Describe the etiopathogenesis, diagnosis, management and prevention of rheumatic fever.
Reading File
Finding Sources
Searching PubMed
"rheumatic fever"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Searching Images
Aschoff body rheumatic fever carditis histology
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive material from multiple authoritative sources. Here is the complete answer:
Rheumatic Fever
"Rheumatic fever licks the joints but bites the heart." — Ernest-Charles Lasègue, 1884
1. Etiopathogenesis
The Agent: Group A β-Hemolytic Streptococcus (GAS)
Acute rheumatic fever (ARF) is a multisystem inflammatory disease that arises exclusively after pharyngeal (not skin) infection with Streptococcus pyogenes (Group A β-hemolytic Streptococcus). The attack rate from untreated GAS pharyngitis ranges from <1% to 3%, rising with certain rheumatogenic M-protein serotypes (mucoid types 3, 5, 18) and a stronger host immune response.
Key streptococcal virulence factors:
- M protein — the primary rheumatogenic determinant; its N-terminal domain contains epitopes that cross-react with human cardiac tissue
- Streptolysins O and S — tissue-damaging exotoxins; ASO antibody is an important serological marker
- Hyaluronic acid capsule — inhibits phagocytosis
- Streptokinase, DNase B, hyaluronidase — facilitate tissue invasion
The Host
- ARF primarily affects children aged 5–15 years
- There is a genetic predisposition: only 3–6% of any population is susceptible
- HLA class II alleles (DR4, DR7, DR2) are associated with susceptibility
- Women develop rheumatic heart disease (RHD) ~1.8× more often than men, likely due to greater GAS exposure through child rearing and hormonal factors
The Environment
Overcrowding, poverty, malnutrition, and poor access to healthcare facilitate streptococcal transmission and reduce opportunities for early treatment — the primary drivers of the disease's concentration in low- and middle-income countries.
Pathogenesis: Molecular Mimicry
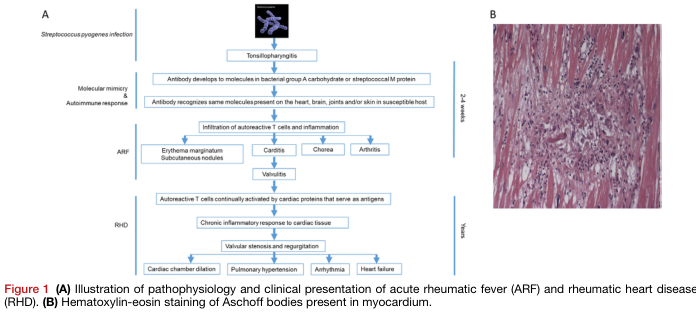
The central mechanism is molecular mimicry — structural similarities between GAS antigens and human proteins trigger a misdirected immune response:
- GAS pharyngitis → immune response generates antibodies and T cells against streptococcal antigens (particularly M protein and Group A carbohydrate)
- These antibodies cross-react with host tissue antigens in the heart, joints, brain, and skin because of shared epitopes
- Autoreactive CD4+ T cells infiltrate target organs; antibodies activate complement and mediate tissue injury
Organ-specific mechanisms:
| Manifestation | Mechanism |
|---|---|
| Carditis | Antibody binding + T-cell infiltration of all three cardiac layers (pericarditis, myocarditis, endocarditis/valvulitis); mitral valve most affected |
| Arthritis | Immune complex deposition in synovium → sterile inflammatory effusion |
| Chorea | Antibodies cross-react with basal ganglia neurons (caudate nucleus) |
| Erythema marginatum | Delayed hypersensitivity reaction in dermal vessels |
| Subcutaneous nodules | Granulomatous inflammation at bony prominences |
Pathological Features
Aschoff bodies are the pathognomonic lesion of rheumatic carditis — perivascular granulomas containing:
- Aschoff cells (activated macrophages with large, "owl-eye" nucleoli)
- Anitschkow cells (caterpillar cells — elongated nuclei with chromatin bars)
- Surrounding lymphocytes and plasma cells
The endocarditis produces small verrucous vegetations along the valve closure line, predominantly on the mitral valve (mitral regurgitation acutely → mitral stenosis from fibrosis and calcification over years). The aortic valve is the second most commonly involved.
2. Clinical Manifestations
ARF develops 2–4 weeks after GAS pharyngitis (the "latent period"), with symptoms lasting 2–6 weeks. The cardinal features, with approximate frequencies in initial attacks:
| Feature | Frequency |
|---|---|
| Fever (>38.5°C) | >90% |
| Migratory polyarthritis | 60–75% |
| Carditis (clinical) | >50% |
| Sydenham chorea | ~30% |
| Erythema marginatum | <10% |
| Subcutaneous nodules | <10% |
Key clinical points:
- Arthritis: Migratory, fleeting, predominantly large joints (knees, ankles, elbows, wrists); pain out of proportion to signs; responds dramatically to NSAIDs (failure to respond should prompt alternative diagnosis); sterile synovial fluid with lymphocyte predominance
- Carditis (pancarditis): Tachycardia out of proportion to fever, new murmurs (mitral/aortic regurgitation), pericardial rub, cardiomegaly, or heart failure; subclinical carditis detectable only by echocardiography is now recognised
- Chorea (Sydenham's chorea / St. Vitus' dance): Involuntary, non-rhythmic, purposeless movements; more pronounced on one side; disappears during sleep; may appear months after pharyngitis, sometimes without other features
- Erythema marginatum: Pink, non-pruritic, blanching macules/papules spreading in a serpiginous pattern on trunk and proximal limbs
- Subcutaneous nodules: 0.5–2 cm, painless, over bony prominences or extensor tendons; almost always associated with carditis
3. Diagnosis
No single definitive test exists — ARF is a clinical diagnosis of exclusion.
Evidence of Preceding GAS Infection (Required)
- Throat culture positive for GAS (often negative by the time ARF presents)
- Rapid antigen detection test
- Elevated/rising streptococcal antibody titers: ASO (most common), anti-DNase B (more sensitive in skin infections and 2–4 weeks after pharyngitis), antistreptokinase, antihyaluronidase
- History of scarlet fever
Revised Jones Criteria (2015 AHA)
The diagnosis requires evidence of preceding GAS infection plus:
- 2 major criteria, OR
- 1 major + 2 minor criteria
(For recurrent ARF: 2 major, or 1 major + 2 minor, or 3 minor criteria)
Major Criteria:
| Low-Risk Populations | Moderate/High-Risk Populations |
|---|---|
| Carditis (clinical and/or subclinical echocardiographic valvulitis) | Same |
| Polyarthritis | Monoarthritis or polyarthritis |
| Chorea | Same |
| Erythema marginatum | Same |
| Subcutaneous nodules | Same |
Minor Criteria:
| Low-Risk | Moderate/High-Risk |
|---|---|
| Polyarthralgia | Monoarthralgia |
| Fever ≥38.5°C | Fever ≥38.5°C |
| ESR ≥60 mm/hr and/or CRP ≥3.0 mg/dL | ESR ≥30 mm/hr and/or CRP ≥3.0 mg/dL |
| Prolonged PR interval (unless carditis is a major criterion) | Same |
Low-risk populations: ARF incidence <2/100,000 school-age children/year or RHD prevalence ≤1/1,000/year.
Supporting Investigations
- ECG: Prolonged PR interval (first-degree AV block); not specific
- Echocardiography (2D + Doppler): Now integral to diagnosis — detects subclinical valvulitis (regurgitation without audible murmur), assesses severity; obtain in all suspected cases
- Inflammatory markers: ESR, CRP, leukocytosis; normochromic normocytic anaemia
- Synovial fluid: Sterile, inflammatory (lymphocyte predominance)
Differential Diagnosis
Juvenile idiopathic arthritis, reactive arthritis, infective endocarditis, viral myocarditis, SLE, serum sickness, Lyme disease
4. Management
General Measures
- Hospitalisation is recommended during the acute phase for diagnosis confirmation and monitoring of cardiac status
- Bed rest — especially with carditis; activity restriction proportional to severity
- Serial echocardiography for carditis
A. Eradication of GAS (Antibiotic Treatment)
All patients receive antibiotics to eliminate residual streptococcal infection, even if throat culture is negative:
| Drug | Dose | Route/Duration |
|---|---|---|
| Benzathine penicillin G (preferred) | 1.2 million units (<27 kg: 600,000 units) | IM single dose |
| Penicillin V | 500 mg 3× daily | PO × 10 days |
| Amoxicillin | 500 mg twice daily | PO × 10 days |
| Erythromycin/Azithromycin | Erythromycin or clarithromycin 250 mg 2×/day | PO × 10 days (penicillin-allergic) |
B. Anti-Inflammatory Therapy
Arthritis and fever:
- Aspirin: 50–100 mg/kg/day in 4 divided doses (max 4–8 g/day) — first-line, dramatic response
- Naproxen: 10–20 mg/kg/day in 2 divided doses — used in small studies with success
- Continue for 1–2 weeks after all symptoms resolve (not just arthritis)
- Failure to respond to NSAIDs should prompt reconsideration of the diagnosis
Carditis:
- Treat heart failure with standard goal-directed therapy: diuretics, ACE inhibitors/ARBs, fluid restriction, bed rest
- Corticosteroids (e.g., prednisolone/hydrocortisone 1–2 mg/kg/day, tapered over 2–4 weeks): considered in severe carditis; evidence remains limited but may be superior to aspirin in hemodynamically significant valvulitis
- Valve surgery is rarely required acutely; may be indicated for acute rupture of a valve leaflet or refractory heart failure
Chorea:
- Usually resolves spontaneously within weeks to months and does not require treatment
- Severe cases: haloperidol, valproic acid, or carbamazepine may be used
5. Prevention
Primary Prevention (Preventing First Episode of ARF)
Adequate antibiotic treatment of GAS pharyngitis prevents ARF:
- Benzathine penicillin G 1.2 million units IM single dose, OR
- Oral penicillin V for 10 days
Timely treatment must occur within 9 days of symptom onset to reliably prevent ARF.
Secondary Prevention (Preventing Recurrences)
ARF recurs at a rate of 8–10% within 5 years without prophylaxis. Each recurrence risks cumulative cardiac damage. Continuous antibiotic prophylaxis is mandatory:
Preferred regimen:
- Benzathine penicillin G 1.2 million units IM every 3–4 weeks (monthly) — most effective; overcomes compliance issues
Alternative oral regimens (less reliable due to adherence):
- Penicillin V 250 mg twice daily
- Sulfadiazine 0.5 g/day (<30 kg) or 1 g/day (≥30 kg)
- Azithromycin 250 mg daily (penicillin-allergic)
Duration of secondary prophylaxis (AHA recommendations):
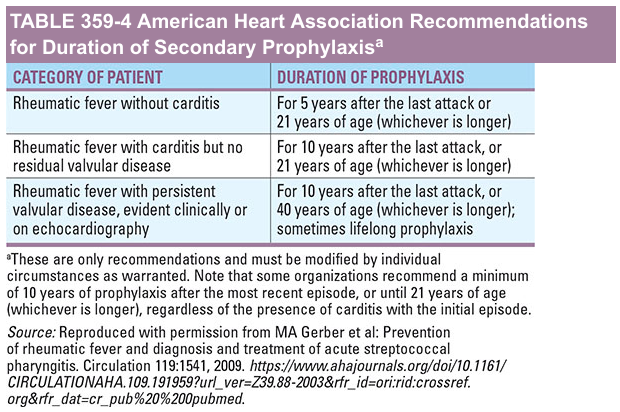
| Category | Duration |
|---|---|
| RF without carditis | 5 years after last attack or age 21 (whichever is longer) |
| RF with carditis but no residual valvular disease | 10 years after last attack or age 21 |
| RF with persistent valvular disease | 10 years after last attack or age 40 (sometimes lifelong) |
Primordial Prevention
Addressing root causes: poverty reduction, improved housing (less overcrowding), better nutrition, access to healthcare, clean water and sanitation. The pre-antibiotic fall in RF incidence in industrialised countries was driven primarily by these socioeconomic improvements, not antibiotics.
Vaccine Development
A GAS vaccine targeting M-protein epitopes is under active development; trials are ongoing, though no licensed vaccine currently exists. This is considered the ultimate tool for eradication of the disease.
6. Prognosis
- 35–70% of patients with acute carditis progress to chronic rheumatic heart disease
- Mitral stenosis is the dominant long-term valvular lesion, typically manifesting 10–20 years after the first ARF episode
- RHD is the leading cause of acquired heart disease in children and young adults in the developing world (~40 million prevalent cases globally), causing 275,000 deaths annually
- Recurrences are the main driver of progressive valve damage; secondary prophylaxis is the most important intervention for altering natural history
Key sources:
- Braunwald's Heart Disease, 12th ed., Ch. 81
- Fuster and Hurst's The Heart, 15th ed., Ch. 27
- Goldman-Cecil Medicine, Table 269-3 (Revised Jones Criteria)
- Tintinalli's Emergency Medicine; Rosen's Emergency Medicine
- Cochrane Review 2024 — Long-term antibiotic prophylaxis for prevention of RF recurrence (PMID 39312290)
- Birru EM et al., 2025 — Adverse reactions to benzathine penicillin G in RHD (PMID 40333929)
This is a shared conversation. Sign in to Orris to start your own chat.