Explain about growth hormone from endocrine physiology in detailed explanation with flowcharts
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Growth Hormone - Detailed Endocrine Physiology
Sources: Medical Physiology (Boron & Boulpaep), Costanzo Physiology 7th Ed., Ganong's Review of Medical Physiology 26th Ed.
1. OVERVIEW
Growth hormone (GH), also called somatotropin or somatotropic hormone, is the single most important hormone for normal growth to adult stature. It is a 191-amino acid straight-chain polypeptide with 2 internal disulfide bridges, secreted by somatotrophs scattered throughout the anterior pituitary gland. It is the most abundant anterior pituitary hormone.
GH has profound effects on protein, carbohydrate, and fat metabolism beyond its growth-promoting role. Its gene is located on chromosome 17, part of a family that includes placental variant GH, human chorionic somatomammotropin, and prolactin.
| Hormone | AA | Homology to GH | Gene (Chr 17) |
|---|---|---|---|
| hGH (human GH) | 191 | 100% | Yes |
| pvGH (placental-variant GH) | 191 | 93% | Yes |
| hCS1/hCS2 (chorionic somatomammotropin) | 191 | 84% | Yes |
| hPRL (human prolactin) | 199 | 16% | No (Chr 6) |
2. HYPOTHALAMIC CONTROL - THE AXIS
HYPOTHALAMUS
│
├──► Arcuate nucleus → GHRH (43-aa peptide) ──────────────► (+) GH secretion
│
└──► Periventricular region → Somatostatin (SS-14) ─────► (−) GH secretion
↑ Also: Ghrelin (28-aa peptide from STOMACH) ────────► (+) GH secretion
[via GH secretagogue receptor 1a, GHSR1a]
The primary regulation of GH secretion is stimulatory - sectioning the pituitary stalk lowers GH secretion, confirming the net drive is excitatory (GHRH > SS).
GHRH Mechanism (at somatotrophs)
GHRH → GHRHR (GPCR) → Gαs → Adenylyl cyclase → ↑ cAMP
│
↓ ▼
↑ [Ca²⁺]i PKA activation
│ │
└────────┴──► GH SYNTHESIS + RELEASE
Somatostatin Mechanism (at somatotrophs)
SS → SS receptor (GPCR) → Gαi → ↓ Adenylyl cyclase → ↓ cAMP
│
↓ [Ca²⁺]i
│
↓ GH RELEASE (inhibited)
3. HYPOTHALAMIC-PITUITARY-TARGET TISSUE DIAGRAM
(From Medical Physiology, Fig. 48-3)
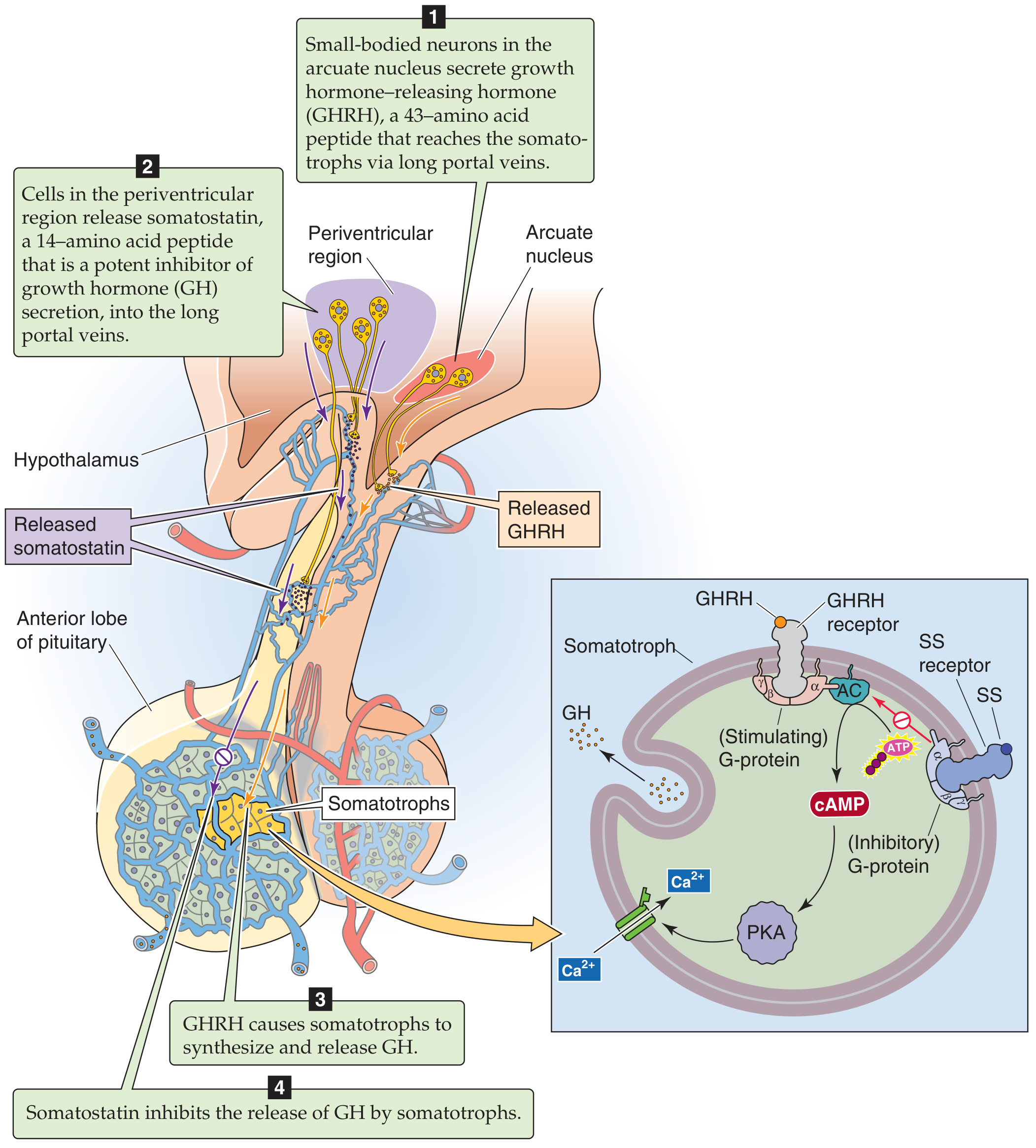
The arcuate nucleus releases GHRH; the periventricular region releases somatostatin (SS). GHRH raises cAMP and Ca²+ in somatotrophs to release GH; SS inhibits adenylyl cyclase and lowers Ca²+ to block GH release.
4. PULSATILE SECRETION AND DIURNAL VARIATION
GH is secreted in a pulsatile pattern, with bursts occurring approximately every 2 hours. The pattern across a 24-hour cycle is shown below:
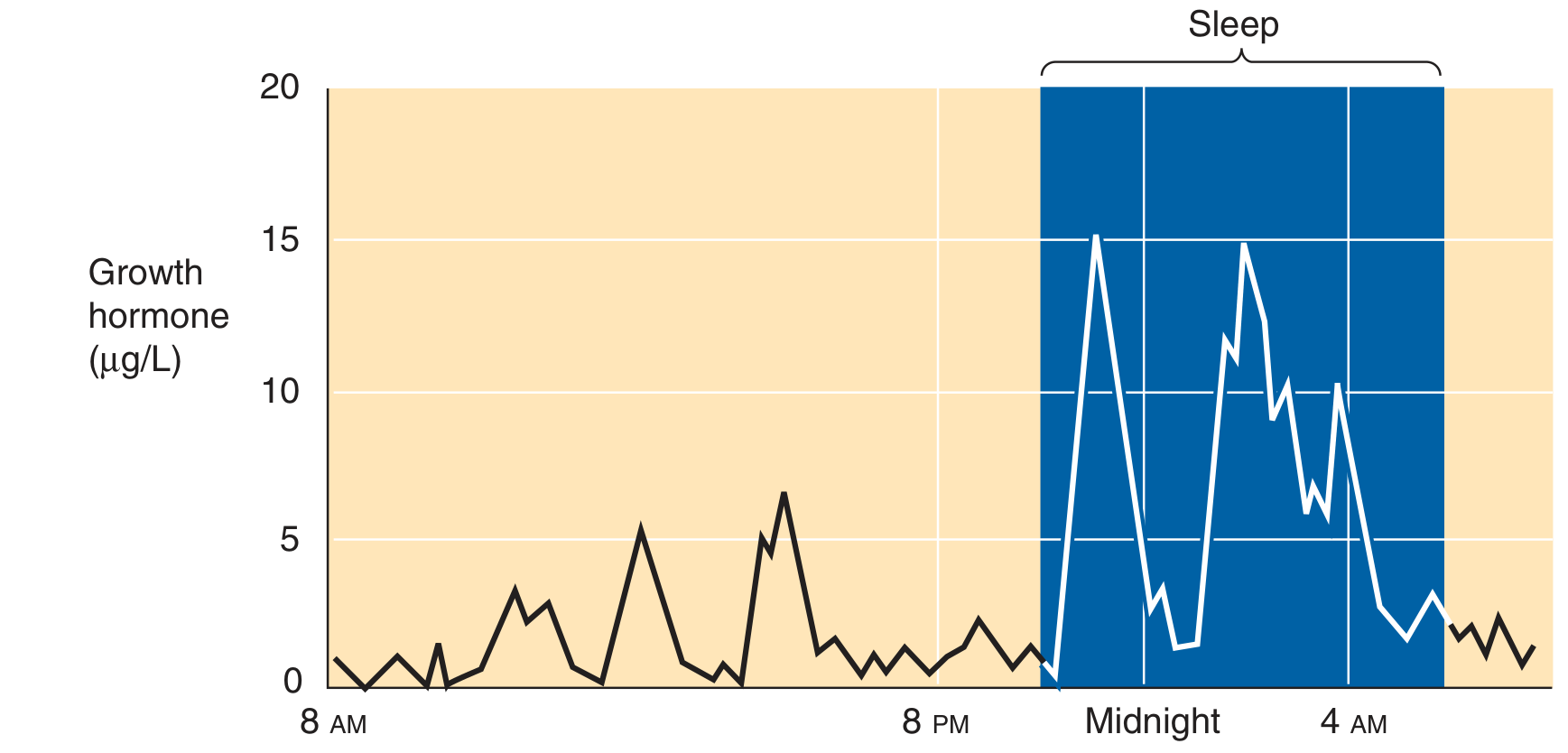
Key point: The largest secretory burst occurs within 1 hour of falling asleep, during slow-wave sleep (stages III and IV). Over 70% of total daily GH secretion occurs during these nocturnal pulses. The pattern depends on sleep-wake cycles, not light-dark cycles.
Lifecycle Pattern of GH Secretion
Birth ──► Childhood (stable) ──► Puberty (massive surge) ──► Adulthood (stable, lower) ──► Senescence (lowest)
↑
Estrogen (females) / Testosterone (males)
increase frequency + magnitude of pulses
→ GROWTH SPURT of puberty
5. FACTORS AFFECTING GH SECRETION
| Stimulatory | Inhibitory |
|---|---|
| Hypoglycemia / fasting / starvation | Hyperglycemia (glucose infusion) |
| Exercise | Elevated free fatty acids (FFA) |
| Stress (trauma, fever, anesthesia, psychological) | Cortisol |
| Slow-wave sleep (stages III & IV) | REM sleep |
| Arginine and certain amino acids / protein meal | Obesity |
| Estrogens and androgens (puberty) | Somatostatin |
| L-dopa, alpha-adrenergic agonists | GH itself (short-loop feedback) |
| Dopamine receptor agonists (apomorphine) | IGF-1 (long-loop feedback) |
| Ghrelin | Medroxyprogesterone |
| Thyroid hormones | Senescence |
| Glucagon | Beta-adrenergic agonists |
6. FEEDBACK CONTROL LOOPS
Feedback Flowchart
(From Ganong's, Fig. 18-3)
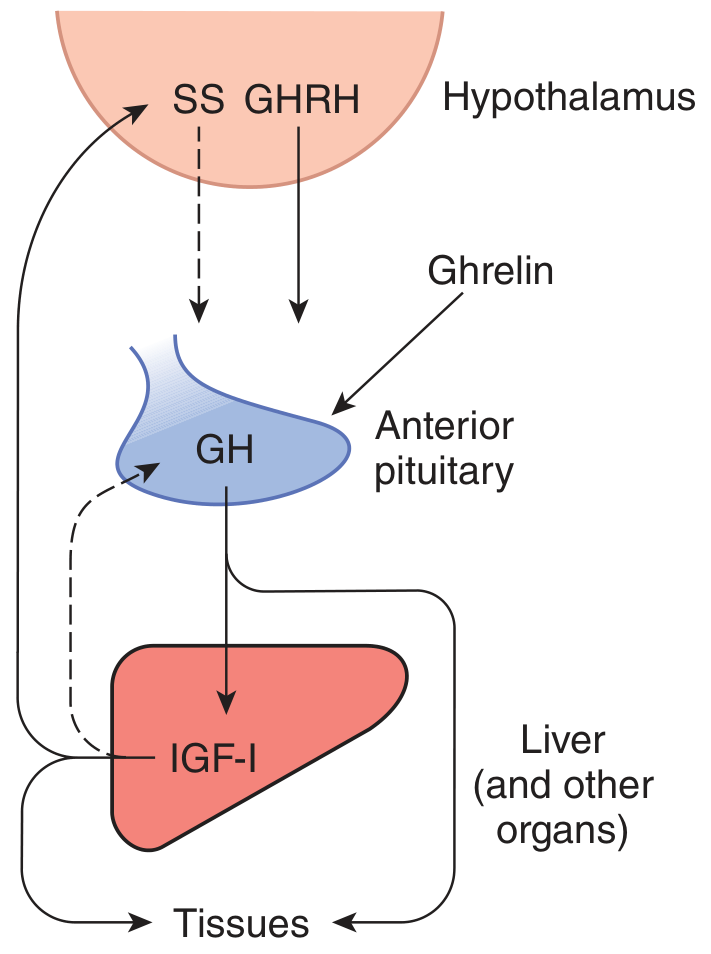
GH secretion ──► ↑ Circulating GH
│
┌─────────────┴──────────────────────┐
│ │
Direct SHORT LOOP: Stimulates LIVER
GH → antagonizes GHRH → produces IGF-1
release from hypothalamus │
LONG LOOP with IGF-1:
1) IGF-1 directly inhibits somatotroph
2) IGF-1 suppresses GHRH release
3) IGF-1 stimulates SS secretion
→ ALL THREE ↓ GH secretion
7. GH RECEPTOR AND SIGNAL TRANSDUCTION
The GH receptor belongs to the cytokine receptor superfamily (NOT a GPCR for target tissue effects). It has:
- Large extracellular domain
- Single transmembrane domain
- Large intracellular domain associated with JAK2 kinase
Receptor Activation
One GH molecule has TWO receptor-binding domains:
GH binds first receptor ──► second receptor recruited ──► HOMODIMERIZATION
│
Essential for activation
JAK2-STAT Signaling (Primary Pathway)
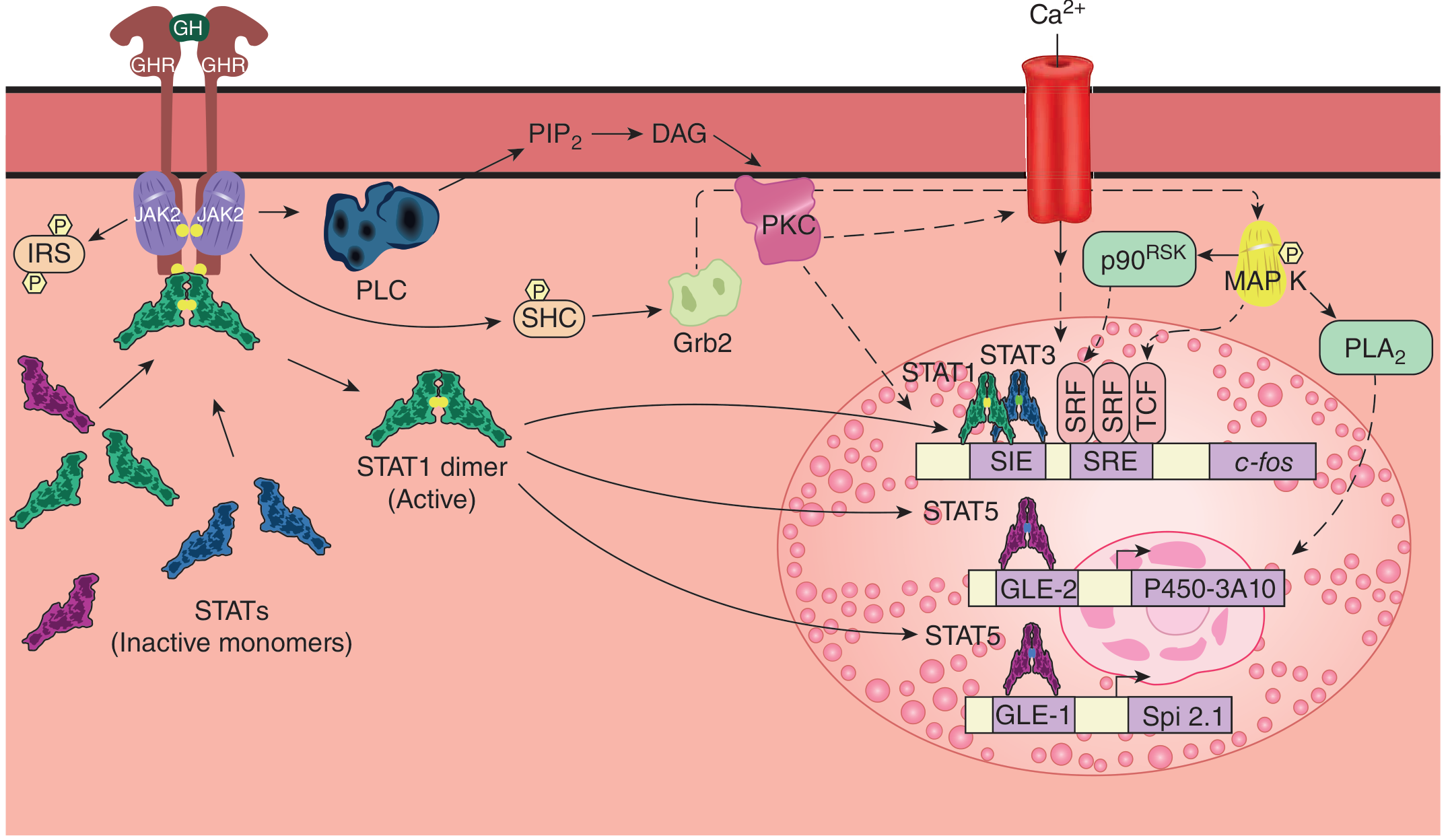
GH–GHR dimer
│
▼
JAK2 transphosphorylation (tyrosine kinase activation)
│
┌──┴──────────────────────────────────────────────┐
│ │
STATs (inactive monomers) phosphorylated IRS-1/IRS-2 phosphorylated
→ STAT1 dimer → SIE element → gene transcription → Insulin-like metabolic effects
→ STAT5 → GLE-1/GLE-2 elements
→ c-fos via SRE/SRF/TCF Also: PLC → DAG → PKC
Ca²+ channels open
MAP kinase activated
PLA₂ activated
8. ACTIONS OF GROWTH HORMONE
GH exerts effects through two mechanisms:
- Direct effects on target cells via GH receptor (JAK2-STAT)
- Indirect effects via IGF-1 (somatomedin C) produced mainly by the liver
Complete Actions Flowchart
GROWTH HORMONE
│
┌──────────────┴──────────────────┐
DIRECT EFFECTS INDIRECT (via IGF-1)
│ │
┌──────┼──────────┐ ┌──────────┴──────────┐
│ │ │ BONE GROWTH SOFT TISSUE GROWTH
▼ ▼ ▼ │ │
MUSCLE FAT LIVER Chondrocytes DNA/RNA/protein
│ │ │ proliferate synthesis in
↓Glucose ↑Lipolysis ↑Gluco- Epiphyseal plates all organs
uptake ↑FFA neogenesis widen → linear ↑ lean body mass
(insulin →↑BG ↑BG growth (+before ↑ organ size
resistance) puberty closure)
Metabolic Effects Summary
| Tissue | GH Effect |
|---|---|
| Muscle | ↓ Glucose uptake (insulin resistance) |
| Adipose tissue | ↑ Lipolysis → ↑ free fatty acids |
| Liver | ↑ Gluconeogenesis, ↑ IGF-1 production |
| Muscle + Fat + Liver | Insulin resistance → ↑ blood glucose ("diabetogenic effect") |
| All organs | ↑ Amino acid uptake, ↑ DNA/RNA/protein synthesis |
| Bone (pre-closure) | ↑ Linear growth via IGF-1 on chondrocytes |
| Bone (post-closure) | Periosteal thickening, no longitudinal growth |
Protein/Electrolyte Effects:
- Positive nitrogen and phosphorus balance
- ↓ Blood urea nitrogen and plasma amino acids (taken up for synthesis)
- ↑ Gastrointestinal Ca²+ absorption
- ↓ Na+ and K+ excretion (diverted to growing tissues)
- ↑ Plasma phosphorus
- ↑ Urinary excretion of 4-hydroxyproline (marker of collagen turnover in growth)
9. IGF-1 (SOMATOMEDIN C) - The Key Mediator
GH → acts on LIVER (primarily) and other tissues (kidney, muscle, cartilage, bone)
│
▼
IGF-1 PRODUCED
│
┌────────────┼───────────────────────┐
│ │ │
Binds IGF-1 Binds to Circulates
receptor IGFBPs (6 types) bound to IGFBP-3
(similar to → prolongs half-life (90% of circulating IGF-1)
insulin R, → modulates activity
tyrosine
kinase)
│
▼
EFFECTS:
- Linear bone growth (chondrocyte proliferation and differentiation)
- ↑ DNA, RNA, protein synthesis in virtually all tissues
- Insulin-like metabolic effects at high concentrations
(can cause hypoglycemia)
- FEEDBACK: inhibits GH secretion (long loop)
IGF-1 vs IGF-2:
- IGF-1: GH-dependent, mirrors GH secretion, mainly post-natal growth
- IGF-2: Less GH-dependent, important for fetal growth
- Both structurally similar to proinsulin, with A, B, C domains + unique D domain (C peptide NOT cleaved, unlike insulin)
10. COMPLETE REGULATORY FLOWCHART
╔═══════════════════════════════════════════════════════════════╗
║ HYPOTHALAMUS ║
║ Arcuate nucleus → GHRH (+) Periventricular → SS (−) ║
╚══════════════╤════════════════════════════════╤══════════════╝
│ Portal veins │ Portal veins
▼ ▼
╔═══════════════════════════════════════════════════════════════╗
║ ANTERIOR PITUITARY (Somatotrophs) ║
║ GHRH → cAMP ↑ → PKA → Ca²+ ↑ → GH release ║
║ SS → cAMP ↓ → Ca²+ ↓ → GH release inhibited ║
║ Ghrelin (stomach) → GHSR1a → GH release (+) ║
╚══════════════════════════╤════════════════════════════════════╝
│
GH released
│
┌────────────────┼─────────────────────────────┐
▼ ▼ ▼
SHORT-LOOP TARGET TISSUES LIVER + others
FEEDBACK (direct effects) → IGF-1 produced
GH → ↓GHRH muscle/fat/liver/bone │
(insulin resistance, LONG-LOOP FEEDBACK:
lipolysis, gluconeogenesis) IGF-1 → ↑ SS
JAK2-STAT signaling IGF-1 → ↓ GHRH
IGF-1 → direct ↓ pituitary
11. PATHOPHYSIOLOGY
GH Deficiency
Deficiency BEFORE puberty:
→ Pituitary dwarfism (growth failure, short stature)
→ Mild obesity, delayed puberty
→ Normal size at birth (GH not needed for fetal growth)
Deficiency AFTER puberty:
→ No major clinical illness
→ ↓ Lean body mass, ↑ body fat
→ Reduced sense of well-being
→ Treatment with recombinant GH restores lean mass, reduces fat
Laron Dwarfism (GH resistance):
- GH levels are ELEVATED (normal pituitary)
- GH receptors are defective
- IGF-1 cannot be produced
- Treatment with GH is ineffective - must use recombinant IGF-1
Causes of GH deficiency (by level):
Hypothalamus → ↓ GHRH secretion
Pituitary → Primary ↓ GH production
Liver → Failure to generate IGF-1
Receptor → GH receptor defect (Laron) or IGF-1 receptor defect
GH Excess
Before puberty (epiphyses OPEN):
→ GIGANTISM
→ Extraordinary height (Tom Thumb's inverse: Alton giant >2.7 m)
→ Linear + soft tissue growth
After puberty (epiphyses CLOSED):
→ ACROMEGALY
→ No increase in height (no linear growth)
→ Periosteal thickening: hands, feet, jaw, brow, skull
→ Soft tissue swelling, hirsutism
→ Enlarged viscera (heart, liver, spleen, GI tract)
→ Hypertension, joint deformity, pulmonary insufficiency, heart failure
→ Insulin resistance / secondary diabetes mellitus
→ 20-40% have concurrent hyperprolactinemia (mixed adenomas)
→ Most common cause: GH-secreting pituitary adenoma
12. CLINICAL CORRELATIONS
| Condition | Mechanism | Features |
|---|---|---|
| Gigantism | GH excess before epiphyseal closure | Height >2 m, proportionate growth |
| Acromegaly | GH excess after epiphyseal closure | Enlarged acral parts, viscera, CV disease |
| Pituitary dwarfism | GH deficiency in childhood | Short stature, normal proportions |
| Laron dwarfism | GH receptor defect | High GH, low IGF-1, does NOT respond to GH |
| GH deficiency (adult) | Tumor/surgery/radiation | Low lean mass, high fat, fatigue |
| Pharmacological use | Recombinant GH therapy | Pediatric GH deficiency, adult GH deficiency, Turner syndrome, PWS |
Key Points to Remember
- GH is a 191-aa polypeptide from somatotrophs of anterior pituitary
- Regulated by GHRH (+), SS (−), Ghrelin (+) from hypothalamus/stomach
- Secreted in pulses - largest burst in stage III/IV sleep; >70% secreted nocturnally
- Acts via JAK2-STAT pathway (cytokine receptor superfamily, homodimerization required)
- Direct effects: diabetogenic (↑ blood glucose via insulin resistance, lipolysis, gluconeogenesis)
- Indirect effects via IGF-1: anabolic, promotes linear growth via chondrocyte proliferation
- Feedback: short loop (GH → ↓GHRH), long loop (IGF-1 → ↑SS, ↓GHRH, direct pituitary inhibition)
- Deficiency before puberty → dwarfism; excess before puberty → gigantism; excess after puberty → acromegaly
- Laron dwarfism = GH receptor defect → high GH, low IGF-1, GH treatment ineffective
- GH peak secretion is at puberty (estrogen in females, testosterone in males)
- Costanzo Physiology 7th Ed., pp. 415-418 | Medical Physiology (Boron & Boulpaep), pp. 1458-1465 | Ganong's Review of Medical Physiology 26th Ed., pp. 329-332
This is a shared conversation. Sign in to Orris to start your own chat.