Explain most common cardiac emergency conditions with ecg images
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the ECG images and clinical content needed for a comprehensive response. Let me compose the full answer.
Common Cardiac Emergency Conditions with ECG Findings
Sources: Tintinalli's Emergency Medicine, Rosen's Emergency Medicine, Frameworks for Internal Medicine, Braunwald's Heart Disease
1. ST-Elevation Myocardial Infarction (STEMI)
STEMI results from complete occlusion of a coronary artery causing transmural ischemia. It is the most time-critical cardiac emergency - "door-to-balloon" time must be under 90 minutes.
ECG criteria for STEMI diagnosis:
- New ST-segment elevation at the J point in 2 or more contiguous leads
- ≥0.1 mV in all leads except V2-V3
- ≥0.2 mV in V2-V3 in men ≥40 years; ≥0.25 mV in men <40 years; ≥0.15 mV in women
- Reciprocal ST depression in mirror leads
- Pathological Q waves develop over hours
Evolution of ECG changes over time:
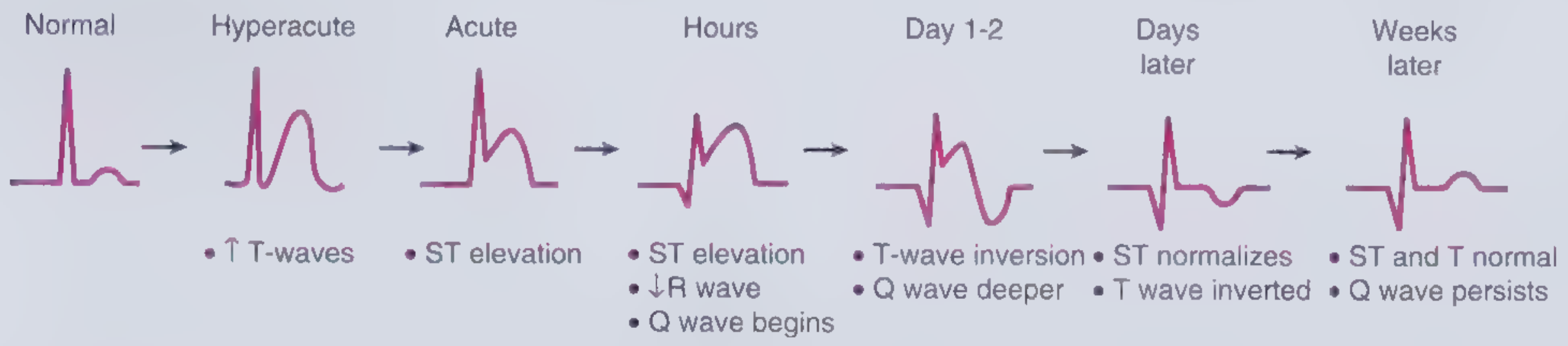
The earliest sign is hyperacute (tall, broad, symmetric) T-waves, followed by ST elevation, Q-wave development, T-wave inversion, and eventually normalization of ST with persistent Q waves.
Treatment: Immediate reperfusion via primary PCI (preferred) or fibrinolytics. Aspirin, heparin, P2Y12 inhibitors.
2. UA/NSTEMI (Non-ST-Elevation ACS)
Partial coronary occlusion or severe ischemia without full transmural involvement. Distinguished from STEMI by the absence of ST elevation, and from UA by troponin rise.
ECG findings:
- New horizontal or downsloping ST depression ≥0.05 mV in 2 contiguous leads
- T-wave inversion ≥0.1 mV with prominent R wave
- May be entirely normal at presentation
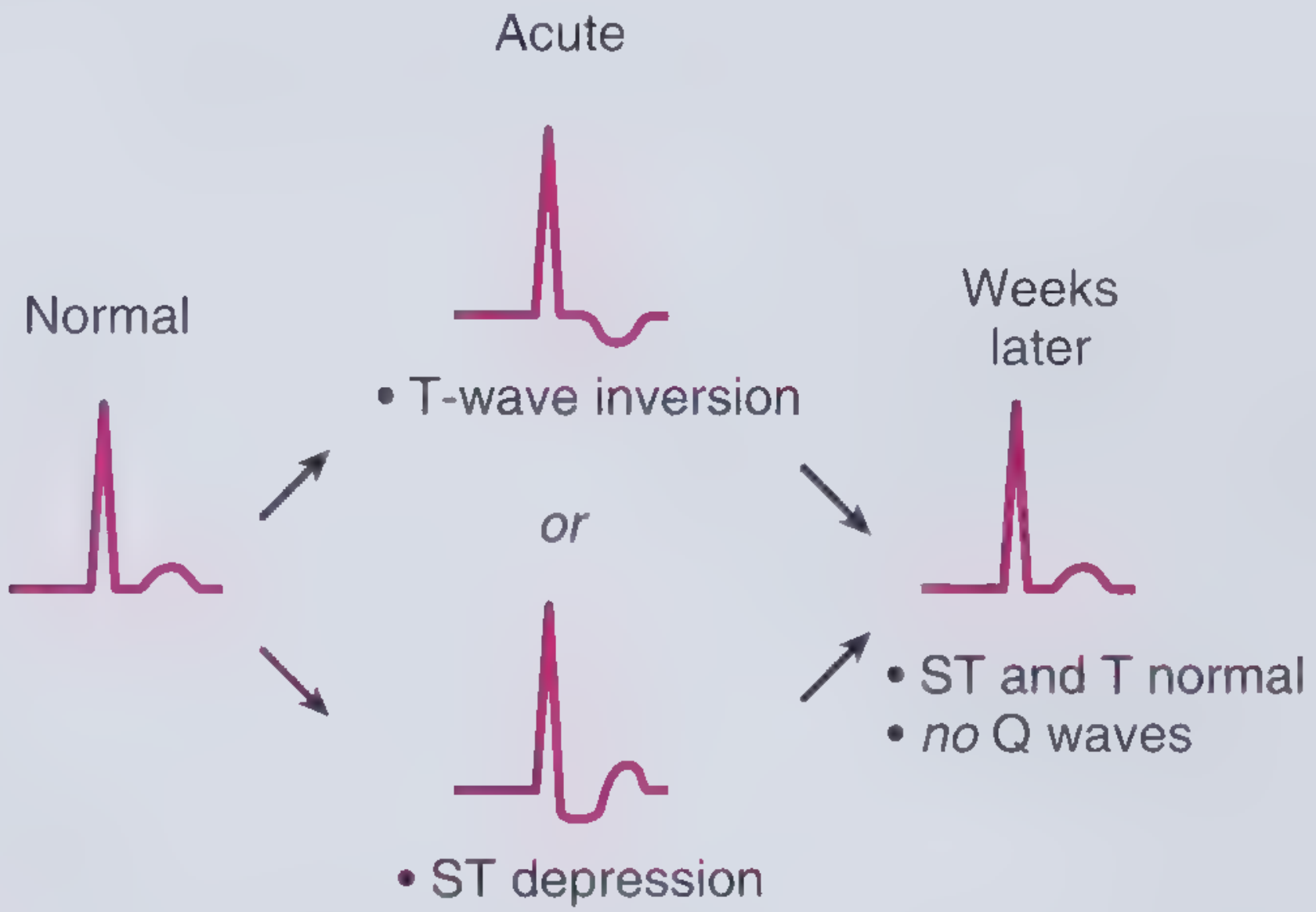
Unlike STEMI, no Q waves form and the ST/T changes normalize without permanent injury markers.
Treatment: Anticoagulation, dual antiplatelet therapy, risk stratification with TIMI/GRACE score, early invasive strategy if high-risk.
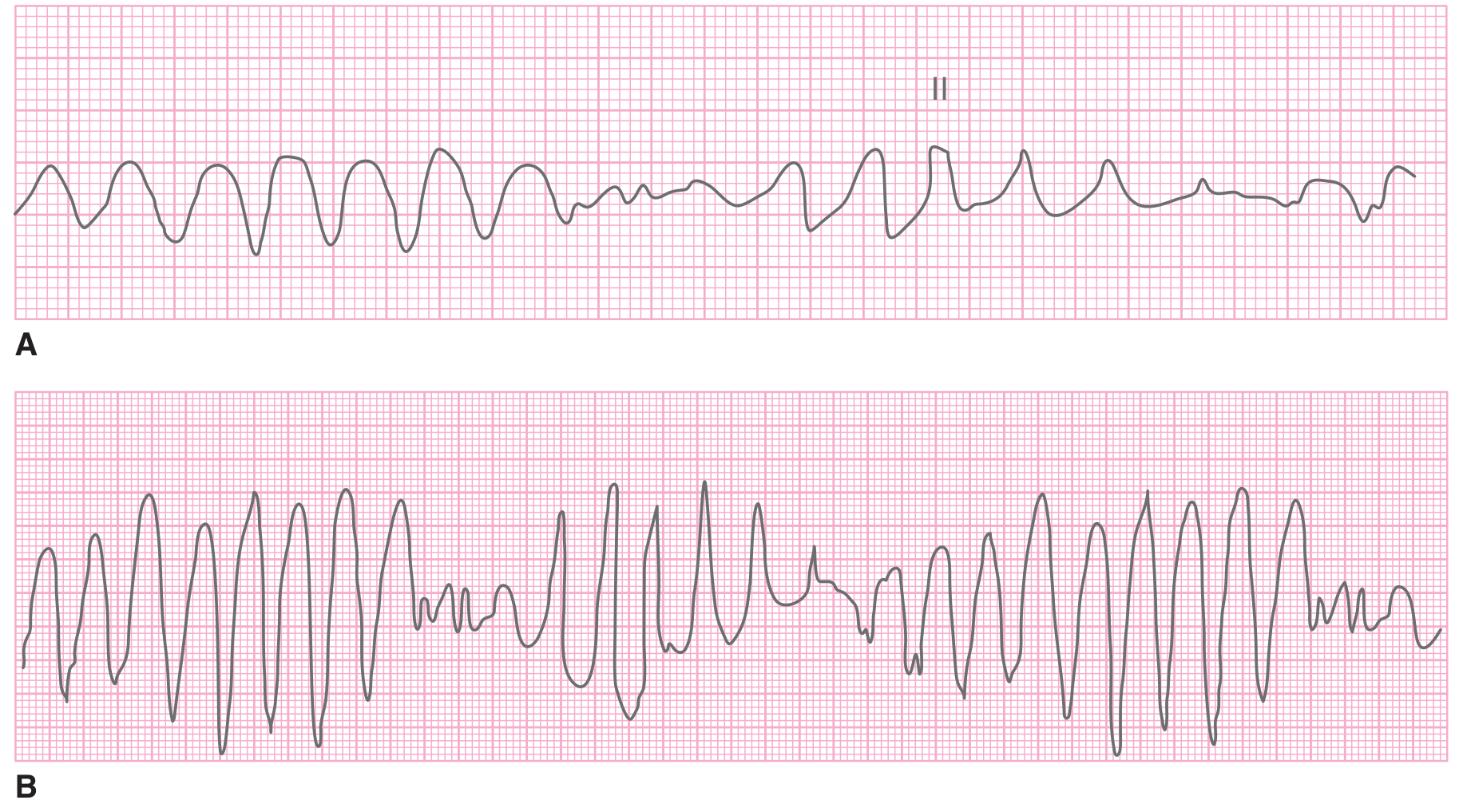
3. Ventricular Fibrillation (VF)
VF is disorganized, chaotic depolarization of ventricular myocardium with no effective cardiac output. It is the most common initial rhythm in sudden cardiac death.
ECG findings:
- No discernible P waves, QRS complexes, or T waves
- Completely chaotic, irregular baseline
- Can appear fine (low amplitude), coarse, or intermediate
- Coarse VF can mimic VT (see panel C below)
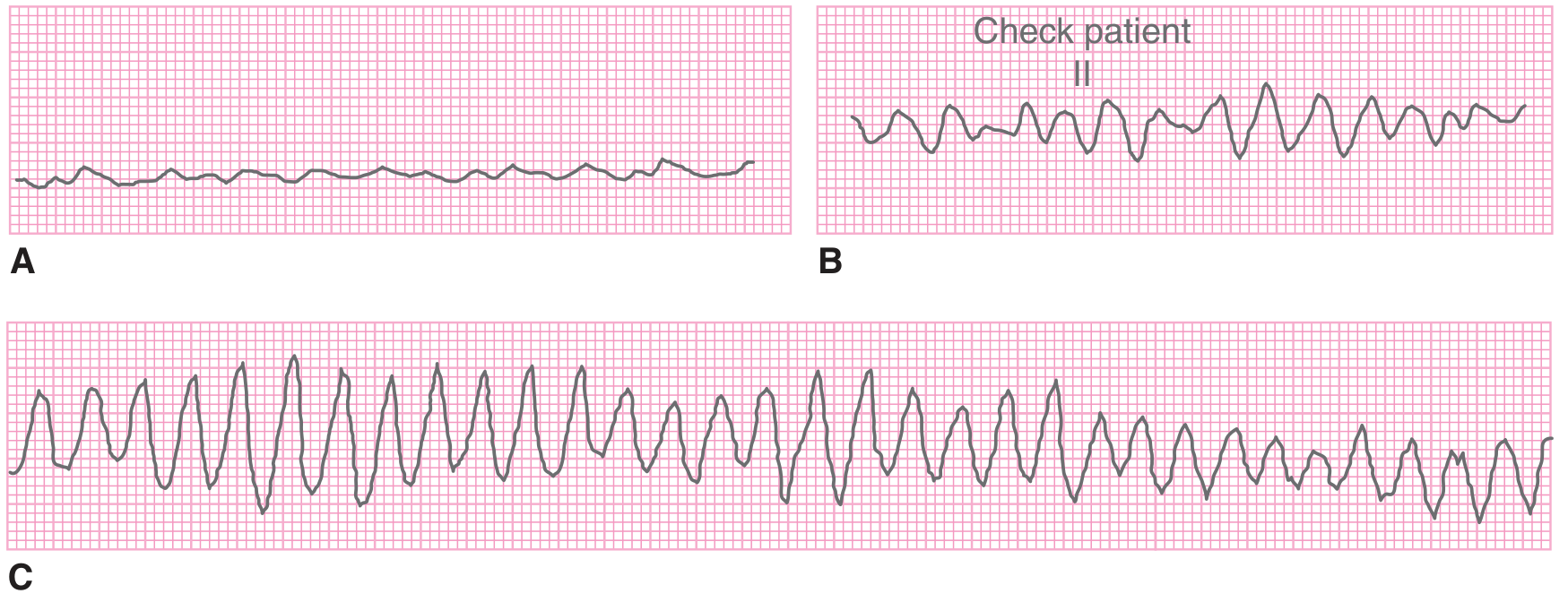
Fine VF (A) is a near-flat chaotic line with no organized deflections. Coarse VF (B, C) has larger oscillations and must be distinguished from pulseless VT - check for a pulse.
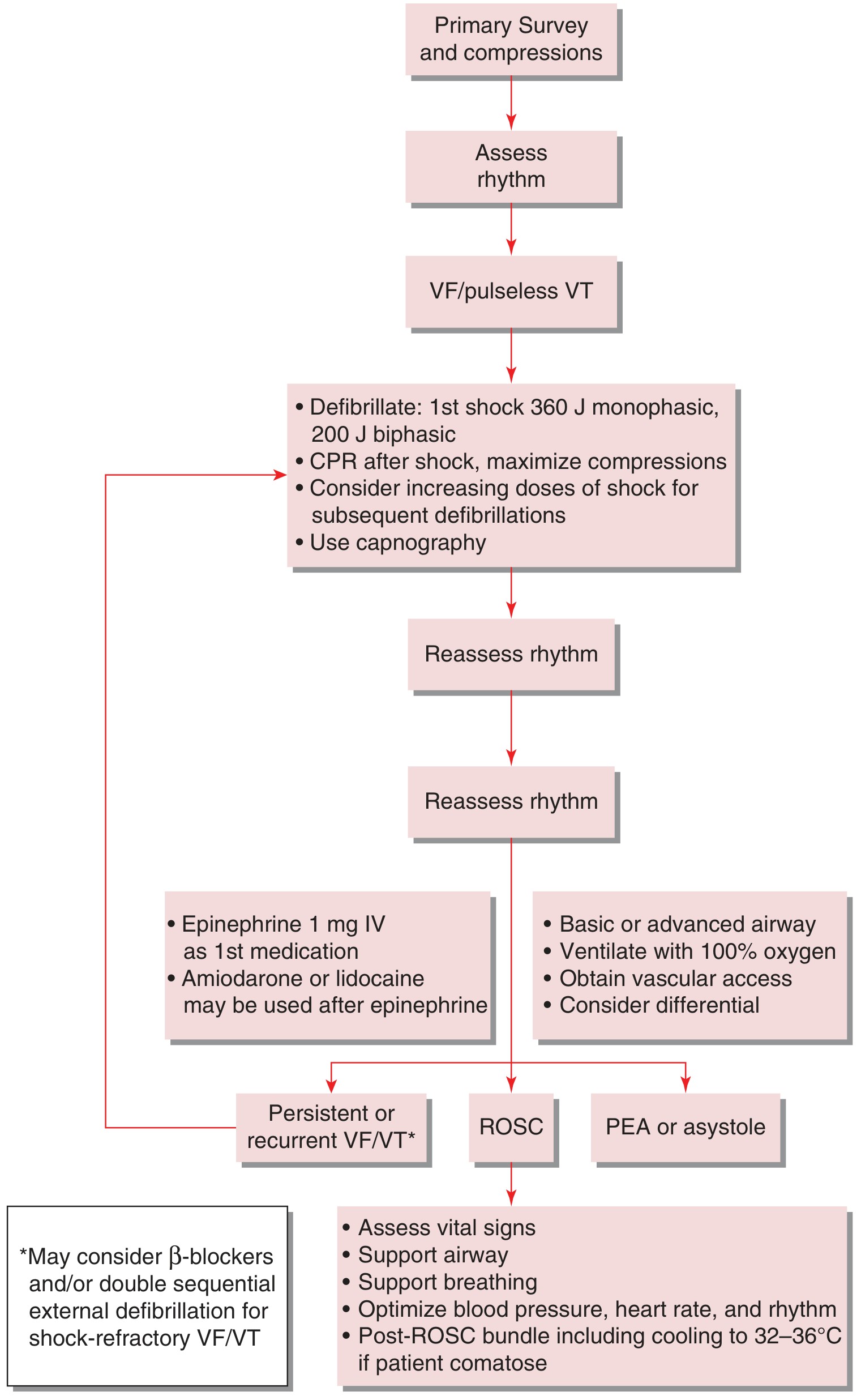
Treatment: Immediate defibrillation (200 J biphasic, 360 J monophasic), CPR, epinephrine 1 mg IV, amiodarone or lidocaine. See management algorithm below:
4. Ventricular Tachycardia (VT)
VT is 3 or more consecutive ventricular depolarizations at a rate >100 beats/min. It accounts for ~50% of cases in patients with ischemic heart disease. VT cannot be reliably distinguished from SVT by symptoms alone - use the ECG.
ECG findings - Monomorphic VT:
- Rate 140-180 bpm (range 120-300)
- Wide QRS >100-120 ms with consistent beat-to-beat morphology
- No associated P waves (occasional dissociated P wave visible)
- Rapid, regular rhythm
ECG findings - Polymorphic VT / Torsades de Pointes:
- Wide QRS with constantly changing morphology and direction
- Torsades: characteristic "twisting of points" pattern with rotating QRS axis
- Associated with prolonged QT interval (congenital or acquired - drugs, electrolyte derangements)
Wide-complex tachycardia differential (ventricular vs. supraventricular sources):
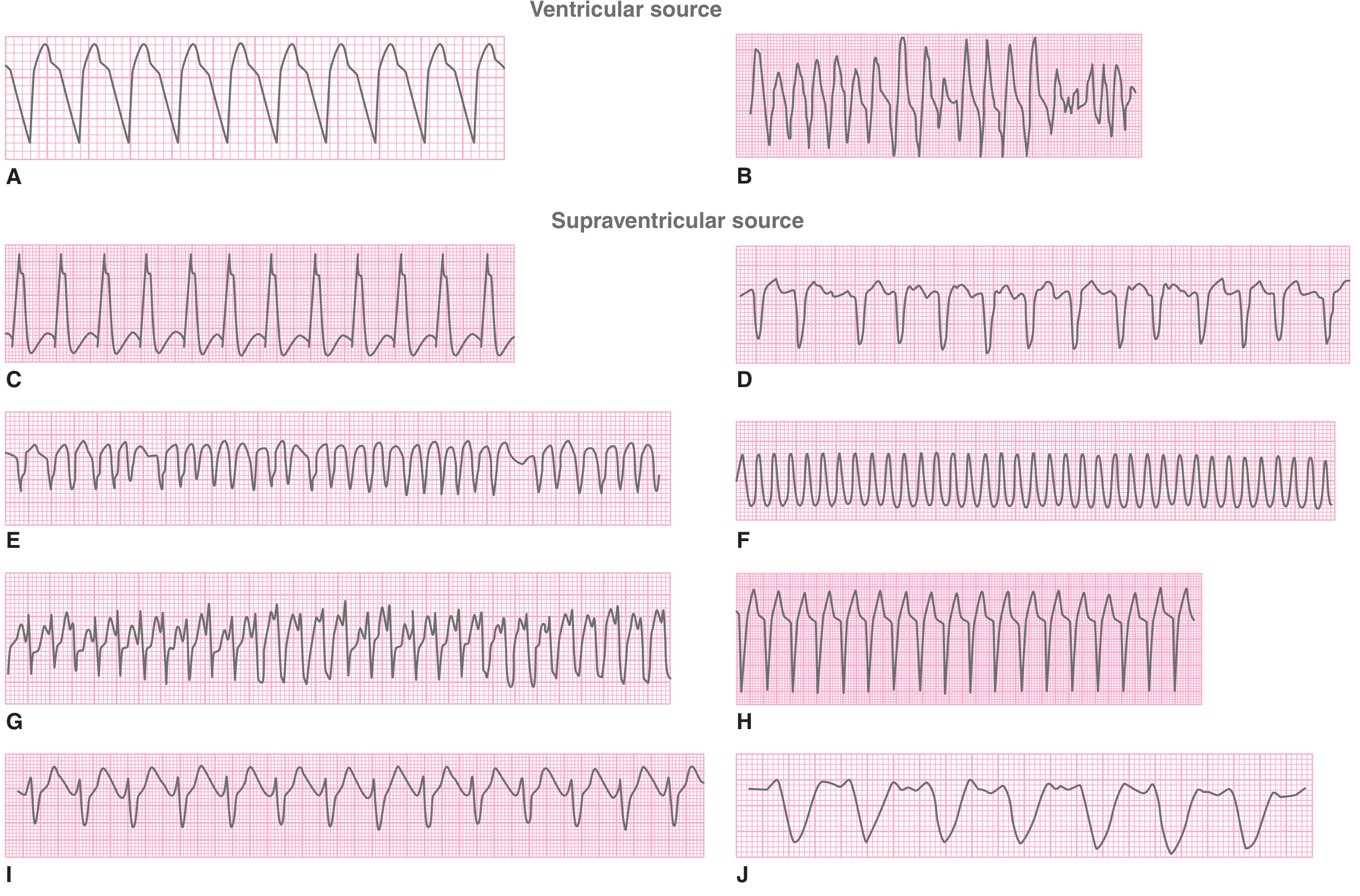
Key rule: assume all wide-complex tachycardias are VT until proven otherwise, especially in hemodynamically unstable patients.
Treatment:
- Unstable (pulseless): defibrillation + CPR (same as VF protocol)
- Unstable (with pulse): immediate synchronized cardioversion + sedation
- Stable: IV procainamide, amiodarone, or lidocaine; avoid verapamil/adenosine unless SVT confirmed
5. Atrial Fibrillation (AF)
AF is the most common sustained arrhythmia after sinus tachycardia. Multiple discharging atrial foci cause chaotic atrial activity with no coordinated contraction, reducing cardiac output and increasing thromboembolic risk.
ECG findings:
- Absent P waves - replaced by chaotic/fibrillatory baseline (best seen in V1)
- Irregularly irregular ventricular rhythm (the hallmark)
- Narrow QRS complexes (unless bundle branch block or WPW)
- Ventricular rate typically 120-170 bpm if AV node unmedicated
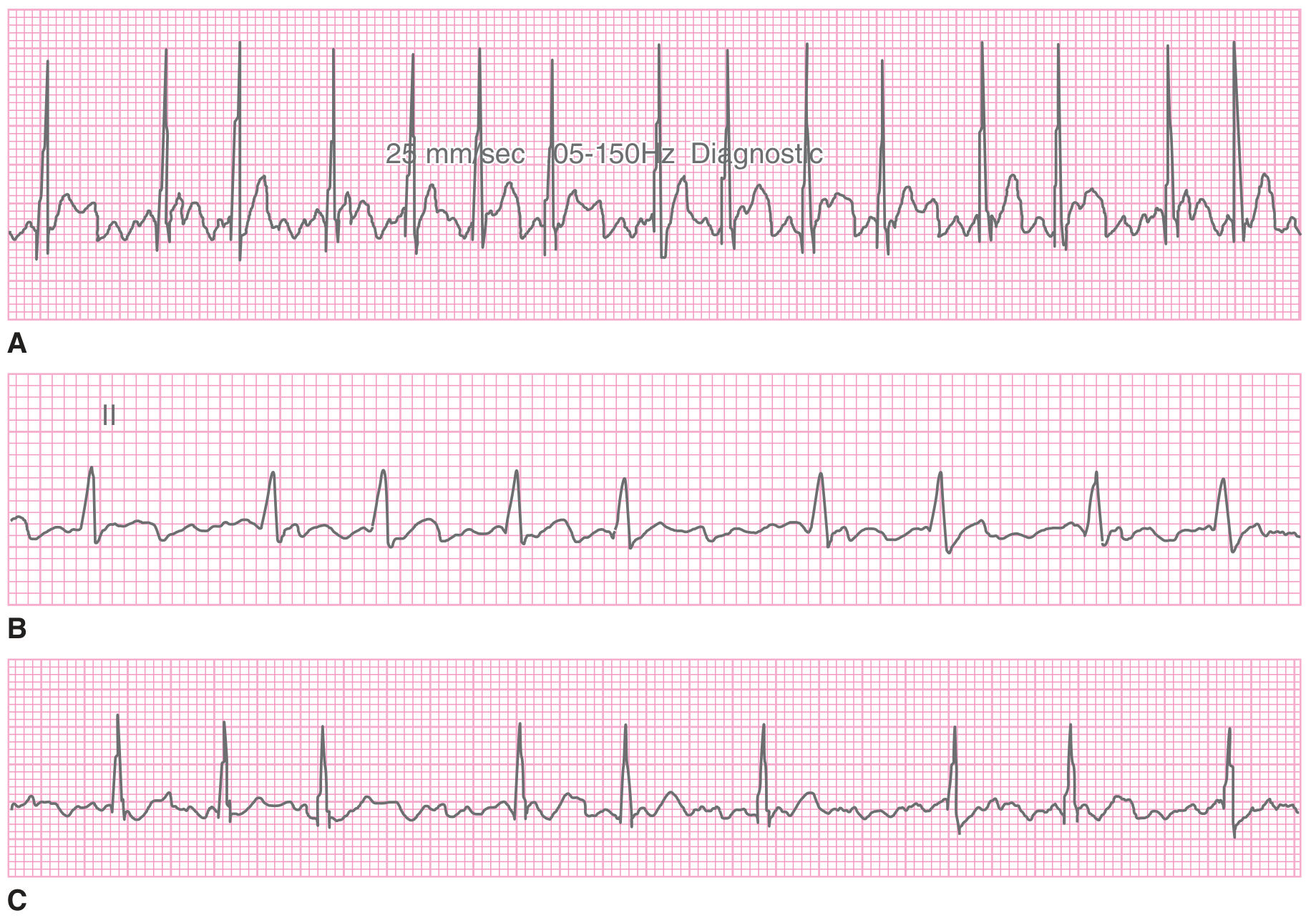
Note the completely irregular R-R intervals and absence of any discernible P waves in all three examples (A, B, C).
Treatment:
- Hemodynamically unstable: immediate DC cardioversion (150-200 J)
- Stable: rate control (IV diltiazem or metoprolol, target HR <100 bpm) OR rhythm conversion
- Anticoagulation: based on CHA₂DS₂-VASc score to prevent stroke
6. Complete (Third-Degree) AV Block
All atrial impulses are blocked from reaching the ventricles. A slow escape pacemaker (junctional or ventricular) takes over, often inadequate to maintain cardiac output.
ECG findings:
- P waves and QRS complexes are completely dissociated (no fixed PR relationship)
- Atrial rate is faster than ventricular rate
- Narrow QRS if junctional escape (40-60 bpm); wide QRS if ventricular escape (<40 bpm)
- QRS rate is regular but slow
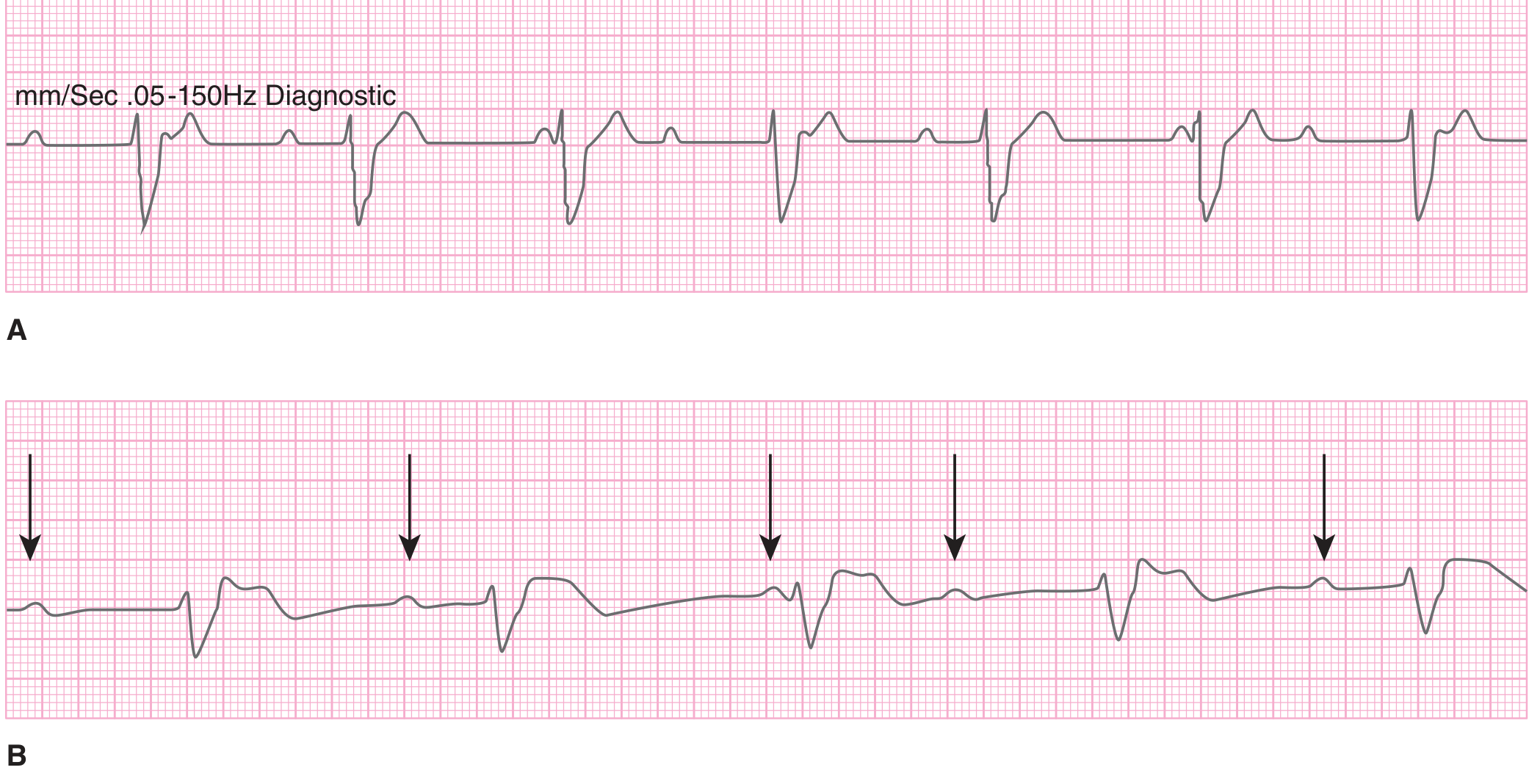
In both examples, atrial rate = 83 bpm, ventricular escape rate = 50 bpm. P waves are completely dissociated from QRS complexes; some P waves are buried in QRS or T waves.
Clinical context: Occurs in up to 8% of inferior MI patients (nodal block, usually reversible). Infranodal complete block from anterior MI carries high mortality even with pacing.
Treatment: Transcutaneous pacing immediately; atropine may help nodal block but not infranodal. Transvenous pacing is definitive.
7. Second-Degree AV Block - Mobitz Type I (Wenckebach)
Progressive PR prolongation until a P wave is completely blocked (dropped QRS), then the cycle resets.
ECG findings:
- Progressive PR lengthening from beat to beat
- Dropped QRS after longest PR
- Group beating pattern
- Usually narrow QRS

Treatment: Usually self-limited. Atropine if hemodynamically compromised. Associated with inferior MI, digoxin toxicity, or myocarditis.
8. First-Degree AV Block
Every atrial impulse conducts but is delayed. Alone it is not an emergency, but in the context of acute MI or drug toxicity it warrants close monitoring as it may progress.
ECG findings:
- PR interval consistently >200 ms
- Every P wave followed by a QRS
- Otherwise normal-appearing rhythm
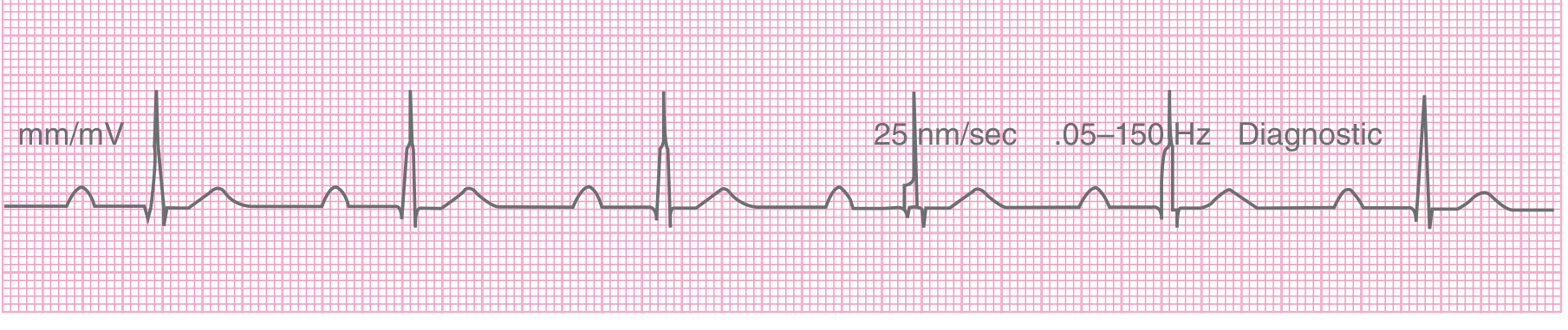
(Image: Sinus rhythm with PR interval 300 ms - well above the normal upper limit of 200 ms)
Quick Reference Summary
| Condition | Key ECG Finding | Rate | Rhythm | Emergency Action |
|---|---|---|---|---|
| STEMI | ST elevation ≥0.1 mV in 2+ contiguous leads | Variable | Regular | PCI within 90 min |
| NSTEMI/UA | ST depression, T-wave inversion, or normal | Variable | Regular | Anticoagulate, risk stratify |
| VF | Chaotic, no QRS | >300 | Totally irregular | Defibrillate immediately |
| Monomorphic VT | Wide QRS, consistent morphology | 140-180 | Regular | Cardiovert if unstable; antiarrhythmics if stable |
| Torsades/Polymorphic VT | Wide, twisting QRS axis | 140-300 | Irregular | Magnesium sulfate; correct QT; defibrillate if pulseless |
| Atrial Fibrillation | No P waves, irregularly irregular | 120-170 (ventricular) | Irregularly irregular | Rate or rhythm control; anticoagulation |
| Complete Heart Block | P-QRS dissociation, slow escape | <40-60 | Regular (slow) | Transcutaneous pacing immediately |
| Wenckebach | Progressive PR prolongation, dropped QRS | Normal-slow | Regularly irregular | Atropine if symptomatic |
Sources: Tintinalli's Emergency Medicine (9e), Rosen's Emergency Medicine, Frameworks for Internal Medicine, Braunwald's Heart Disease (12e)
This is a shared conversation. Sign in to Orris to start your own chat.