External carotid artery and its branches and Internal carotid artery and its branches with images . In detailed notes for mbbs student
Reading File
Finding Sources
Finding Sources
Searching the Web
external carotid artery branches mnemonic MBBS anatomy detailed
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Finding Sources
Reading File
Loading Image
Reading File
Finding Sources
Loading Image
Reading File
Loading Image
I now have all the content and images needed to write comprehensive MBBS notes. Let me compose the full detailed answer.
External & Internal Carotid Arteries - Detailed MBBS Notes
COMMON CAROTID ARTERY - Overview
The common carotid artery (CCA) bifurcates at the level of the upper border of the thyroid cartilage (C3-C4 level) into:
- External carotid artery (ECA) - supplies structures external to the skull
- Internal carotid artery (ICA) - enters the skull to supply the brain
At the bifurcation, the carotid sinus (a slight dilation) contains baroreceptors (CN IX - glossopharyngeal nerve). The carotid body (chemoreceptor) lies here too.
Origin: Right CCA arises from the brachiocephalic trunk; Left CCA arises directly from the aortic arch.
PART 1: EXTERNAL CAROTID ARTERY (ECA)
Origin and Course
The ECA arises from the CCA at the level of the upper border of the thyroid cartilage. It lies anteromedial to the ICA at its origin, then winds laterally and posteriorly to it as it ascends. It passes through or deep to the parotid gland and terminates behind the neck of the mandible by dividing into its two terminal branches (maxillary and superficial temporal arteries).
Relations:
- Medially: Hyoid bone, pharyngeal wall, superior laryngeal nerve, stylopharyngeus muscle
- Laterally: Internal carotid artery (initially)
- Superficially crossed by: Hypoglossal nerve (CN XII), lingual vein, facial vein, posterior belly of digastric, stylohyoid muscle
Mnemonic for 8 Branches: "Some Anatomists Like Fucking, Others Prefer Sex & Masturbation"
Or the classic MBBS mnemonic: "S A L F O P S M" (read as SALFOPSM)
| Letter | Branch |
|---|---|
| S | Superior thyroid artery |
| A | Ascending pharyngeal artery |
| L | Lingual artery |
| F | Facial artery |
| O | Occipital artery |
| P | Posterior auricular artery |
| S | Superficial temporal artery (terminal) |
| M | Maxillary artery (terminal) |
Diagram: Common Carotid and External Carotid Artery
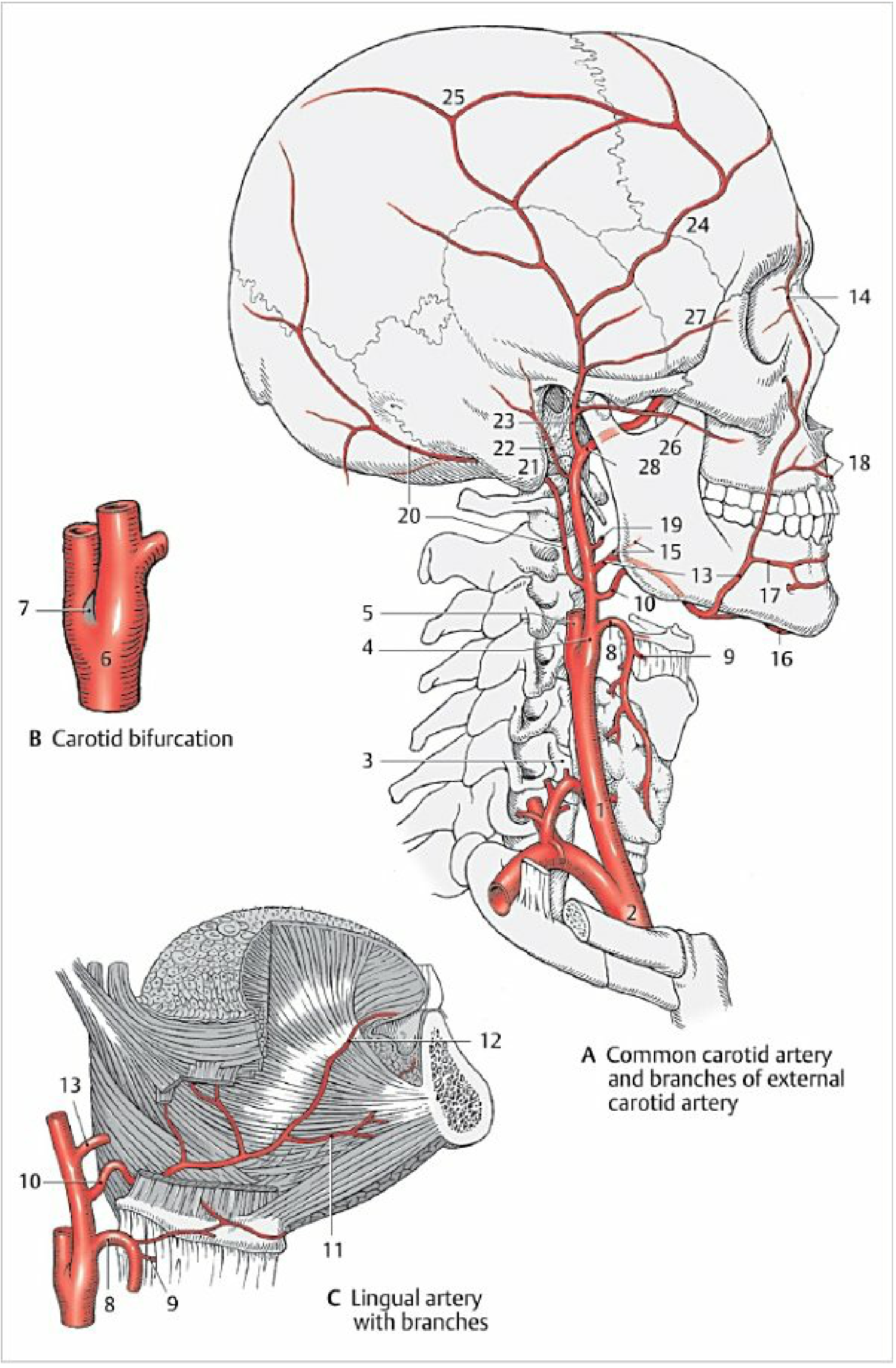
Fig. 2.21 - Common carotid artery and branches of the external carotid artery (Color Atlas of Human Anatomy, Vol. 2)
Branches of the ECA in Order
1. Superior Thyroid Artery
- Origin: First branch; arises from the anterior surface of ECA near or at the bifurcation
- Course: Passes downward and forward to the superior pole of the thyroid gland
- Branches:
- Superior laryngeal artery - pierces the thyrohyoid membrane to supply the interior of the larynx
- Sternocleidomastoid branch
- Cricothyroid branch
- Infrahyoid branch
- Supply: Thyroid gland (superior pole), larynx, sternocleidomastoid, cricothyroid
Clinical note: Ligated during thyroidectomy; injury to the superior laryngeal nerve (runs with this artery) causes loss of high-pitched phonation.
2. Ascending Pharyngeal Artery
- Origin: Second branch; smallest branch; arises from the posterior/medial aspect of the ECA
- Course: Ascends between the ICA and the wall of the pharynx to the base of skull
- Supply: Pharyngeal constrictors, stylopharyngeus, soft palate, palatine tonsil, pharyngotympanic (Eustachian) tube, meninges of the posterior cranial fossa (via posterior meningeal artery), tympanic cavity (via inferior tympanic artery)
3. Lingual Artery
- Origin: Anterior surface of ECA, at the level of the greater horn of the hyoid bone, just above the superior thyroid artery
- Course: Passes deep to the hypoglossal nerve (CN XII), runs between the middle pharyngeal constrictor and hyoglossus
- Branches:
- Dorsal lingual arteries - supply posterior tongue, tonsil, epiglottis
- Deep lingual artery (ranine artery) - supplies deep/anterior tongue (visible under tongue)
- Sublingual artery - supplies sublingual gland, floor of mouth, gums
- Supply: Tongue, sublingual gland, soft palate, tonsil, epiglottis
Clinical: Lingual artery is ligated in partial glossectomy. The deep lingual artery can be seen through the mucosa on the underside of the tongue.
4. Facial Artery
- Origin: Anterior surface of ECA, just above the lingual artery; may share a common trunk with lingual artery (linguofacial trunk)
- Course in neck: Passes deep to stylohyoid and posterior belly of digastric, then into the submandibular gland, loops over the submandibular gland and hooks under the mandible just anterior to the masseter (where the pulse is palpable)
- Course in face: Enters the face at the antero-inferior angle of the masseter, runs a tortuous course superiorly and medially, ends at the medial angle of the eye as the angular artery (anastomoses with the ophthalmic artery)
- Branches in neck:
- Ascending palatine artery
- Tonsillar artery (main supply to palatine tonsil)
- Submental artery
- Glandular branches to submandibular gland
- Branches in face:
- Inferior labial artery
- Superior labial artery (supplies nasal septum anteriorly)
- Lateral nasal artery
- Angular artery (terminal branch)
- Supply: Face from inferior border of mandible to medial angle of eye, tonsil, soft palate, submandibular gland
Clinical: The tortuous course is an adaptation to allow stretching during facial movements. The angular artery anastomoses with the ophthalmic artery (ICA territory) - this is a dangerous anastomosis for infections (spread to cavernous sinus). Facial pulse palpable at the inferior border of the mandible anterior to the masseter.
5. Occipital Artery
- Origin: Posterior surface of ECA, opposite the facial artery
- Course: Passes upward and posteriorly, deep to the posterior belly of digastric (which forms a notch on the artery), crosses the sternocleidomastoid, passes through the trapezius, and emerges on the posterior scalp
- Supply: Sternocleidomastoid, meninges of posterior cranial fossa, mastoid air cells, deep muscles of the back of the neck, posterior scalp (up to vertex)
Clinical: The groove (notch) of the occipital artery on the digastric is a surgical landmark. Occipital neuralgia may be confused with vascular headache.
6. Posterior Auricular Artery
- Origin: Posterior surface of ECA, above the digastric and stylohyoid, just above the occipital artery
- Course: Passes superiorly and posteriorly between the mastoid process and the auricle
- Branches:
- Stylomastoid artery - enters stylomastoid foramen, supplies facial nerve (CN VII), tympanic cavity, mastoid antrum, semicircular canals
- Posterior tympanic artery - to tympanic cavity
- Auricular and occipital branches - supply external ear and scalp posterior to ear
- Supply: Parotid gland, nearby muscles, external ear, scalp posterior to ear, middle and inner ear structures
Clinical: Stylomastoid artery is the main blood supply to CN VII in the facial canal - must be preserved in facial nerve surgery.
7. Superficial Temporal Artery (Terminal Branch)
- Origin: One of the two terminal branches of ECA; begins posterior to the neck of the mandible inside the parotid gland
- Course: Passes superiorly, emerges from the upper border of the parotid gland, crosses the zygomatic process of the temporal bone just anterior to the ear (where the pulse is palpable and artery is superficially placed), and divides into anterior and posterior branches in the temporal region
- Branches:
- Transverse facial artery - runs horizontally across the face between the parotid duct and zygomatic arch
- Zygomatico-orbital artery
- Anterior temporal (frontal) branch - supplies forehead, frontal scalp
- Posterior temporal (parietal) branch - supplies temporal, parietal scalp
- Middle temporal artery
- Supply: Parotid gland, masseter, lateral face, anterior ear, temporalis muscle, lateral scalp
Clinical: Superficial temporal artery pulse is palpable anterior to the tragus of the ear. This vessel is biopsied in suspected temporal (giant cell) arteritis - the most common vasculitis of adults >50 years. It is used for extracranial-intracranial (EC-IC) bypass surgery.
8. Maxillary Artery (Terminal Branch - Largest)
Origin: Larger terminal branch of ECA; arises posterior to the neck of the mandible within the parotid gland, medial to the superficial temporal artery.
Course - divided into 3 parts:
| Part | Location | Key Landmark |
|---|---|---|
| 1st (Mandibular) | Behind neck of mandible | Between mandible and sphenomandibular ligament |
| 2nd (Pterygoid) | In infratemporal fossa | Superficial/deep to lateral pterygoid muscle |
| 3rd (Pterygomaxillary) | In pterygopalatine fossa | Through pterygomaxillary fissure |
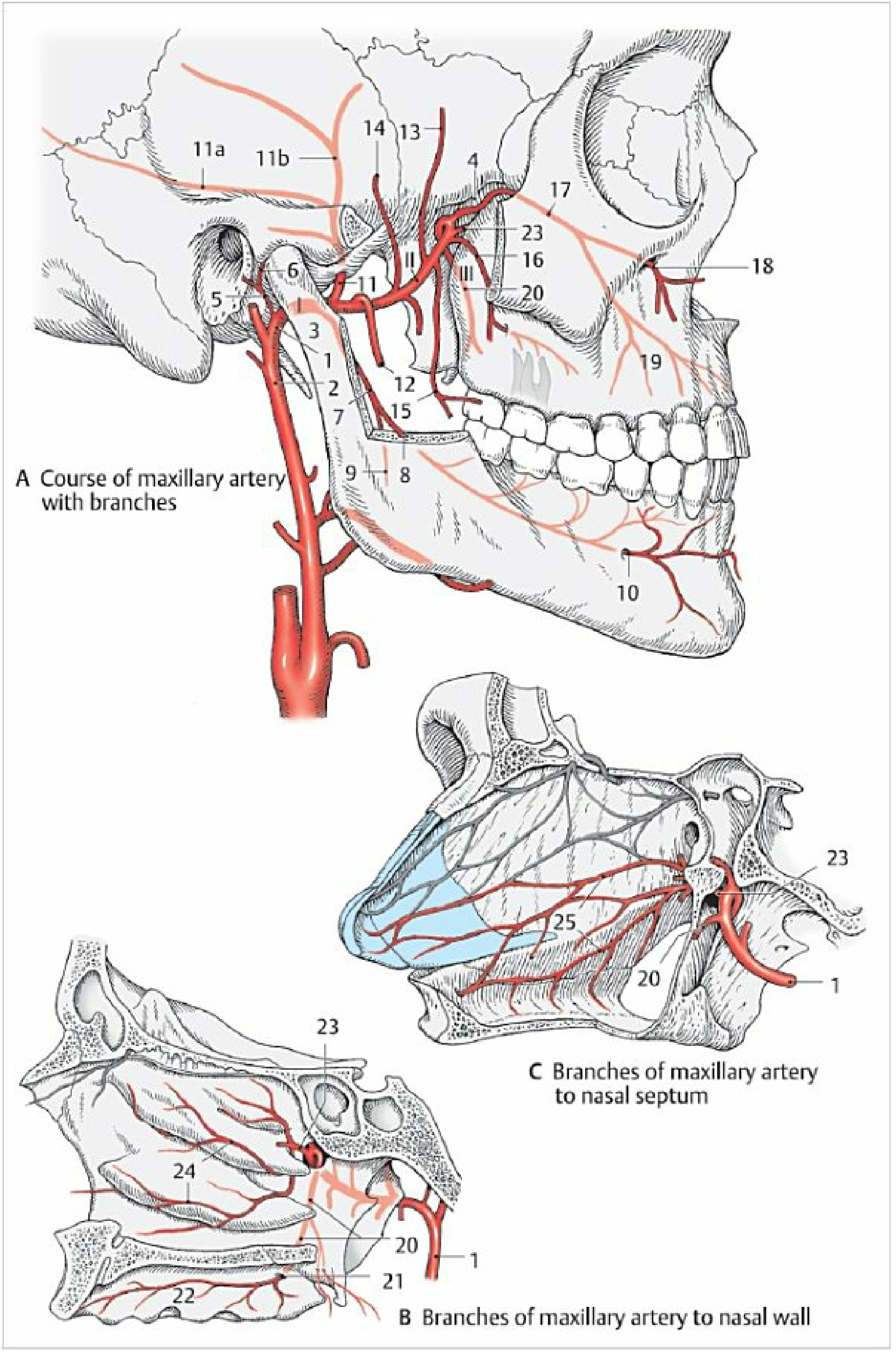
Fig. 2.22 - Maxillary artery course and branches (Color Atlas of Human Anatomy, Vol. 2)
Branches of the Maxillary Artery:
From 1st (Mandibular) Part - Mnemonic: "DAIIM"
- Deep auricular artery - TMJ, external acoustic meatus, tympanic membrane
- Anterior tympanic artery - tympanic cavity (via petrotympanic fissure)
- Inferior alveolar artery - enters mandibular canal, gives mylohyoid branch before entry, supplies mandibular teeth, terminates as mental artery (exits mental foramen)
- Middle meningeal artery - passes through foramen spinosum, largest artery to dura mater; divides into frontal (anterior) and parietal (posterior) branches; runs in epidural space
Clinical: Middle meningeal artery injury = extradural (epidural) hematoma - "lucid interval" then rapid deterioration. The frontal branch marks the pterion (thinnest skull point).
From 2nd (Pterygoid) Part - Mnemonic: "MADABB"
- Masseteric artery - to masseter
- Anterior and posterior deep temporal arteries - to temporalis muscle
- Pterygoid branches - to pterygoid muscles
- Buccal artery - to buccinator and buccal mucosa (anastomoses with facial artery)
From 3rd (Pterygomaxillary) Part - Mnemonic: "PIAGDS"
- Posterior superior alveolar artery - upper molar and premolar teeth, maxillary sinus
- Infraorbital artery - through inferior orbital fissure, infraorbital canal, infraorbital foramen; gives anterior superior alveolar arteries (upper incisors and canines); supplies lower eyelid, cheek, upper lip
- Greater palatine (descending palatine) artery - through greater palatine canal; greater palatine artery to hard palate; lesser palatine arteries to soft palate
- Artery of pterygoid canal (Vidian artery) - to auditory tube and upper pharynx
- Sphenopalatine artery (terminal branch) - through sphenopalatine foramen; posterior lateral nasal arteries and posterior septal branches; anastomoses in Little's area (Kiesselbach's plexus) on nasal septum
Clinical: The sphenopalatine artery is the most common source of posterior epistaxis. Little's area (Kiesselbach's plexus) is the commonest site of anterior epistaxis, where anastomoses from the facial, maxillary (sphenopalatine + greater palatine), and ophthalmic (anterior ethmoidal) arteries converge.
Summary Table: Branches of the ECA
(Gray's Anatomy for Students, p. 1152)
| Branch | Origin (Surface) | Main Supply |
|---|---|---|
| Superior thyroid a. | Anterior | Thyroid, larynx |
| Ascending pharyngeal a. | Medial/Posterior | Pharynx, palate, meninges |
| Lingual a. | Anterior | Tongue, sublingual gland |
| Facial a. | Anterior | Face, tonsil, submandibular gland |
| Occipital a. | Posterior | Posterior scalp, SCM, meninges |
| Posterior auricular a. | Posterior | Ear, mastoid, scalp |
| Superficial temporal a. | Terminal | Lateral scalp, face |
| Maxillary a. | Terminal | Deep face, teeth, dura, nose, palate |
PART 2: INTERNAL CAROTID ARTERY (ICA)
Origin and Course
The ICA arises from the CCA at the upper border of the thyroid cartilage (C3-C4 level). It gives NO branches in the neck. It ascends in the carotid sheath, enters the skull through the carotid canal in the petrous temporal bone, and ultimately terminates by dividing into the anterior cerebral artery (ACA) and middle cerebral artery (MCA).
Key fact: The ICA lies posterolateral to the ECA at its origin, then passes medial to ECA as it ascends.
Segments of the ICA
The ICA is divided into 4 classic segments (or 7 by Bouthillier classification):
| Segment | Location | Branches |
|---|---|---|
| C1 - Cervical | Neck, from bifurcation to carotid canal | None |
| C2 - Petrous | Within carotid canal in petrous temporal bone | Caroticotympanic arteries, Vidian artery (artery of pterygoid canal) |
| C3 - Cavernous | Within cavernous sinus (carotid siphon - S-shaped) | Meningohypophyseal trunk (tentorial artery, inferior hypophyseal artery, dorsal meningeal artery); Artery of inferior cavernous sinus; Capsular artery |
| C4 - Supraclinoid/Cerebral | After piercing dura at anterior clinoid process - intracranial | All major branches (see below) |
ICA Angiogram - Segments Labeled
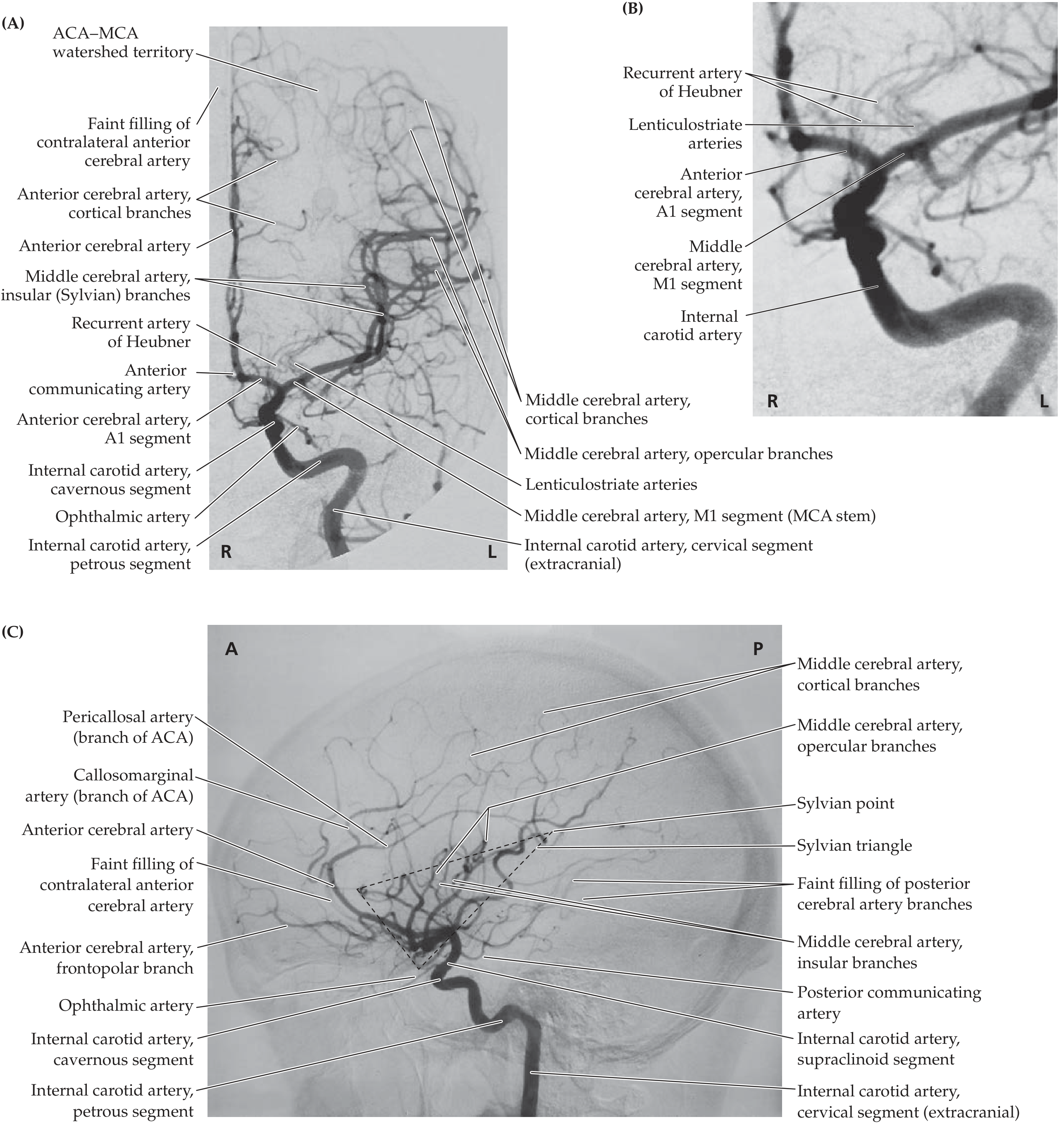
Angiographic images of the anterior circulation showing ICA segments and terminal branches (Neuroanatomy through Clinical Cases, 3rd Edition)
Relations of the ICA in the Neck (Cervical Segment)
- Anterolaterally: ECA, hypoglossal nerve (CN XII)
- Posteriorly: Sympathetic chain, superior cervical ganglion
- Medially: Pharynx and superior laryngeal nerve
- Contents of carotid sheath: ICA (anteriorly), internal jugular vein (posterolaterally), vagus nerve (CN X) (between and behind both)
The Cavernous Segment and Carotid Siphon
Within the cavernous sinus, the ICA forms an S-shaped curve known as the carotid siphon. The cavernous sinus contains (from medial to lateral in the wall):
- CN III (oculomotor)
- CN IV (trochlear)
- CN V1 (ophthalmic division)
- CN V2 (maxillary division)
- CN VI (abducens) - lies directly adjacent to ICA
Clinical: Cavernous sinus thrombosis causes ophthalmoplegia (CN III, IV, VI palsy), proptosis, and pain (CN V1/V2). An ICA aneurysm in the cavernous sinus may compress CN VI first (closest to artery).
Terminal Branches of the ICA (Supraclinoid Segment)
After piercing the dura medial to the anterior clinoid process, the ICA gives off these branches in order:
1. Ophthalmic Artery
- First and most important branch of the supraclinoid ICA
- Arises at the level of the anterior clinoid process
- Enters the orbit through the optic canal alongside the optic nerve (CN II)
- Initially inferior and lateral to optic nerve, then crosses over it superiorly and runs on its medial side
Branches of the Ophthalmic Artery:
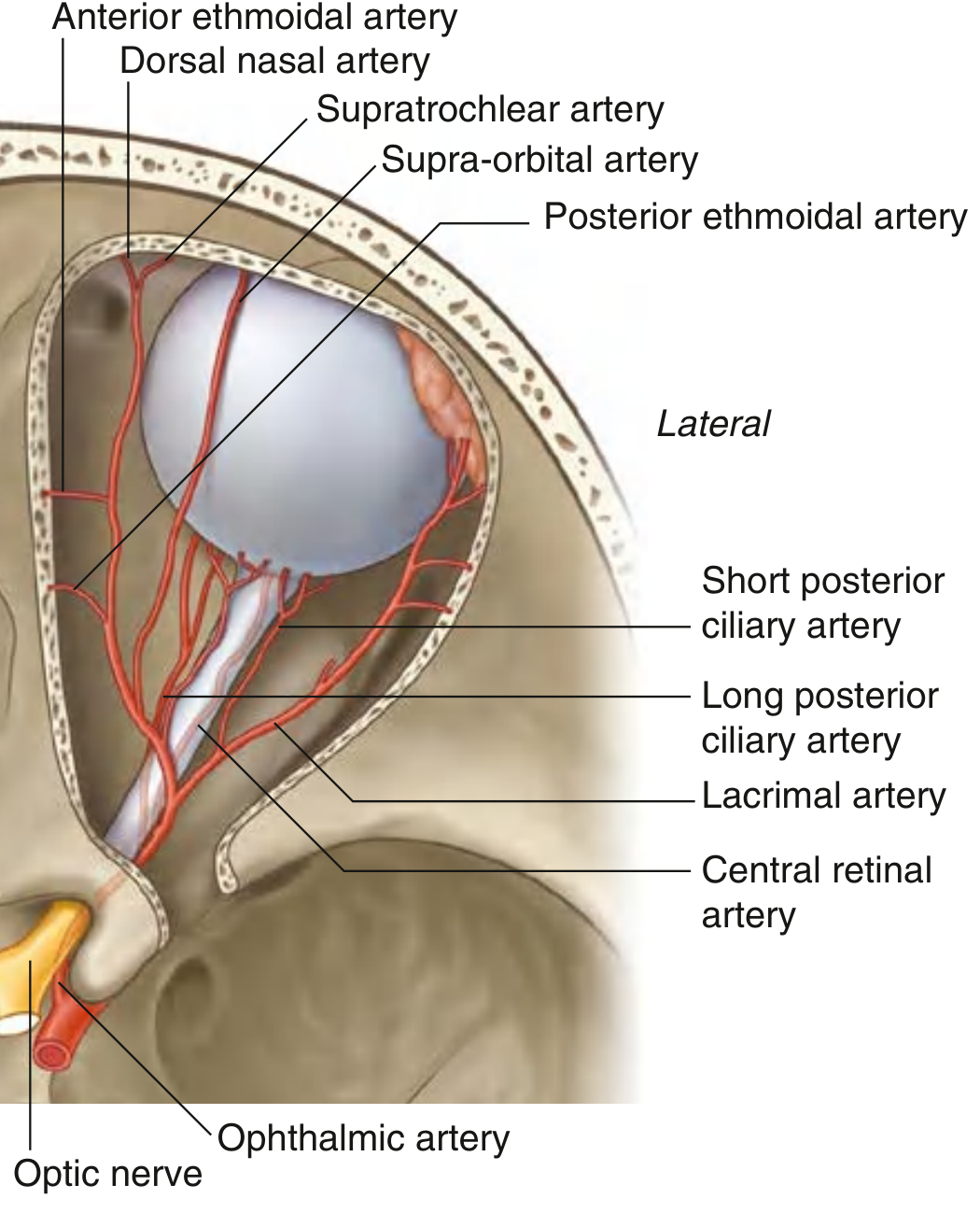
Fig. 8.102 - Arterial Supply to the Orbit and Eyeball (Gray's Anatomy for Students)
| Branch | Supply |
|---|---|
| Central retinal artery | Enters optic nerve; only supply to inner 2/3 retina; visible on fundoscopy |
| Lacrimal artery | Lacrimal gland, lateral eyelids |
| Long posterior ciliary arteries (x2) | Iris, ciliary body (anterior uvea) |
| Short posterior ciliary arteries (x6-10) | Choroid, outer retina |
| Supra-orbital artery | Exits supra-orbital foramen; forehead, scalp to vertex |
| Anterior ethmoidal artery | Enters anterior ethmoidal foramen; ethmoidal cells, frontal sinus, nasal cavity (septum + lateral wall) |
| Posterior ethmoidal artery | Ethmoidal cells, nasal cavity roof |
| Medial palpebral arteries | Medial eyelids |
| Dorsal nasal artery (terminal) | Bridge of nose; anastomoses with facial artery |
| Supratrochlear artery (terminal) | Forehead, scalp; anastomoses with facial artery |
Clinical: Occlusion of the central retinal artery = sudden, painless, complete monocular blindness ("like a curtain falling"). This is an ophthalmological emergency. The ophthalmic artery anastomoses with ECA branches (facial, maxillary) = collateral pathway in ICA occlusion.
2. Posterior Communicating Artery (PCoA)
- Arises from the posterior wall of the ICA
- Runs posteriorly to join the posterior cerebral artery (PCA) - connecting anterior and posterior circulations (forms part of the Circle of Willis)
- Perforating branches: Supply anterior hypothalamus, optic tract, posterior optic chiasm, anterior thalamus
Clinical: A PCoA aneurysm is the most common aneurysm to cause a CN III (oculomotor) palsy - classically a "surgical third nerve palsy" with ptosis, dilated/fixed pupil, and eye looking "down and out." The pupil is involved because the pupillary fibres run on the outside of CN III.
3. Anterior Choroidal Artery (AChA)
- Arises from the posterior wall of ICA, distal to PCoA
- Courses posterolaterally along the optic tract to reach the choroidal fissure
- Supply (vast and clinically important):
- Choroid plexus of the temporal (inferior) horn
- Hippocampus and amygdala
- Optic tract
- Posterior limb of the internal capsule (genu and posterior 2/3)
- Globus pallidus
- Lateral geniculate body (origin of optic radiations)
- Tail of the caudate nucleus
- Substantia nigra
- Cerebral peduncle (middle third)
Clinical: AChA infarct = contralateral hemiplegia + hemianesthesia + homonymous hemianopia (the "three H's"). This is called the anterior choroidal artery syndrome. Small vessel but huge territory.
4. Terminal Bifurcation: Anterior Cerebral Artery (ACA) + Middle Cerebral Artery (MCA)
The ICA terminates by dividing into the ACA and MCA at the medial end of the lateral cerebral sulcus (Sylvian fissure).
Circle of Willis (Circulus Arteriosus)
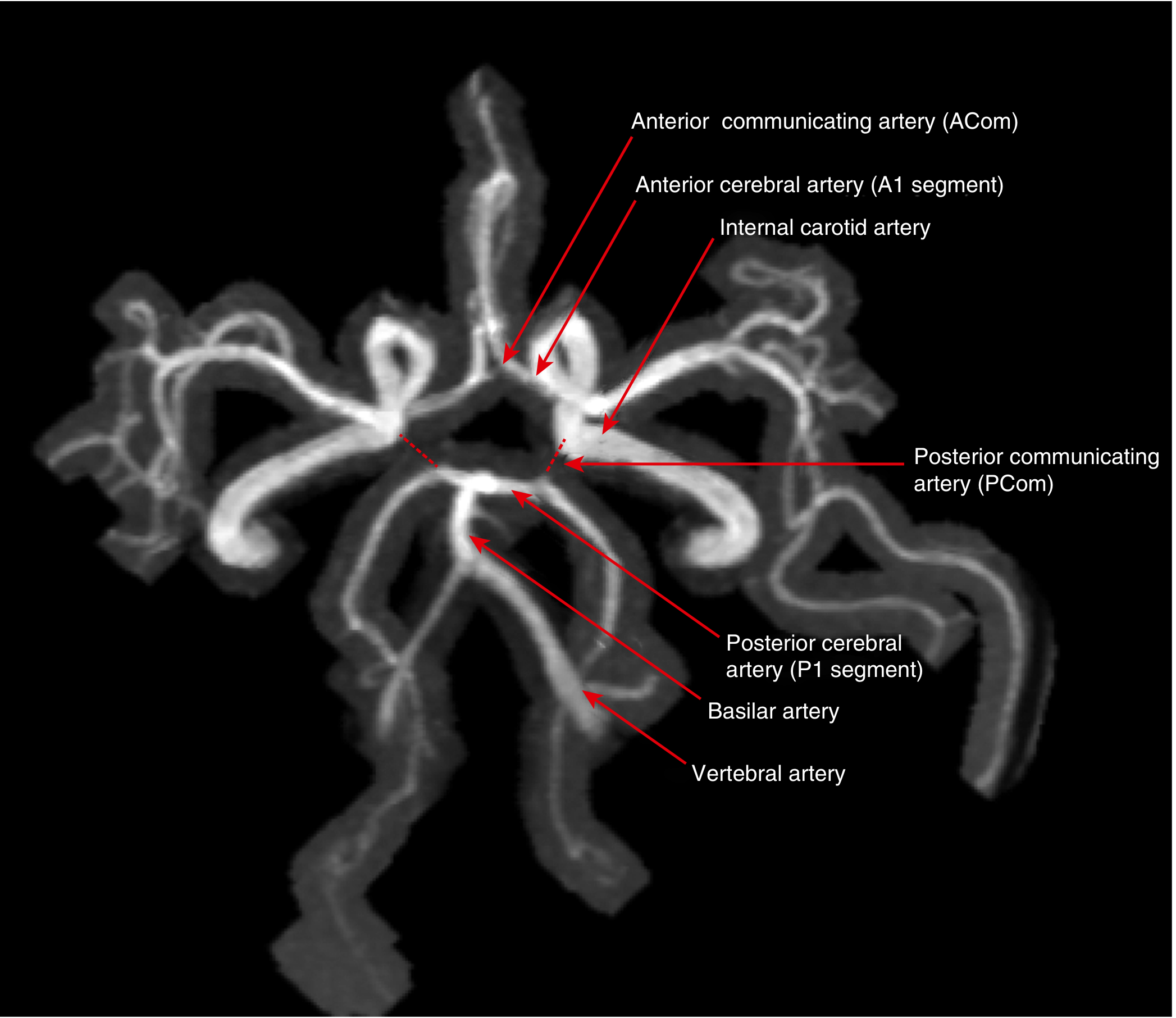
MR angiogram of the Circle of Willis (Goldman-Cecil Medicine)
The Circle of Willis is an arterial anastomotic ring at the base of the brain providing collateral circulation:
| Component | Artery |
|---|---|
| Anterior part | Anterior communicating artery (ACoA) + ACA (A1 segments) |
| Lateral parts | ICA (both sides) |
| Posterior part | PCA (P1 segments) + Posterior communicating arteries (PCoA) + Basilar artery |
Anatomical variations are common - a complete circle is present in only ~20-25% of people. The most common variant is a hypoplastic or absent PCoA.
Summary Table: ICA Segments and Branches
| Segment | Branches | Clinical Relevance |
|---|---|---|
| Cervical (C1) | None | Carotid stenosis, dissection |
| Petrous (C2) | Caroticotympanic, Vidian | Petrous apex lesions |
| Cavernous (C3) | Meningohypophyseal trunk, inferior cavernous sinus a. | Cavernous sinus thrombosis, CN VI palsy |
| Supraclinoid (C4) | Ophthalmic a., PCoA, AChA, ACA, MCA | Stroke, aneurysm |
KEY CLINICAL CORRELATIONS
| Clinical Scenario | Artery Involved |
|---|---|
| Extradural hematoma | Middle meningeal artery (1st part maxillary a.) |
| Posterior epistaxis | Sphenopalatine artery |
| Anterior epistaxis (Kiesselbach's plexus) | Facial + maxillary + ophthalmic anastomosis |
| Tonsillectomy bleeding | Tonsillar branch of facial artery |
| Temporal arteritis (biopsy site) | Superficial temporal artery |
| Sudden monocular blindness | Central retinal artery (ophthalmic branch) |
| Surgical CN III palsy with pupil dilation | Posterior communicating artery aneurysm |
| Contralateral hemiplegia + hemianopia | Anterior choroidal artery infarct |
| Horner's syndrome in neck | Sympathetic chain alongside cervical ICA |
| Carotid body tumor | CCA bifurcation/ECA origin |
QUICK EXAM REVISION
ECA distinguishing features (from ICA at bifurcation):
- Lies anteromedial to ICA at origin
- Gives branches in the neck (ICA gives none)
- Smaller caliber than ICA
- Has no carotid sinus
- Occluded by compressing the ECA branches on the scalp
ICA distinguishing features:
- No branches in the neck
- Larger caliber
- Lies posterolateral to ECA at origin, then medial
- Has carotid sinus (baroreceptor) at its origin
- Enters the skull via the carotid canal
Sources: Gray's Anatomy for Students (9780323934237); Color Atlas of Human Anatomy Vol. 2 (9783132424487); Localization in Clinical Neurology 8e (9781975160241); Goldman-Cecil Medicine (9780323930345); Neuroanatomy through Clinical Cases 3rd Ed. (9781605359625); Scott-Brown's Otorhinolaryngology Vol. 1 (9781138094611)
This is a shared conversation. Sign in to Orris to start your own chat.