Gustillo Anderson classification and management
Reading File
Finding Sources
Finding Sources
Searching PubMed
"open fracture" AND "Gustilo" AND classification management
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
Gustilo Anderson open fracture classification types
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I have all the information needed. Here is the comprehensive answer:
Gustilo–Anderson Classification of Open Fractures
The Gustilo–Anderson (G-A) classification is the most widely used system for open fractures. It evaluates three variables: wound size, degree of contamination, and extent of soft tissue injury. True classification can only be finalised intraoperatively (after debridement), not at initial presentation — the type may upgrade with further debridement. There is considerable interobserver variability (42–94% agreement).
Classification
| Type | Wound | Soft Tissue | Fracture Pattern | Mechanism |
|---|---|---|---|---|
| I | < 1 cm, clean | Minimal muscle contusion; no periosteal stripping | Simple transverse/oblique | Low energy; usually "inside-out" (bone pierces skin) |
| II | 1–10 cm | Moderate damage; flaps/avulsion without extensive crush; little periosteal stripping | Simple transverse/short oblique, minimal comminution | Moderate energy |
| IIIA | > 10 cm (or any size with heavy contamination) | Extensive laceration; periosteal stripping present but adequate soft tissue cover remains after debridement | Segmental fracture, comminution | High energy: gunshot, farm/barnyard, shotgun |
| IIIB | Same as IIIA | Extensive periosteal stripping + bone exposure — inadequate coverage; flap required | Comminuted/segmental | High energy + contamination |
| IIIC | Any size | Any extent of soft tissue injury | Any pattern | Vascular injury requiring repair — regardless of wound size |
Key memory point: The distinction between IIIA, IIIB, and IIIC depends on soft tissue cover adequacy and vascular status, NOT wound size alone.
Clinical Example — Type I (inside-out puncture wound)

Clinical Example — Type III (massive soft tissue disruption)

Infection Risk by Grade
| Grade | Infection Rate |
|---|---|
| Type I | 0–2% |
| Type II | 2–10% |
| Type IIIA | ~10–25% |
| Type IIIB | ~10–50% |
| Type IIIC | Highest (+ amputation risk) |
In practice, clinicians often dichotomise into IIIB/IIIC vs. all others, as infection rates for Types I, II, and IIIA are similar, while IIIB/IIIC require soft tissue coverage and carry substantially higher morbidity.
Management
1. Emergency / Initial
- ATLS primary survey — manage life-threatening injuries first
- Wound: bedside irrigation of gross contamination, loose sterile dressing, splint; avoid repeated inspection in the ED to minimise contamination
- Fracture reduction and splinting
- Mark NPO; arrange theatre
2. Antibiotics (Most Important Intervention)
Antibiotics must be started within 1 hour of injury (some protocols push prehospital administration for severe injuries). Delay beyond 3 hours significantly increases infection risk.
| Grade | Agent | Duration |
|---|---|---|
| Type I & II | Cefazolin (1st-gen cephalosporin) | 24 h after primary closure; 24 h after each subsequent procedure |
| Type III | Cefazolin + aminoglycoside (gentamicin/tobramycin) | 48 h from presentation; 24 h after each subsequent procedure |
| Soil/farm contamination | + Penicillin G (anaerobic/clostridial cover) | Single dose or extended per severity |
| Freshwater contamination | Fluoroquinolone (ciprofloxacin/levofloxacin) or 3rd/4th-gen cephalosporin | — |
| Saltwater contamination | Doxycycline + ceftazidime (Vibrio coverage) | — |
| True penicillin allergy | Clindamycin ± vancomycin (if high community MRSA rate) | — |
Aminoglycoside caveat: Dose-dependent nephrotoxicity and ototoxicity have led some institutions to omit aminoglycosides — use is declining. Check local protocols.
3. Tetanus Prophylaxis
| Patient Status | Tetanus-Prone Wound | Non-tetanus-Prone Wound |
|---|---|---|
| Unknown / < 3 doses | Toxoid + Human Tetanus Immunoglobulin (TIG) | Toxoid only |
| Fully immunised, last booster > 5 years | Toxoid booster | Not required |
Tetanus-prone wound: > 6 hours old, > 1 cm deep, devitalised tissue, gross contamination.
4. Debridement and Irrigation
- Perform within 6–24 hours of injury
- Thorough excision of all devitalised muscle, bone, and contaminated tissue
- Pulsed lavage irrigation (normal saline); low-pressure irrigation is as effective as high-pressure and avoids driving bacteria deeper into tissue
- Counter-incisions to improve wound access reduce flap rates (especially medial ankle)
- Repeat debridement every 48–72 hours if needed until wound is clean
- Antibiotic bead pouch (methylmethacrylate + tobramycin ± vancomycin): useful for highly contaminated wounds as local antibiotic delivery
5. Fracture Stabilisation
- Reduces further soft tissue damage and facilitates wound management
- Options:
- External fixator — preferred for heavily contaminated/unstable wounds, temporary stabilisation before definitive fixation
- Intramedullary nail — suitable for Type I–IIIA fractures once adequately debrided (widely used for tibial shaft fractures)
- Plate fixation (ORIF) — selected cases, requires good soft tissue coverage
- Spanning external fixator — periarticular open fractures
6. Wound Coverage
| Timeframe | Significance |
|---|---|
| Primary closure (same sitting) | Only if wound can be closed without tension after debridement (Type I/II) |
| < 7 days | Goal for definitive soft tissue coverage |
| > 7 days | Significantly increased infection risk |
Tibia coverage by zone (rule of thumb):
- Proximal third → Gastrocnemius muscle flap
- Middle third → Soleus muscle flap
- Distal third → Fasciocutaneous flap or free-tissue transfer (microvascular)
Negative pressure wound therapy (VAC): useful adjunct between debridements but is NOT a substitute for definitive coverage.
7. Vascular Injury (Type IIIC)
- Requires urgent vascular surgery consultation
- Temporary vascular shunt → skeletal stabilisation → definitive vascular repair (preferred sequence)
- Warm ischaemia time: revascularisation should be complete within 6 hours to avoid irreversible muscle necrosis
- Amputation rates for IIIC historically up to 50%; early multidisciplinary approach improves limb salvage
8. Compartment Syndrome Monitoring
All high-energy open fractures (especially tibia) require serial compartment assessments. Paradoxically, the open wound may decompress one compartment but not others. Fasciotomy threshold: compartment pressure > 30 mmHg, or within 30 mmHg of diastolic blood pressure.
Limitations of G-A Classification
- Designed originally for open tibia fractures only — validity for other bones is extrapolated
- Poor interobserver reliability (42–94%)
- Final grade can only be assigned intraoperatively, not at presentation
- Treatment-based rather than anatomy-based (type of wound closure defines IIIB)
OTA Open Fracture Classification (OTA-OFC)
Developed to address these shortcomings. Grades five independent factors:
- Skin (laceration size/complexity)
- Muscle (degree of loss)
- Arterial injury
- Contamination
- Bone loss
The OTA-OFC is more precise and better predicts outcomes than G-A, but its complexity has limited widespread adoption. The G-A system remains the standard in clinical practice.
Sources: Rockwood and Green's Fractures in Adults, 10th ed. (2025); Miller's Review of Orthopaedics, 9th ed.; Sabiston Textbook of Surgery; Bailey and Love's Short Practice of Surgery, 28th ed.
Development dysplasia of hip diagnosis and treatment
Reading File
Finding Sources
Finding Sources
Searching PubMed
"developmental dysplasia of the hip"[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Searching Images
developmental dysplasia of hip DDH Pavlik harness ultrasound Graf classification
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the data needed for a comprehensive, illustrated answer. Let me compile it.
Developmental Dysplasia of the Hip (DDH)
DDH describes a spectrum of hip instability ranging from a shallow (dysplastic) acetabulum that may sublux, to a fully dislocated hip that is irreducible. The key underlying problem is failure of normal concentric development between the femoral head and the acetabulum.
Spectrum of Disease
| Grade | Description |
|---|---|
| Dysplasia | Shallow acetabulum; femoral head in joint but inadequately covered |
| Subluxation | Femoral head partially displaced, within the labrum |
| Dislocation (reducible) | Ortolani positive — dislocated but reducible |
| Dislocation (irreducible) | Ortolani negative — dislocated and cannot be reduced |
| Teratologic | Dislocated in utero, irreducible at birth; associated with arthrogryposis, Larsen syndrome, trisomy 21 |
Incidence & Risk Factors
- Neonatal instability: ~20 per 1,000 live births; true dislocation ~2 per 1,000
- Many hips stabilise spontaneously within the first 2–3 weeks
Risk factors (in decreasing importance):
- Breech presentation (especially extended breech) — 30–50× increased risk
- Female sex — 4–5× more common; oestrogen-related peripartum ligamentous laxity
- Positive family history — ≥20% incidence with affected first-degree relative
- Firstborn child — tight primigravid uterus, left occipito-anterior position → 67% left hip
- Oligohydramnios — restricts fetal movement
- Swaddling with hips in extension — postnatal risk factor
Associations: torticollis (20%), metatarsus adductus (10%); no association with clubfoot.
Diagnosis
Clinical Examination — Neonate
The critical question at neonatal examination:
Is the hip dislocated? If so, is it reducible (Ortolani +) or irreducible? If not dislocated, is it dislocatable (Barlow +)?
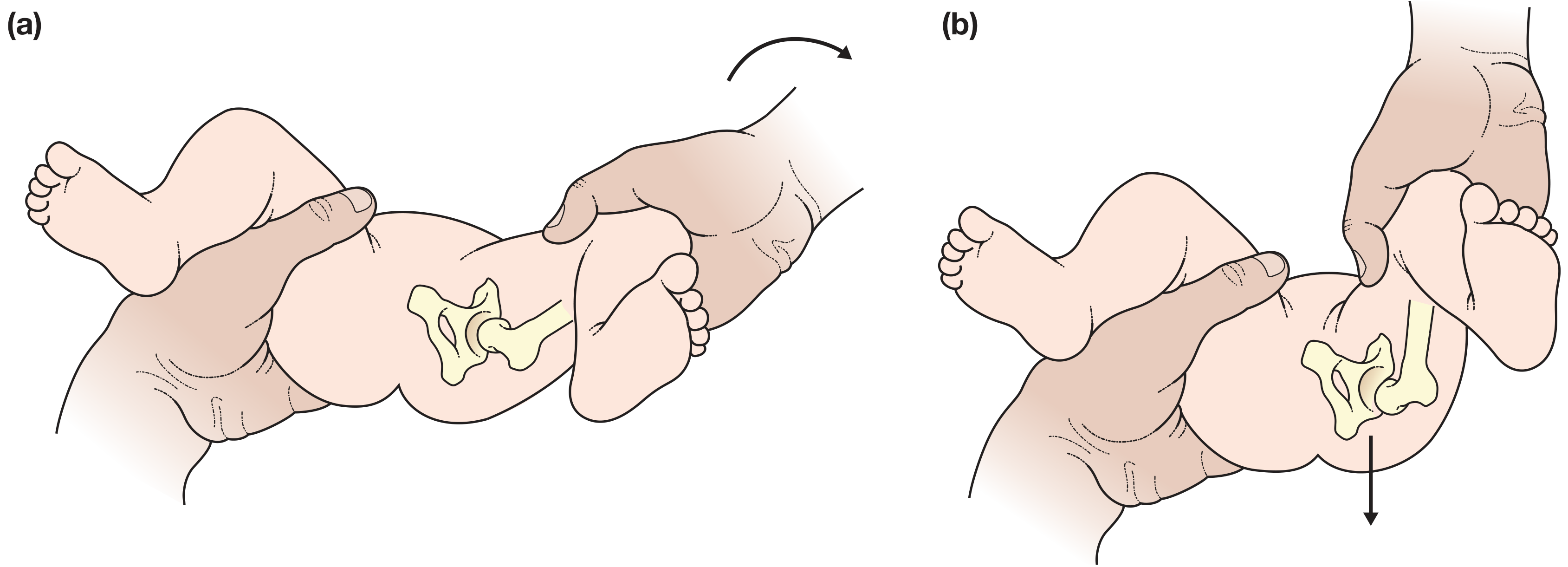
Ortolani test: Hip at 90° flexion → gentle abduction + elevation of greater trochanter → clunk of reduction = positive (dislocated but reducible)
Barlow test: Hip at 90° flexion → adduction + posterior pressure on knee → clunk of dislocation = positive (reduced but dislocatable)
Bilateral dislocation may be missed — abduction is symmetrically limited and may appear normal in low-tone infants.
Clinical Examination — Older Infant/Child
| Sign | Age | Finding |
|---|---|---|
| Limited hip abduction | > 3 months | < 60° abduction on affected side |
| Galeazzi sign | Any | Apparent femoral shortening — knees at unequal heights with hips & knees at 90° |
| Asymmetric thigh/gluteal folds | Infant | Less reliable |
| Trendelenburg gait | Toddler | Contralateral pelvis drops when standing on affected leg |
| Limping / tip-toe gait | Child | Affected leg appears short |
| Lumbar lordosis + waddling gait | Bilateral | |
| Exercise-related groin/knee pain | Adolescent |
Investigations
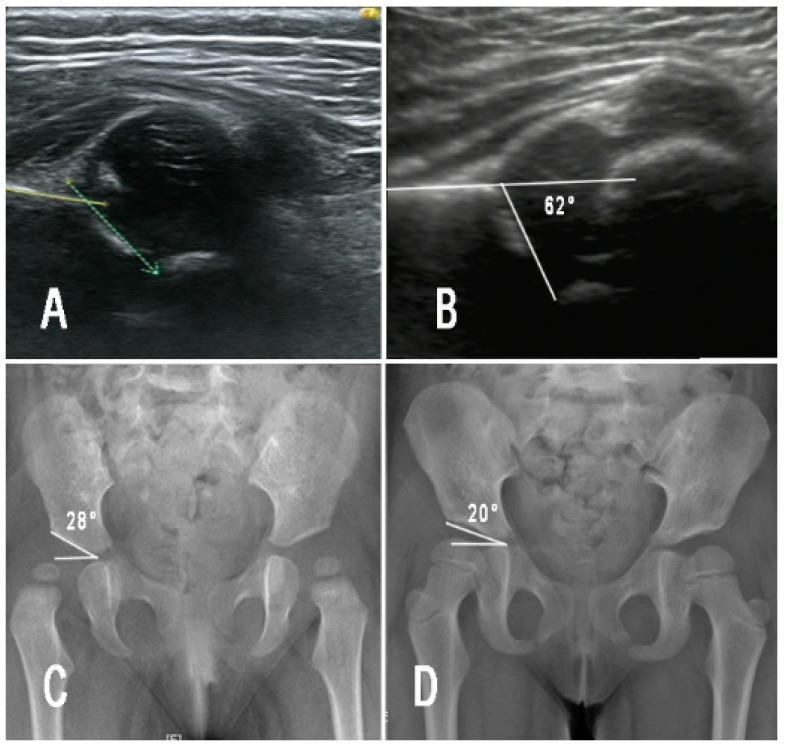
1. Ultrasound (< 4–6 months)
Modality of choice in the neonatal period, since the femoral head is cartilaginous and not visible on X-ray until 4–6 months.
Performed at 4–6 weeks of age (coronal view, lateral decubitus position):
Graf Classification (α angle on coronal US):
| Graf Type | α angle | Interpretation | Action |
|---|---|---|---|
| I | ≥ 60° | Normal, mature | None |
| IIa | 50–59° | Immature (< 3 months) | Follow-up |
| IIb | 50–59° | Delayed ossification (> 3 months) | Treatment |
| IIc | 43–49° | Critical zone — borderline | Treatment |
| III | < 43° | Subluxed; cartilaginous roof displaced | Treatment |
| IV | — | Dislocated | Treatment |
Normal: α > 60°; femoral head bisected by the iliac line; Morin index (femoral head coverage) > 50%.
Selective US screening is recommended for:
- Breech presentation
- Positive family history
- Abnormal clinical examination
2. Plain Radiograph (≥ 4–5 months)
Used once the femoral ossific nucleus begins to appear (normally 4–6 months; often delayed in DDH).
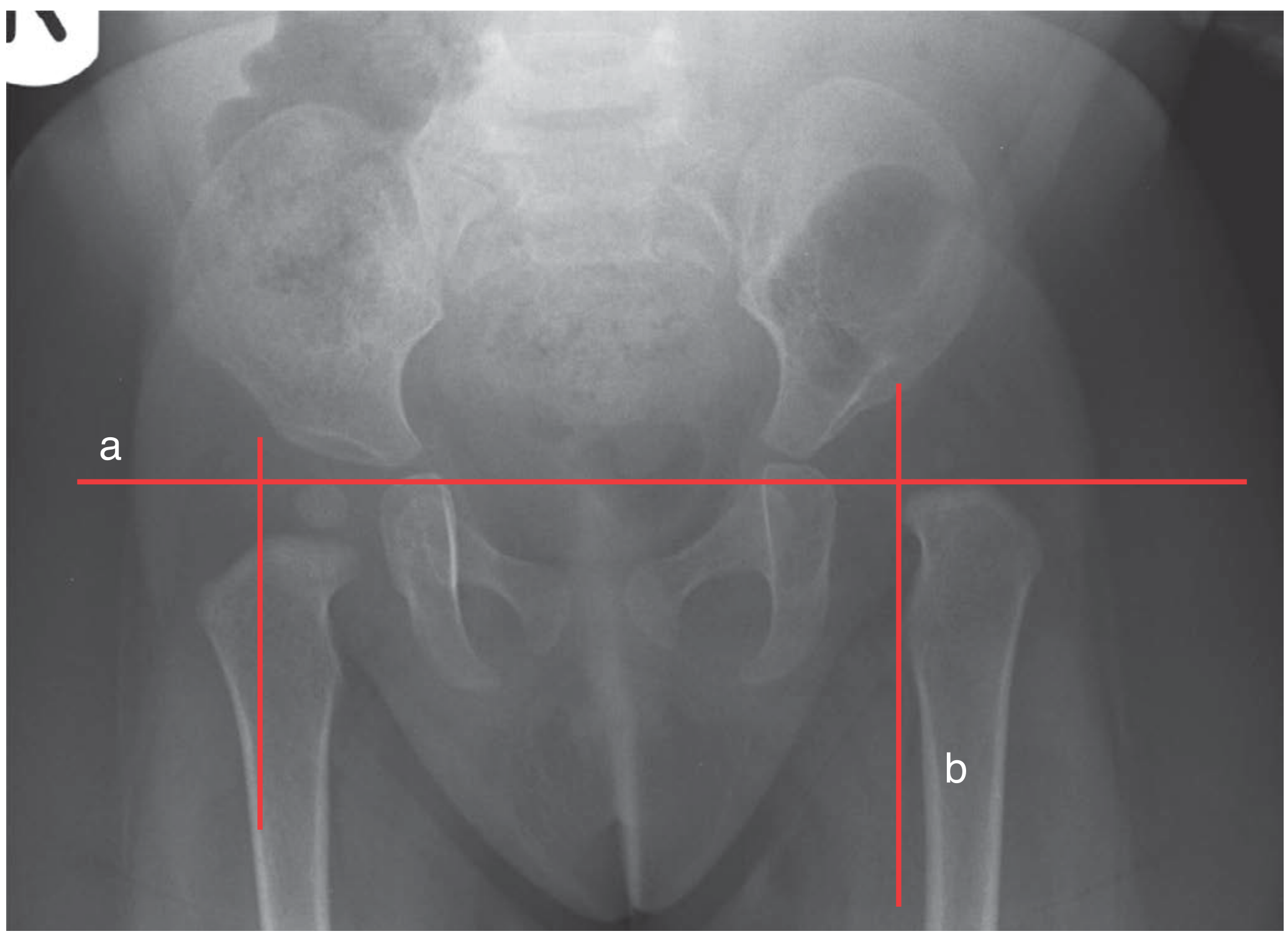
Key radiographic lines and measurements:
| Line / Measurement | Description | Normal |
|---|---|---|
| Hilgenreiner's line | Horizontal line through both triradiate cartilages (Y-cartilages) | Reference line |
| Perkin's line | Vertical line through lateral acetabular edge, perpendicular to Hilgenreiner's | Ossific nucleus should be medial |
| Shenton's line | Smooth arc from femoral neck to superior pubic ramus | Disrupted in dislocation/subluxation |
| Acetabular index (AI) | Angle between Hilgenreiner's line and roof of acetabulum | Normal: < 25–30° (decreases with age) |
| Centre-edge (Wiberg) angle | In older children — lateral femoral head coverage | Normal > 25° |
3. Arthrography
Used intraoperatively to:
- Confirm concentric reduction before casting
- Identify blocks to reduction (the "thorn sign" indicates normal labral position)
- Assess medial dye pool width (> 8 mm suggests inadequate reduction)
4. CT / MRI
- Post-reduction confirmation of concentric reduction in the spica cast
- MRI preferred (no radiation) for post-reduction assessment
- CT used where MRI unavailable
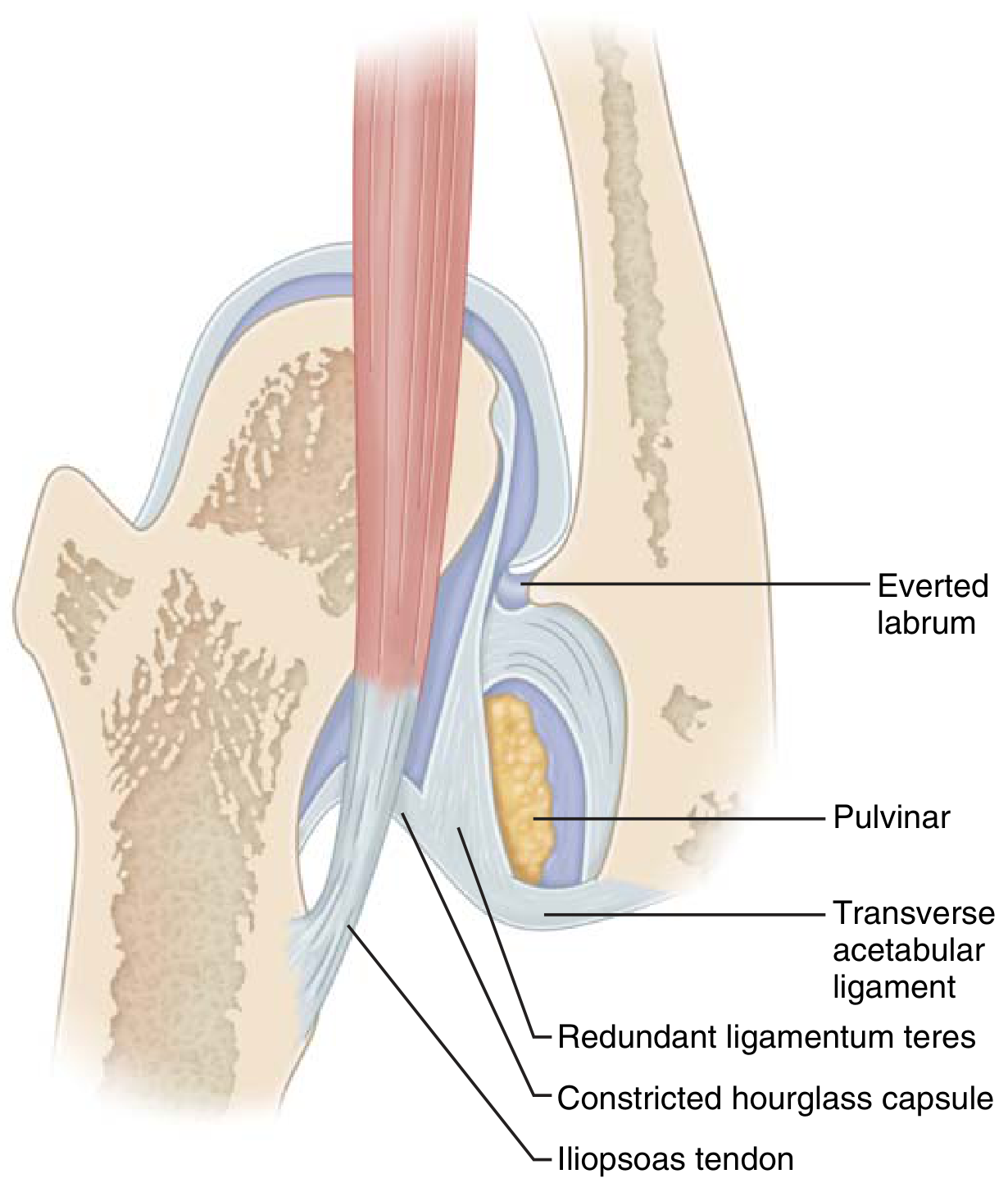
Blocks to Concentric Reduction
When a hip cannot be reduced, the following structures are implicated:
Treatment
The overarching goal is stable concentric reduction of the femoral head within the acetabulum, achieved as early as possible to allow normal acetabular development — while avoiding avascular necrosis (AVN) of the femoral head, the most feared complication.
Age 0–6 Months: Pavlik Harness
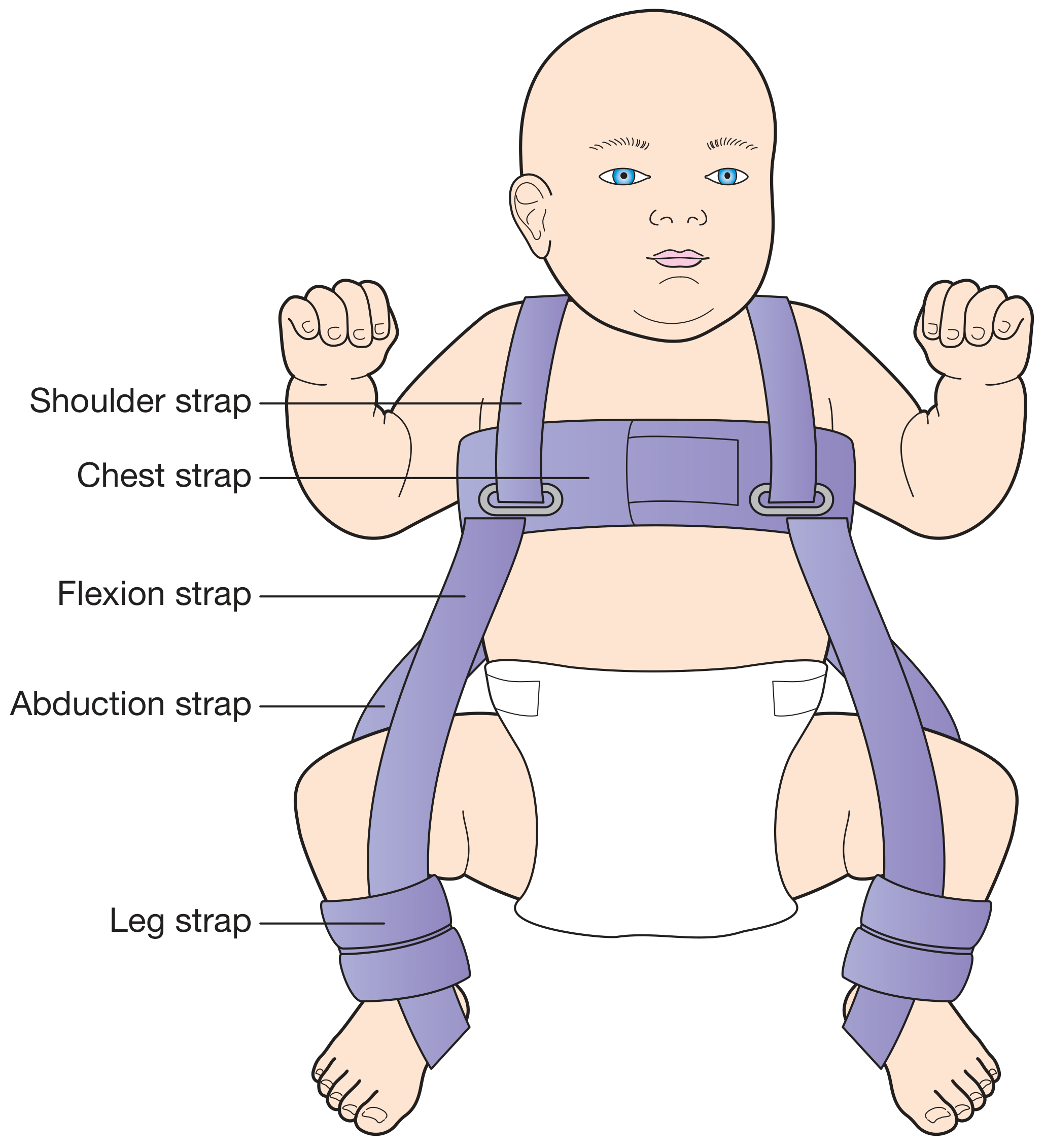
- First-line treatment for all Ortolani-positive and Barlow-positive hips (reducible and dislocatable)
- Maintains hips in the "human position" — ~100° of flexion, mild abduction (Salter position)
- Worn 23 hours/day for at least 6 weeks after reduction achieved, then part-time (nights/naps) for a further 6–8 weeks
- Reduction confirmed by ultrasound after fitting; repeat US to monitor
Safe zone (Ramsey zone): Between maximum adduction before redislocation and maximum abduction before AVN risk. A narrow safe zone (< 40°) is an indication for adductor tenotomy.
Complications of Pavlik harness:
- AVN — from excessive abduction (compresses posterosuperior retinacular branch of medial femoral circumflex artery)
- Femoral nerve palsy — from excessive flexion (transient)
- "Pavlik disease" — if reduction is not achieved within 3 weeks, continued harness use causes erosion of the pelvis superior to the acetabulum, making subsequent closed reduction more difficult → discontinue at 3 weeks if not reduced
Risk factors for harness failure:
- Age > 7 weeks at initiation
- Bilateral dislocations
- Absent Ortolani sign (irreducible hip)
- Teratologic dislocation (absolute contraindication)
Age 6–18 Months: Closed Reduction + Spica Cast
For hips failing Pavlik harness treatment, or presenting in this age group.
Procedure (under general anaesthetic):
- Examination under anaesthetic
- Hip arthrography — assess reduction and blocks
- Adductor ± psoas tenotomy if tight
- Closed reduction — gentle traction + flexion + abduction
- Hip spica cast in the stable zone of abduction (hips ≥ 90° flexion)
- Post-reduction CT or MRI to confirm concentric reduction
If closed reduction fails or only achieved in extreme position → proceed to open reduction.
Age 6–18 Months (failed closed) / Age ≥ 18 Months: Open Reduction
Approach:
- Medial approach (Ferguson/Ludloff): 6–24 months; allows direct access to medial obstacles; does not permit simultaneous capsulorrhaphy
- Anterior (Smith-Petersen) approach: preferred from 9–12 months onwards; allows capsulorrhaphy; lower risk to medial femoral circumflex artery than medial approach at older ages
Structures released at open reduction:
- Adductor longus tenotomy
- Iliopsoas release
- Pulvinar excision
- Transverse acetabular ligament division
- Labrum repositioning
- Capsulorrhaphy (tightening of capsule) to maintain reduction
Femoral shortening osteotomy: Added for children > 18 months to reduce excessive pressure on reduction (reduces AVN risk).
Pelvic Osteotomies (for residual acetabular dysplasia)
| Osteotomy | Age | Mechanism |
|---|---|---|
| Salter | 18 months–6 years | Single innominate osteotomy; redirects acetabulum anterolaterally; requires open triradiate cartilage |
| Pemberton | 18 months–8 years | Incomplete pericapsular osteotomy; reduces acetabular volume; good for large femoral heads |
| Dega | Similar to Pemberton | Posterior hinge; useful in neuromuscular DDH |
| Triple osteotomy (Steel/Tönnis) | Older children, skeletal near-maturity | Three cuts (ilium, ischium, pubis); triradiate cartilage must be closed or near-closed |
| Periacetabular (Ganz/PAO) | Adolescent/adult; closed triradiate | Redirects entire acetabulum; best for reducible dysplastic hips; preserves posterior column |
| Chiari | Salvage | Medial displacement osteotomy; non-anatomic; used for irreducible dysplasia |
| Shelf/augmentation | Salvage | Extends acetabular roof with bone graft |
Surgery is contraindicated in children > 6–8 years with bilateral dislocations and > 8–10 years with unilateral — the pseudoacetabulum provides sufficient function and correction risks more harm than benefit.
Summary Treatment Algorithm
Birth → Neonatal exam (Ortolani / Barlow)
│
├─ Unstable / dislocated → Observe 2–3 weeks (many resolve spontaneously)
│ Still abnormal at 4–6 weeks → Ultrasound + Pavlik harness
│
├─ 0–6 months → Pavlik harness (23 h/day x 6–8 weeks)
│ Reduced → Continue until US/XR normal
│ Not reduced in 3 weeks → Stop harness → EUA + closed reduction + spica
│
├─ 6–18 months → EUA + arthrogram + closed reduction + spica cast
│ Failure → Open reduction (medial or anterior approach) ± adductor tenotomy
│
├─ 18 months–3 years → Open reduction + femoral shortening + possible pelvic osteotomy
│
├─ 3–8 years → Open reduction + pelvic osteotomy (Salter/Pemberton/Dega)
│
├─ Older child / adolescent → Triple/PAO osteotomy ± femoral osteotomy
│
└─ Adult → PAO (if reducible), Chiari/shelf (salvage), or THA when arthritic
Complications
| Complication | Cause | Comments |
|---|---|---|
| Avascular necrosis (AVN) | Excessive abduction, forced reduction, medial approach | Most feared; graded I–V; can lead to permanent deformity and early OA |
| Redislocation | Inadequate capsulorrhaphy or reduction | Requires repeat intervention |
| Residual acetabular dysplasia | Incomplete treatment response | May need pelvic osteotomy |
| Femoral nerve palsy | Excessive flexion in Pavlik harness | Transient; resolves on harness adjustment |
| Leg length discrepancy | AVN or growth disturbance | — |
| Early osteoarthritis | Untreated or poorly treated DDH | Leads to THA in adult life |
| "Pavlik disease" | Continued harness when not reducing | Acetabular erosion; complicates later reduction |
Sources: Miller's Review of Orthopaedics, 9th ed.; Bailey and Love's Short Practice of Surgery, 28th ed.; Schwartz's Principles of Surgery, 11th ed.; Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.