anti d injecton
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Here is a comprehensive overview of the Anti-D Injection (Rh Immune Globulin / RhIG):
Anti-D Injection (Rh₀(D) Immune Globulin)
What It Is
Anti-D injection is a preparation of human IgG antibodies directed against the D antigen of the Rhesus (Rh) blood group system. It is given to Rh(D)-negative individuals to prevent sensitization (alloimmunization) to Rh(D)-positive red blood cells.
Brand names: RhoGAM, HyperRHO S/D, WinRho-SDF, Rhophylac, MICRhoGAM
Why It Is Needed — The Problem It Prevents
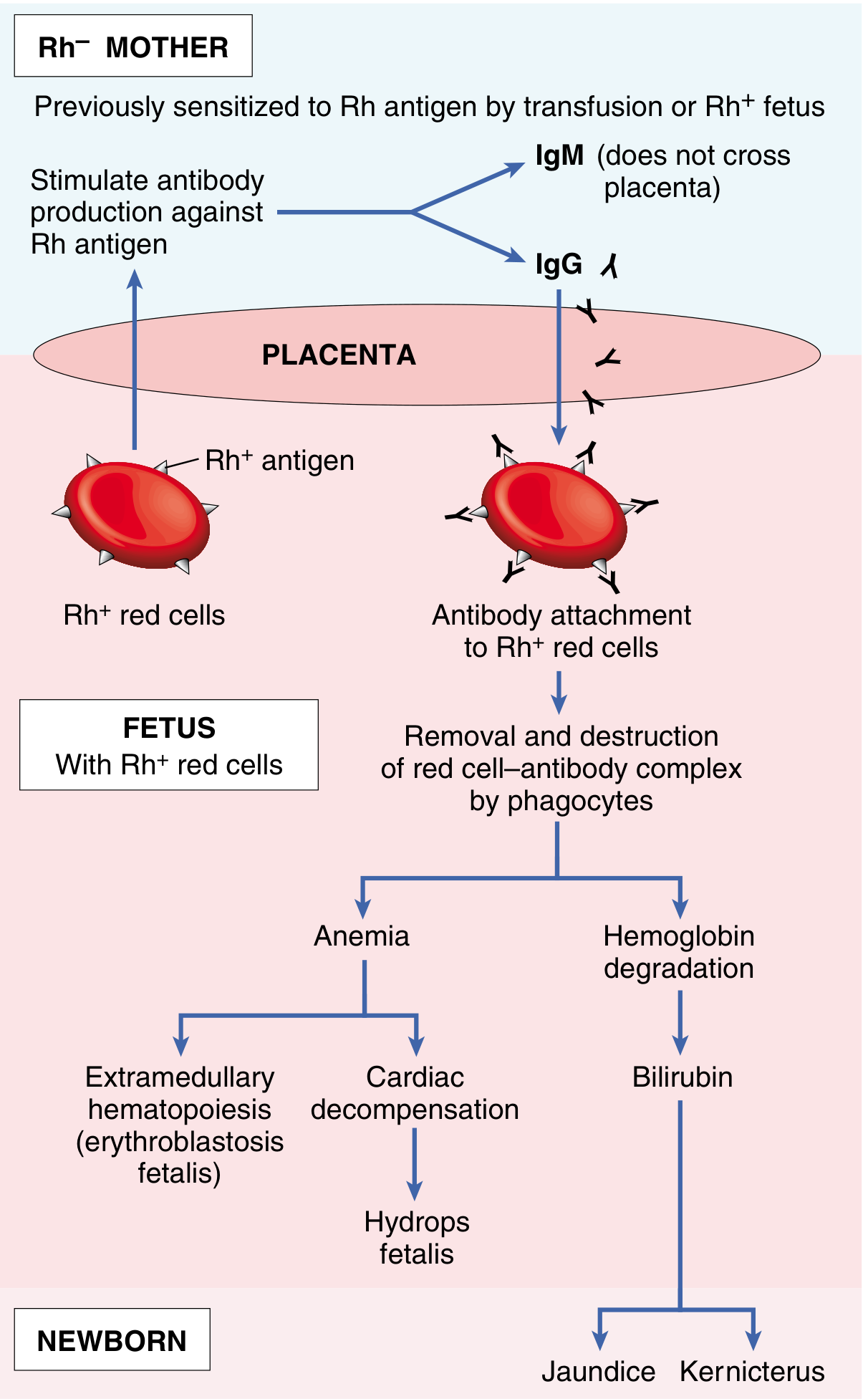
When an Rh(D)-negative mother carries an Rh(D)-positive fetus, fetal red cells can enter maternal circulation (fetomaternal hemorrhage), especially during delivery or trauma. This triggers the mother's immune system to produce anti-D antibodies (initially IgM — which don't cross the placenta — then IgG on subsequent exposure).
In a subsequent Rh-positive pregnancy, the pre-formed maternal IgG anti-D antibodies cross the placenta and destroy fetal red cells, causing:
- Fetal anemia → cardiac decompensation → Hydrops fetalis
- Hemoglobin breakdown → Jaundice and Kernicterus
- Extramedullary hematopoiesis (erythroblastosis fetalis)
Rh disease is therefore uncommon in the first pregnancy but becomes progressively worse in subsequent ones. — Robbins, Cotran & Kumar Pathologic Basis of Disease
Mechanism of Action
Anti-D immunoglobulin works by passive immunization — the exogenous anti-D antibodies coat and rapidly clear any Rh(D)-positive fetal red cells from the maternal circulation before they can trigger the mother's own immune response. This prevents active sensitization.
Indications
1. Obstetric prophylaxis (primary use):
- Antenatal dose at 28 weeks gestation (routine)
- Postnatal dose within 72 hours of delivery of an Rh(D)-positive baby
- Following miscarriage/abortion, ectopic pregnancy, or termination (even early pregnancy — fetal cells can reach maternal circulation)
- Following invasive procedures: amniocentesis, chorionic villus sampling (CVS), cordocentesis
- Following abdominal trauma in pregnancy
- Antepartum hemorrhage (threatened/actual)
- External cephalic version
2. Transfusion:
- Prevention of isoimmunization in Rh(D)-negative individuals transfused with Rh(D)-positive blood or blood components
3. Immune Thrombocytopenic Purpura (ITP):
- In non-splenectomized, Rh(D)-positive patients (IV formulation only — WinRho-SDF, Rhophylac)
Doses
| Indication | Preparation | Dose |
|---|---|---|
| Antenatal prophylaxis (28 wks) | IM | 1500 IU (300 mcg) |
| Postnatal (within 72 hrs) | IM | 1500 IU (300 mcg) |
| Early pregnancy loss (<12 wks) | IM | 250 IU (50 mcg) mini-dose |
| Massive fetomaternal hemorrhage | IM/IV | Additional doses (guided by Kleihauer-Betke test) |
| ITP (Hgb ≥10 g/dL) | IV | 250 IU/kg |
| ITP (Hgb 8–10 g/dL) | IV | 125–200 IU/kg |
Conversion: 1 mcg = 5 IU — Harriet Lane Handbook
The standard full dose of 300 mcg (1500 IU) covers approximately 15 mL of fetal red cells (30 mL whole blood). If the Kleihauer-Betke test shows a larger fetomaternal bleed, additional doses are required.
Timing
- Must be given within 72 hours of the sensitizing event for maximum efficacy
- Can still offer partial protection if given up to 9–10 days after exposure
- Does NOT help if the mother is already sensitized (Coombs-positive / anti-D antibodies already present) — in that case, the pregnancy requires monitoring and management for existing disease
Contraindications & Cautions
- Contraindicated in IgA deficiency (risk of anaphylaxis)
- Do NOT give to Rh(D)-positive individuals (no benefit; wasteful)
- Do NOT give if mother is already sensitized to D antigen
- Use with caution in: atherosclerosis, hyperviscosity, coagulation disorders (thrombotic risk)
- May interfere with immune response to live vaccines (MMR, varicella) — timing should be considered
Side Effects
- Local injection site reactions (pain, redness)
- Mild systemic: fever, chills, headache
- Rare: hemolysis (especially with IV use in ITP — due to destruction of Rh(D)-positive red cells)
- Rare: intravascular hemolysis → anemia, renal insufficiency (IV use)
Key Points to Remember
| Given to | Rh(D)-negative mother only |
| Prevents | Maternal sensitization to D antigen |
| Does NOT treat | Already-sensitized (alloimmunized) mothers |
| Antenatal | 28 weeks |
| Postnatal | Within 72 hours of delivery |
| Early pregnancy events | Mini-dose (250 IU) if <12 weeks |
Sources: Harriet Lane Handbook (23rd ed.), Robbins & Cotran Pathologic Basis of Disease, Rosen's Emergency Medicine, Tietz Textbook of Laboratory Medicine
This is a shared conversation. Sign in to Orris to start your own chat.