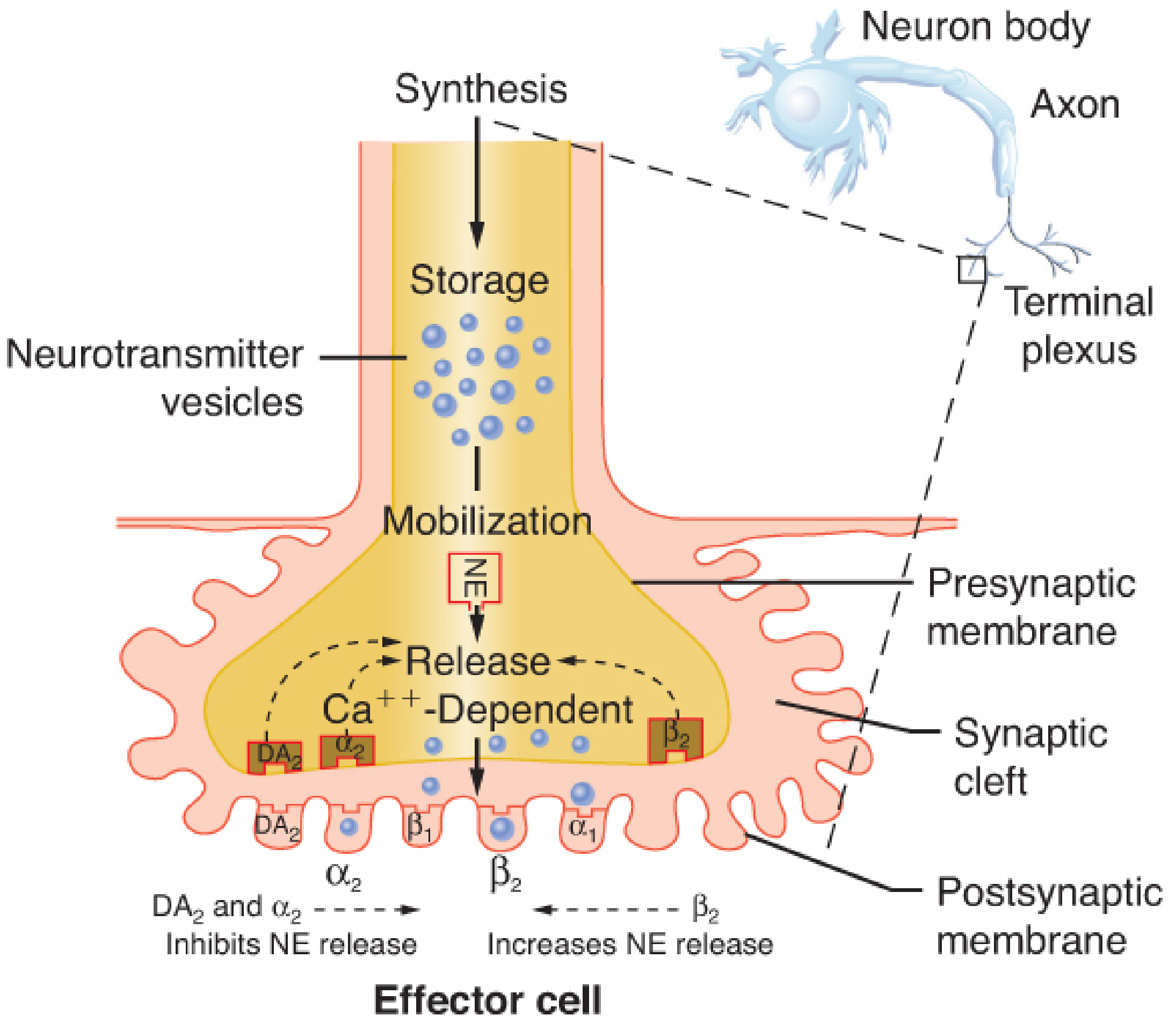
- Presynaptic α2 and DA2: Inhibit NE release (negative feedback)
- Presynaptic β2: Increase NE release (positive feedback)
- Postsynaptic α2 and β2: Extrasynaptic/hormonal receptors (not innervated directly)
Dopaminergic (DA) Receptors
A separate peripheral adrenergic receptor class responds to dopamine:
- DA1: Renal, mesenteric, and coronary vessels (vasodilation)
- DA2: Presynaptic; inhibit NE release (similar to α2)
Dopamine at increasing doses also activates α and β receptors in a dose-dependent manner.
Desensitization and Downregulation
Prolonged exposure to catecholamines leads to tachyphylaxis (refractoriness):
- GPCR kinases (GRKs) phosphorylate the activated receptor
- β-arrestin binds → blocks G-protein access
- Receptor is directed to endosomes (internalized) - reversible dephosphorylation can recycle receptor back
- Some receptors reach lysosomes and are degraded (downregulation)
The β2 receptor is most susceptible to desensitization. Long-term catecholamine exposure (mainly via β1) contributes to cardiac dysfunction and heart failure progression.
Biased Agonism
Modern pharmacology recognizes that different ligands binding the same receptor can stabilize different receptor conformations, activating only a subset of downstream signals (e.g., G-protein pathway only, or β-arrestin pathway only). This "biased agonism" offers the potential to design drugs with precise specificity - activating beneficial pathways while avoiding side effects.
Clinical Summary Table
| Receptor | Location | Signal | Key Agonist | Key Antagonist | Effect |
|---|---|---|---|---|---|
| α1 | Vascular smooth muscle, heart | Gq → ↑Ca²⁺ | Phenylephrine | Prazosin | Vasoconstriction, ↑inotropy |
| α2 | Presynaptic nerve terminals, platelets | Gi → ↓cAMP | Clonidine, dexmedetomidine | Yohimbine | ↓NE release, ↓BP, sedation |
| β1 | Heart, kidney | Gs → ↑cAMP | Dobutamine | Metoprolol, atenolol | ↑HR, ↑contractility, ↑renin |
| β2 | Bronchi, vessels, liver | Gs → ↑cAMP | Salbutamol, terbutaline | Propranolol (non-selective) | Bronchodilation, vasodilation |
| β3 | Adipose | Gs → ↑cAMP | Mirabegron (bladder β3) | - | Lipolysis, bladder relaxation |
Sources: Barash, Cullen, and Stoelting's Clinical Anesthesia, 9e, p. 1050-1053 | Goodman & Gilman's The Pharmacological Basis of Therapeutics, pp. 218-219
What are specific drugs that target each receptor subtype (agonists & antagonists)?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Excellent - I now have comprehensive data from Katzung's Basic & Clinical Pharmacology and other sources. Here is the full drug reference:
Drugs Targeting Adrenergic Receptor Subtypes
AGONISTS
α1 Agonists
These cause vasoconstriction and are used for hypotension, nasal decongestion, and mydriasis.
| Drug | Selectivity | Clinical Use |
|---|---|---|
| Phenylephrine | Selective α1 | Vasopressor for hypotension, nasal decongestant, mydriatic (eye drops) |
| Midodrine (prodrug → desglymidodrine) | Selective α1 | Orthostatic hypotension (oral, long-acting) |
| Methoxamine | Selective α1 | Paroxysmal SVT (raises BP to trigger vagal reflex) |
| Oxymetazoline / Xylometazoline | Predominantly α1 | Nasal decongestants (topical) |
Phenylephrine is not a catechol derivative - it is not inactivated by COMT and thus has a longer duration than catecholamines. - Katzung's Basic and Clinical Pharmacology, 16e
α2 Agonists
Act centrally to reduce sympathetic outflow ("sympatholytics"), used mainly as antihypertensives and sedatives.
| Drug | Key Use |
|---|---|
| Clonidine | Hypertension, ADHD, opioid/alcohol withdrawal, pain |
| Dexmedetomidine | ICU/procedural sedation, reduces opioid requirements |
| Methyldopa | Hypertension in pregnancy (drug of choice) |
| Guanfacine | Hypertension, ADHD |
| Guanabenz | Hypertension |
| Tizanidine | Centrally acting muscle relaxant (α2 in spinal cord) |
| Apraclonidine / Brimonidine | Glaucoma (topical - reduce aqueous humor secretion) |
Alpha2-selective agonists decrease blood pressure through CNS actions that reduce sympathetic tone, even though direct application to a vessel may cause vasoconstriction. - Katzung's Basic and Clinical Pharmacology, 16e
Non-selective α Agonists / Mixed Catecholamines
| Drug | Receptor Profile | Key Effects |
|---|---|---|
| Norepinephrine (NE) | α1, α2 >> β1; minimal β2 | ↑ systolic + diastolic BP; vasopressor of first choice in septic shock |
| Epinephrine (EPI) | α1, α2, β1, β2 (all) | ↑ HR, ↑ contractility, ↑ BP; anaphylaxis, cardiac arrest, local anesthetic adjunct |
| Dopamine (dose-dependent) | DA1 > β1 > α (low→high doses) | Low: renal vasodilation; moderate: ↑ cardiac output; high: vasoconstriction |
Norepinephrine is the vasopressor of first choice in shock - it has predominantly α-adrenergic properties but its modest β effects help maintain cardiac output. Dopamine has no advantage over norepinephrine and is associated with higher arrhythmia incidence. - Katzung's, 16e
β1 Agonists
Cardiac stimulants - used in heart failure, shock, bradycardia.
| Drug | Selectivity | Clinical Use |
|---|---|---|
| Dobutamine | β1 selective (also some β2/α1) | Acute heart failure, cardiogenic shock (inotrope of choice) |
| Isoproterenol | Non-selective β1+β2 | Severe bradycardia, AV block (rarely used now) |
β2 Agonists
Bronchodilators - cornerstone of asthma/COPD management.
| Drug | Duration | Clinical Use |
|---|---|---|
| Salbutamol (Albuterol) | Short-acting (SABA) | Acute asthma/bronchospasm rescue |
| Terbutaline | Short-acting | Bronchospasm; also tocolysis (preterm labor) |
| Metaproterenol | Moderate | Asthma |
| Salmeterol | Long-acting (LABA) | Asthma/COPD maintenance (not rescue) |
| Formoterol | Long-acting (LABA) | Asthma/COPD maintenance |
| Ritodrine | β2 selective | Tocolysis (uterine relaxation) |
β-Adrenoceptor agonists are best delivered by inhalation for greatest local airway effect with least systemic toxicity. - Katzung's Basic and Clinical Pharmacology, 16e
β3 Agonists
| Drug | Clinical Use |
|---|---|
| Mirabegron | Overactive bladder (relaxes detrusor muscle) |
| Vibegron | Overactive bladder |
ANTAGONISTS (BLOCKERS)
α1 Antagonists (α1 Blockers)
Cause vasodilation; used for hypertension and BPH.
| Drug | Clinical Use |
|---|---|
| Prazosin | Hypertension, BPH, PTSD nightmares |
| Terazosin | Hypertension, BPH |
| Doxazosin | Hypertension, BPH |
| Tamsulosin | BPH (highly uroselective α1A) |
| Silodosin | BPH (highly uroselective α1A) |
| Alfuzosin | BPH |
α2 Antagonists
| Drug | Clinical Use |
|---|---|
| Yohimbine | Research tool; historically used for erectile dysfunction |
| Mirtazapine | Antidepressant (blocks α2 autoreceptors → ↑ NE/5-HT release) |
| Idazoxan | Research only |
Non-selective α Antagonists
| Drug | Clinical Use |
|---|---|
| Phentolamine | Pheochromocytoma (pre-op), hypertensive crisis, reversal of local anesthetic vasoconstriction |
| Phenoxybenzamine | Pheochromocytoma (pre-op, irreversible/non-competitive) |
In pheochromocytoma, β-blockers must NEVER be given alone - unopposed α stimulation causes hypertensive crisis. α-blockers must be given first. - Rosen's Emergency Medicine
β1-Selective Antagonists ("Cardioselective" - 2nd Generation)
Safer in asthmatics at low doses (selectivity is relative and lost at high doses).
| Drug | Half-life | Notes |
|---|---|---|
| Metoprolol | 3-4 h | Heart failure, MI, hypertension, rate control |
| Atenolol | 6-9 h | Hypertension, angina |
| Bisoprolol | 9-12 h | Heart failure (with low starting dose) |
| Esmolol | 10 min | Ultra-short IV; intraoperative tachycardia/hypertension, SVT |
| Betaxolol | 14-22 h | Hypertension; also topical for glaucoma |
| Acebutolol | 3-4 h | Has partial agonist activity (ISA) |
Non-selective β Antagonists (1st Generation)
Block both β1 and β2 - avoid in asthma/COPD.
| Drug | Key Notes |
|---|---|
| Propranolol | Prototype; also blocks β in thyroid storm, migraine prophylaxis, essential tremor, portal hypertension |
| Nadolol | Long-acting, renally cleared |
| Timolol | Topical for glaucoma; also oral for hypertension |
| Sotalol | Also class III antiarrhythmic (K⁺ channel block) |
| Pindolol, Carteolol | Have partial agonist activity (ISA) |
Mixed α + β Antagonists (3rd Generation)
| Drug | Receptor Profile | Clinical Use |
|---|---|---|
| Labetalol | α1 + non-selective β | Hypertensive urgency/emergency in pregnancy, hypertension |
| Carvedilol | α1 + non-selective β | Chronic heart failure, post-MI, hypertension |
| Bucindolol | α1 + non-selective β | Heart failure (less commonly used) |
With mixed α1+β blockers like labetalol and carvedilol, cardiac output is maintained with a greater fall in peripheral resistance. - Goodman & Gilman's, 13e
Quick Summary Diagram
AGONISTS ANTAGONISTS
--------- -----------
α1: Phenylephrine α1: Prazosin, Tamsulosin
Midodrine Phentolamine (non-selective)
α2: Clonidine α2: Yohimbine, Mirtazapine
Dexmedetomidine
β1: Dobutamine β1: Metoprolol, Atenolol, Esmolol
β2: Salbutamol, Salmeterol β (non-sel): Propranolol, Timolol
β3: Mirabegron α+β: Labetalol, Carvedilol
Sources: Katzung's Basic and Clinical Pharmacology, 16e | Barash's Clinical Anesthesia, 9e | Goodman & Gilman's Pharmacological Basis of Therapeutics | Rosen's Emergency Medicine
How about the same with cholinergic stimulation
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
I now have comprehensive content from Goodman & Gilman's and Katzung's. Here is the full breakdown:
Cholinergic Receptors - Drugs by Subtype
Cholinergic receptors are activated by acetylcholine (ACh). They divide into two major families based on their pharmacology and structure:
RECEPTOR TYPES AT A GLANCE
| Family | Subtypes | Structure | Location |
|---|---|---|---|
| Muscarinic | M1 - M5 | GPCR (7-TM) | Autonomic effectors, CNS, glands |
| Nicotinic | NM (muscle), NN (neuronal) | Ligand-gated ion channel | NMJ, autonomic ganglia, CNS |
MUSCARINIC RECEPTORS (M1-M5)
Signaling - The Even/Odd Rule
The G-protein coupling follows a clean pattern illustrated below:
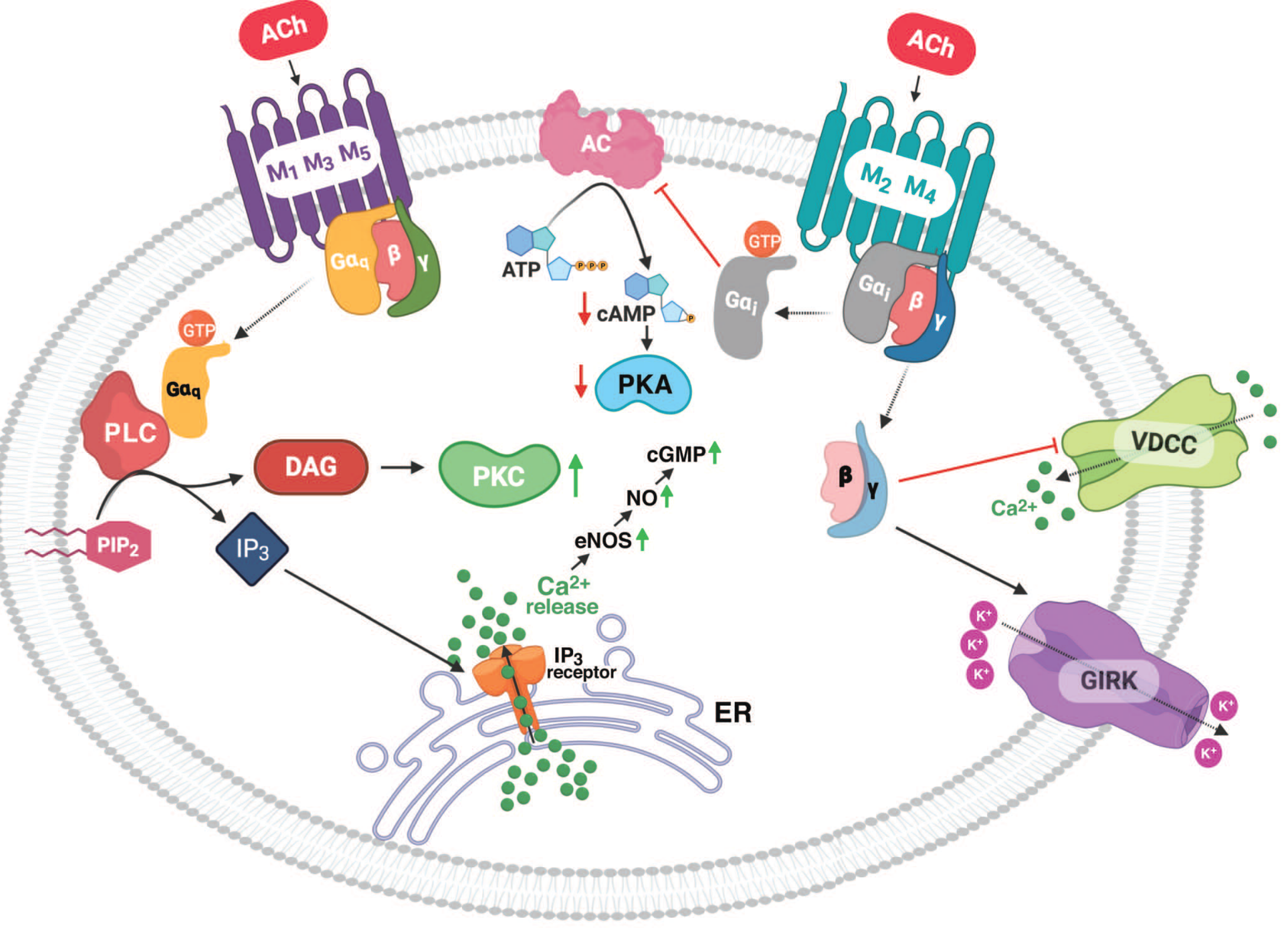
- M1, M3, M5 (odd) → Couple to Gq → PLC → IP3 + DAG → ↑ intracellular Ca²⁺ + PKC activation
- M2, M4 (even) → Couple to Gi → ↓ adenylyl cyclase → ↓ cAMP, open GIRK K⁺ channels, inhibit VDCC
Subtype Locations & Functions
| Subtype | G-protein | Primary Location | Key Effects |
|---|---|---|---|
| M1 | Gq | Gastric parietal cells, autonomic ganglia, CNS (cortex, hippocampus) | ↑ Gastric acid secretion; CNS: memory/cognition |
| M2 | Gi | Heart (SA/AV node), presynaptic nerve terminals | ↓ HR (bradycardia), ↓ AV conduction, inhibits NE/ACh release |
| M3 | Gq | Smooth muscle (bronchi, GI, bladder), exocrine glands, vascular endothelium | Bronchoconstriction, ↑ GI motility, bladder contraction, salivation, vasodilation via NO |
| M4 | Gi | CNS (striatum), presynaptic | Modulates dopamine; presynaptic autoreceptor |
| M5 | Gq | CNS (substantia nigra), cerebral vasculature | Cerebrovascular dilation; reward/addiction pathways |
MUSCARINIC AGONISTS
Direct Agonists (Choline Esters)
| Drug | Selectivity | Key Use | Notes |
|---|---|---|---|
| Acetylcholine (ACh) | All M + N | Intraocular (ophthalmic) | Too rapidly hydrolyzed for systemic use |
| Methacholine | Predominantly M | Bronchoprovocation test (asthma diagnosis) | Resistance to cholinesterase hydrolysis; longer duration |
| Carbachol | M + N | Glaucoma (topical); post-op urinary retention | Resistant to hydrolysis; stimulates both M and N |
| Bethanechol | Predominantly M3 | Urinary retention, post-op ileus | Oral; no nicotinic activity; not hydrolyzed by AChE |
Direct Agonists (Natural Alkaloids)
| Drug | Key Use | Notes |
|---|---|---|
| Pilocarpine | Glaucoma (topical), xerostomia (Sjögren's, post-radiation) | Tertiary amine - crosses BBB; potent miosis and ciliary muscle contraction |
| Muscarine | Toxicology (mushroom poisoning) | Prototype muscarinic agonist; not therapeutic |
| Arecoline | Research only | Active ingredient in betel nut |
| Cevimeline | Xerostomia in Sjögren's syndrome | Selective M1/M3 agonist |
Muscarinic agonists are currently used in treatment of urinary bladder disorders and xerostomia, and in diagnosis of bronchial hyperreactivity (bronchoprovocation test). - Goodman & Gilman's
MUSCARINIC ANTAGONISTS (Antimuscarinics)
Natural Alkaloids
| Drug | Key Uses | Notes |
|---|---|---|
| Atropine | Bradycardia, organophosphate poisoning, pre-op antisialagogue, mydriasis, cycloplegia | Prototype; crosses BBB; tertiary amine |
| Scopolamine | Motion sickness (transdermal patch), pre-op sedation, nausea | Crosses BBB - more CNS effects than atropine (sedation, amnesia) |
Small doses of atropine depress salivary and bronchial secretion and sweating. Larger doses dilate the pupil, impair accommodation, and block the vagus (tachycardia). Even larger doses inhibit GI motility and urinary voiding. - Goodman & Gilman's
Respiratory (Inhaled Antimuscarinics)
| Drug | Duration | Use |
|---|---|---|
| Ipratropium | Short-acting (SAMA) | COPD, acute asthma (add-on) |
| Tiotropium | Long-acting (LAMA) | COPD maintenance (once daily) |
| Aclidinium | Long-acting | COPD |
| Umeclidinium | Long-acting | COPD (often combined with LABA) |
| Glycopyrrolate (inhaled) | Long-acting | COPD |
| Revefenacin | Long-acting | COPD (nebulized) |
Quaternary amines - do NOT cross the blood-brain barrier; minimal systemic effects.
Urological (M3-Selective Antimuscarinics) - for Overactive Bladder
| Drug | Selectivity | Notes |
|---|---|---|
| Oxybutynin | M3 | Available oral/transdermal/intravesical |
| Tolterodine | M2/M3 | Less CNS penetration than oxybutynin |
| Solifenacin | M3-preferring | Once daily |
| Darifenacin | M3-preferring | Least CNS effects |
| Fesoterodine | M2/M3 | Prodrug of active tolterodine metabolite |
| Trospium | Non-selective M | Quaternary - does not cross BBB |
GI Antimuscarinics
| Drug | Use |
|---|---|
| Hyoscine butylbromide (Buscopan) | GI spasm, renal/biliary colic |
| Dicyclomine | IBS, GI spasm |
| Glycopyrrolate (oral/IV) | Excessive drooling, peptic ulcer (rarely) |
CNS / Neurological Antimuscarinics
| Drug | Use |
|---|---|
| Benztropine | Parkinson's disease (tremor, rigidity); antipsychotic-induced EPS |
| Trihexyphenidyl | Parkinson's disease, drug-induced EPS |
| Biperiden | Parkinson's disease, EPS |
Ophthalmic Antimuscarinics (Mydriasis + Cycloplegia)
| Drug | Duration | Use |
|---|---|---|
| Tropicamide | Short (4-6 h) | Fundoscopy/refraction |
| Cyclopentolate | Intermediate | Fundoscopy |
| Homatropine | Intermediate | Uveitis |
| Atropine (topical) | Long (days-weeks) | Penalization therapy for amblyopia |
M1-Selective Antagonist
| Drug | Use |
|---|---|
| Pirenzepine | Peptic ulcer disease (↓ gastric acid via M1 blockade at ganglia); not widely available |
NICOTINIC RECEPTORS
Two distinct subtypes - different locations and drug sensitivities:
| Subtype | Location | Ion Channel | Blocked By |
|---|---|---|---|
| NM (muscle type) | Neuromuscular junction | Na⁺/K⁺ | Curare, rocuronium, vecuronium, succinylcholine |
| NN (neuronal type) | Autonomic ganglia, adrenal medulla, CNS | Na⁺/K⁺ | Hexamethonium, mecamylamine, trimethaphan |
NICOTINIC AGONISTS
NMJ Agonist / Depolarizing Neuromuscular Blocker
| Drug | Mechanism | Use |
|---|---|---|
| Succinylcholine | Binds NM nicotinic receptor, causes persistent depolarization (Phase I block) | Rapid sequence intubation (ultra-short acting - hydrolyzed by plasma cholinesterase) |
| Nicotine | NN + NM agonist | Nicotine replacement therapy (patches, gum, lozenges) for smoking cessation |
| Varenicline | Partial agonist at α4β2 neuronal nicotinic receptor | Smoking cessation |
Succinylcholine consists of two acetylcholine molecules linked through the acetate methyl groups. Like ACh, it stimulates nicotinic receptors at the NMJ - but unlike ACh, it remains bound longer causing persistent depolarization. - Miller's Anesthesia
NICOTINIC ANTAGONISTS
Non-depolarizing NMJ Blockers (NM)
Long-acting:
| Drug | Notes |
|---|---|
| Pancuronium | Vagolytic (↑ HR); mostly renal elimination |
| d-Tubocurarine | Historical prototype; histamine release |
Intermediate-acting:
| Drug | Notes |
|---|---|
| Rocuronium | Fast onset; reversible with sugammadex |
| Vecuronium | Minimal cardiovascular effects |
| Atracurium | Hofmann elimination (organ-independent) |
| Cisatracurium | Cleaner Hofmann elimination; less histamine |
Short-acting:
| Drug | Notes |
|---|---|
| Mivacurium | Hydrolyzed by plasma cholinesterase |
Ganglionic Blockers (NN)
Largely obsolete but pharmacologically important:
| Drug | Use |
|---|---|
| Hexamethonium | Prototype ganglionic blocker (historical) |
| Mecamylamine | Hypertension (historical); investigational for CNS addiction |
| Trimethaphan | Controlled hypotension in surgery (historical) |
INDIRECT CHOLINERGIC AGONISTS (AChE Inhibitors)
These increase ACh at all cholinergic synapses (both M and N receptors) by blocking acetylcholinesterase.
Reversible AChE Inhibitors
| Drug | Clinical Use | Notes |
|---|---|---|
| Neostigmine | Reverse NMJ block post-surgery; myasthenia gravis | Quaternary amine; does not cross BBB; most used in anesthesia |
| Pyridostigmine | Myasthenia gravis (oral maintenance) | Slower onset than neostigmine; preferred for chronic MG |
| Edrophonium | Diagnosis of MG (Tensilon test - historical) | Very short-acting |
| Physostigmine | Reverse central anticholinergic toxicity (atropine OD) | Tertiary - crosses BBB |
| Rivastigmine | Alzheimer's disease, Parkinson's dementia | Brain-selective AChE + BuChE inhibitor |
| Donepezil | Alzheimer's disease | Brain-selective; once daily |
| Galantamine | Alzheimer's disease | Also positive allosteric modulator at nicotinic receptors |
Irreversible AChE Inhibitors (Organophosphates)
| Drug | Use / Context |
|---|---|
| Echothiophate | Glaucoma (historical ophthalmic use) |
| Sarin, soman, VX | Chemical warfare nerve agents |
| Malathion, parathion | Pesticides (toxicology) |
Antidote for organophosphate poisoning: Atropine (blocks M effects) + Pralidoxime (2-PAM) (reactivates AChE before aging)
Summary Table
AGONISTS ANTAGONISTS
--------- -----------
MUSCARINIC:
Direct: Bethanechol (M3) M (non-selective): Atropine, Scopolamine
Pilocarpine M1: Pirenzepine
Methacholine M3 (bladder): Oxybutynin, Solifenacin
Carbachol M3 (lung): Ipratropium, Tiotropium
Indirect (AChEi): CNS M: Benztropine, Trihexyphenidyl
Neostigmine, Pyridostigmine
Donepezil, Rivastigmine
NICOTINIC:
NM: Succinylcholine NM (non-depol): Rocuronium, Vecuronium
NN: Nicotine, Varenicline Atracurium, Pancuronium
NN (ganglionic): Hexamethonium
Sources: Goodman & Gilman's Pharmacological Basis of Therapeutics | Katzung's Basic and Clinical Pharmacology, 16e | Barash's Clinical Anesthesia, 9e | Miller's Anesthesia, 10e | Lippincott Illustrated Reviews: Pharmacology
This is a shared conversation. Sign in to Orris to start your own chat.