Clubbing
Reading File
Finding Sources
Searching PubMed
digital clubbing pathophysiology causes
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have everything needed for a comprehensive answer. Here it is:
Digital Clubbing
Definition
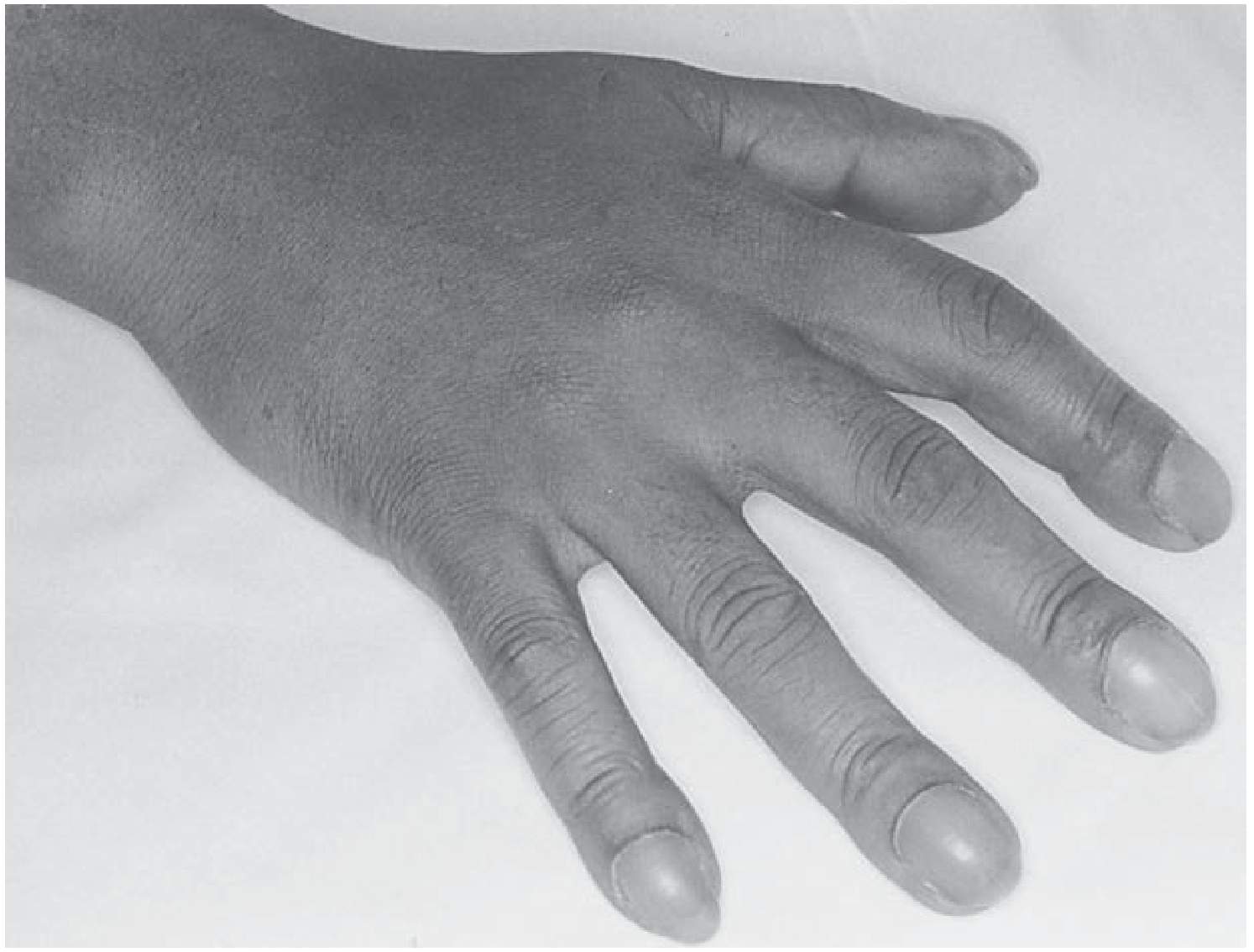
Clubbing is the selective bulbous enlargement of the distal segments of the fingers (and toes) due to proliferation of soft connective tissue, particularly on the dorsal surface, accompanied by increased sponginess at the base of the nail. First described by Hippocrates in association with empyema.
Clinical Features
Four hallmarks (Murray & Nadel's):
- Loss of the normal nail-bed angle — the nail makes a >165° angle with its cuticle (Lovibond angle >180°), effectively flattening it
- Softening and sponginess of the nail bed — the nail "floats" on its bed; periungual erythema
- Bulging/enlargement of the distal phalanx — may be warm and erythematous
- Curved nails — both longitudinal and coronal planes affected
The flattening of the nail-cuticle angle is the most sensitive single measurement.
Pathophysiology
The mechanism is not fully established but current evidence points to:
- Increased capillary density stimulated by hypoxia → vascular growth factors (VEGF, PDGF, HIF-1α, HIF-2α)
- Shunting of blood past the capillary bed of the lung or liver → angiogenic factors that are normally metabolized escape into the digital circulation
- Platelet precursors (megakaryocyte fragments) bypassing the pulmonary capillary filter release growth factors in the digital microcirculation
- Inflammation and intravascular shunting co-exist in many associated conditions (e.g., bronchiectasis, liver cirrhosis)
Clubbing can develop rapidly (within ~2 weeks, as in new-onset empyema) and can reverse (e.g., after lung transplantation for cystic fibrosis or corrective cardiac surgery).
Causes
Not associated with overt disease
- Hereditary / familial (autosomal dominant)
- Sporadic (idiopathic)
- Pachydermoperiostosis
Thoracic (most common acquired cause)
- Lung cancer — the single most common cause of acquired clubbing
- Mesothelioma, other pleural tumours
- Oesophageal cancer, lymphoma
Pulmonary infections / suppurative disease
- Bronchiectasis, cystic fibrosis
- Lung abscess, empyema
- Sarcoidosis/TB-related bronchiectasis
Interstitial lung disease
- Idiopathic pulmonary fibrosis, asbestosis
- Collagen vascular disease-related ILD
Cardiovascular
- Cyanotic congenital heart disease
- Infective endocarditis
- Pulmonary AV fistula, hereditary haemorrhagic telangiectasia
- Infected aortic graft, Takayasu's arteritis
Gastrointestinal / hepatic
- Inflammatory bowel disease (Crohn's, ulcerative colitis)
- Hepatic cirrhosis, hepatopulmonary syndrome, biliary cirrhosis
- Polyposis coli
Other
- Thyroid acropachy
- HIV (in children)
- Secondary hyperparathyroidism
- Haemoglobinopathies, congenital methaemoglobinaemia
- Drug-induced (e.g., voriconazole)
- Occupational (jackhammer operators)
Unilateral Clubbing
A distinct subset — localised to one hand/arm — caused by vascular or neurological disorders affecting that limb:
- Subclavian artery aneurysm
- Brachial AV fistula
- Median nerve injury
- Shoulder subluxation, local trauma, hemiplegia
Associated: Hypertrophic Osteoarthropathy (HOA)
Clubbing can be accompanied by HOA — subperiosteal new bone formation at the distal diaphyses of long bones (radius/ulna, tibia/fibula), causing:
- Painful, symmetric arthritis-like changes in shoulders, knees, ankles, wrists, elbows
HOA is most strongly associated with bronchogenic carcinoma, mesothelioma, cystic fibrosis, and other intrathoracic malignancies. Confirmed by plain X-ray or MRI (periosteal reaction) or bone scintigraphy (99mTc-MDP).
Clinical Significance & Workup
Clubbing was found in 1% of all internal medicine admissions and was associated with serious underlying disease in 40% of those patients. New-onset clubbing always warrants:
- Chest X-ray (first-line)
- CT thorax if CXR unrevealing — to exclude pulmonary neoplasm while it may still be localised and resectable
Sources: Harrison's Principles of Internal Medicine 22E; Murray & Nadel's Textbook of Respiratory Medicine; Fishman's Pulmonary Diseases and Disorders; Goldman-Cecil Medicine
Clubbing
The previous conversation already contains a comprehensive answer on digital clubbing. Here's a summary of what was covered:
Digital Clubbing — Summary
Definition
Selective bulbous enlargement of distal digits due to soft tissue proliferation, with increased nail-bed sponginess. First described by Hippocrates.
4 Clinical Hallmarks
- Loss of nail-bed angle (Lovibond angle >180°)
- Nail-bed softening/sponginess — nail "floats"
- Bulging distal phalanx (warm, erythematous)
- Curved nails (longitudinal + coronal planes)
Pathophysiology
- Hypoxia → VEGF, PDGF, HIF-1α/2α → increased capillary density
- Blood shunting past lung/liver → angiogenic factors reach digital circulation unmetabolised
- Megakaryocyte fragments bypass pulmonary filter → growth factor release in digits
Key Causes
| Category | Examples |
|---|---|
| Thoracic (most common) | Lung cancer #1, mesothelioma, bronchiectasis, CF, ILD, lung abscess |
| Cardiac | Cyanotic CHD, infective endocarditis, pulmonary AV fistula |
| GI/Hepatic | IBD, hepatic cirrhosis, hepatopulmonary syndrome |
| Idiopathic/familial | Hereditary, pachydermoperiostosis |
| Other | Thyroid acropachy, HIV, voriconazole (drug-induced) |
Unilateral Clubbing
Localised vascular/neurological cause: subclavian aneurysm, brachial AV fistula, median nerve injury, hemiplegia
Hypertrophic Osteoarthropathy (HOA)
Subperiosteal new bone at distal long bone diaphyses → painful arthritis-like changes. Strongly linked to bronchogenic carcinoma and mesothelioma. Confirmed by X-ray, MRI, or bone scan.
Workup for New-Onset Clubbing
- CXR first
- CT thorax if CXR normal — exclude occult pulmonary neoplasm
Clubbing = serious disease in 40% of cases; always investigate.
This is a shared conversation. Sign in to Orris to start your own chat.