Difference between B and T lymphocytes both physiological and clinical
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
I now have comprehensive information from multiple authoritative textbooks. Let me compile the full, detailed answer.
B Lymphocytes vs T Lymphocytes: Physiological and Clinical Differences
1. Origin and Preprocessing
| Feature | B Lymphocytes | T Lymphocytes |
|---|---|---|
| Common origin | Bone marrow stem cells | Bone marrow stem cells |
| Preprocessing site | Liver (mid-fetal life), then bone marrow (late fetal + post-birth) | Thymus gland |
| Mature in | Bone marrow | Thymus |
| Named after | Bursa (of Fabricius in birds) / Bone marrow | Thymus |
In the thymus, T lymphocytes undergo rapid proliferation and develop diversity for specific antigens. Crucially, up to 90% of developing T cells are destroyed by negative selection - those that react against self-antigens are eliminated before release. B lymphocytes in the bone marrow undergo a parallel process of negative selection against self-antigens. - Guyton and Hall Textbook of Medical Physiology
2. Percentage in Peripheral Blood
-
T cells: 60-80% of circulating lymphocytes
-
B cells: 20-30% of circulating lymphocytes
-
NK cells: 5-15% (neither T nor B)
-
Histology: A Text and Atlas With Correlated Cell and Molecular Biology
3. Surface Markers (CD Markers)
| Marker | B Cells | T Cells |
|---|---|---|
| Pan-marker | CD19, CD20, CD21, CD22 | CD3 (pan-T marker) |
| Specific subsets | CD40, surface Ig (sIg) | CD4 (helper), CD8 (cytotoxic) |
| Receptor | BCR = membrane immunoglobulin | TCR (T-cell receptor) - alpha/beta or gamma/delta |
| Co-receptors | CD40 (interacts with CD154 on T cells) | CD28 (co-stimulation), CD154 (CD40L) |
| MHC restriction | Recognize free/soluble antigen | Recognize antigen only when bound to MHC on APCs |
Although T and B cells cannot be distinguished on the basis of morphology alone, their distinctive CD proteins identify them on immunolabeling. - Histology: A Text and Atlas
4. Antigen Recognition - A Key Physiological Difference
| Feature | B Cells | T Cells |
|---|---|---|
| What they recognize | Free/intact antigen (3D conformational epitopes) | Peptide fragments presented on MHC molecules |
| Presented by | Not required (direct antigen binding) | Antigen-presenting cells (macrophages, dendritic cells, B cells) |
| MHC restriction | None | CD4+ T cells: MHC Class II; CD8+ T cells: MHC Class I |
| Receptor structure | BCR = surface immunoglobulin | TCR = alpha/beta heterodimer (95%) or gamma/delta |
"Although B lymphocytes recognize intact antigens, T lymphocytes respond to antigens only when they are bound to specific molecules called MHC proteins on the surface of antigen-presenting cells." - Guyton and Hall, p.468
5. Subtypes and Their Physiological Functions
T Lymphocyte Subtypes
| Subtype | Marker | Function |
|---|---|---|
| T-helper (Th) | CD4+ | >75% of T cells. Master regulator - secretes lymphokines (IL-2, IL-4, IL-5, IFN-γ, etc.) that activate B cells, macrophages, and CTLs. Subsets: Th1, Th2, Th17, Tfh |
| Cytotoxic T cells (CTL) | CD8+ | Kill virus-infected cells, tumor cells, and allograft cells. Recognize antigen on MHC I. Release perforins and granzymes causing target cell lysis |
| Regulatory T cells (Treg) | CD4+CD25+FOXP3+ | Suppress excessive immune responses. Prevent autoimmunity. Important in tumor immunology and tolerance |
| γδ T cells | TCR γδ | Innate-like function; found especially in gut and skin; respond to non-peptide antigens |
B Lymphocyte Subtypes
| Subtype | Function |
|---|---|
| Naive B cells | Circulate in follicles; not yet antigen-activated |
| Plasma cells | Terminally differentiated B cells; secrete large amounts of antibody (>2000 Ig molecules/second) |
| Memory B cells | Long-lived; responsible for rapid secondary immune response |
| Regulatory B cells (Breg) | Secrete IL-10; suppress inflammatory responses |
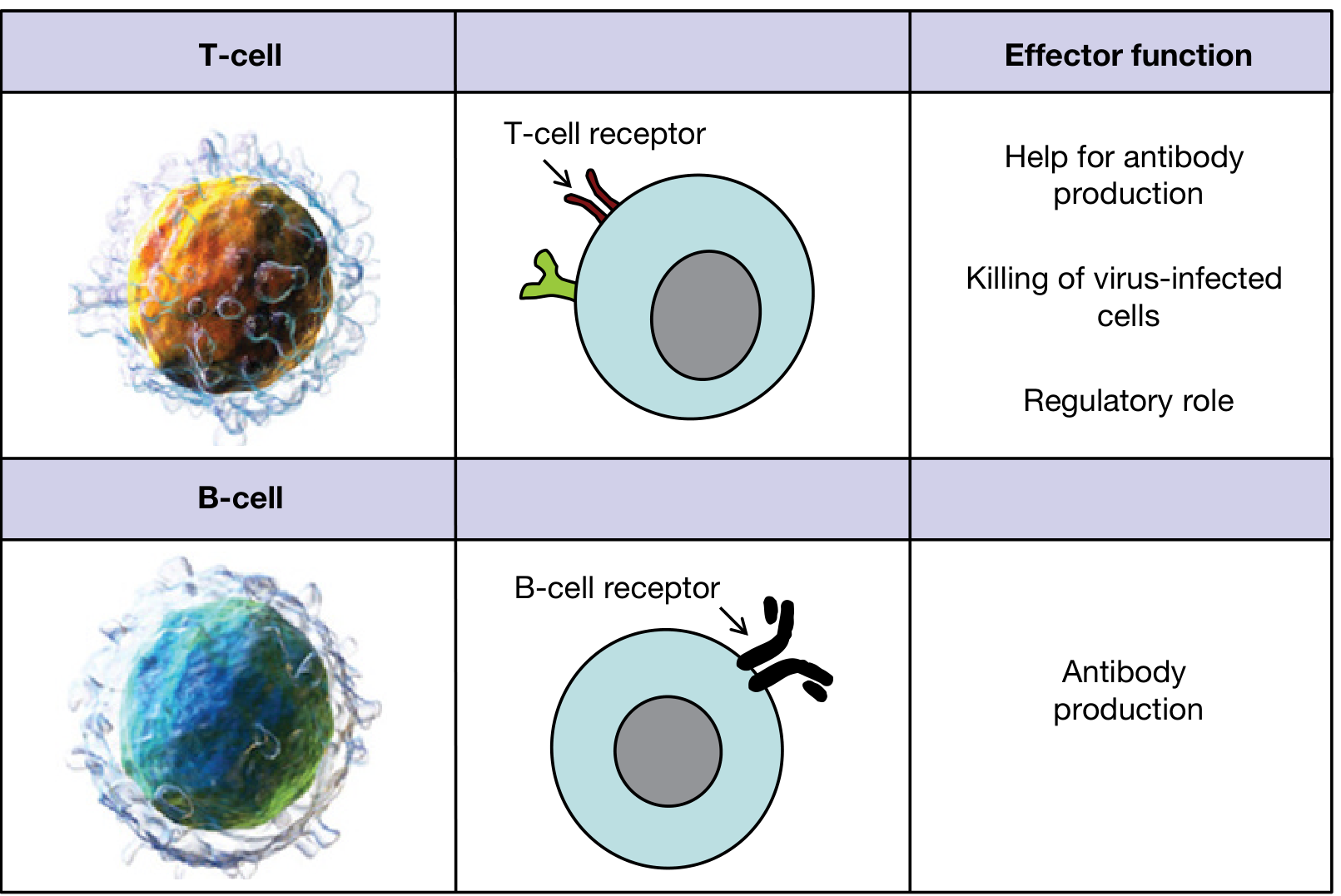
6. Effector Mechanisms
| Feature | B Cells | T Cells |
|---|---|---|
| Type of immunity | Humoral (antibody-mediated) | Cell-mediated |
| Effector product | Antibodies (IgM, IgG, IgA, IgE, IgD) | Activated T cells released into lymph + circulation |
| Target | Extracellular pathogens, toxins, soluble antigens | Intracellular pathogens, viruses, tumor cells, transplanted tissues |
| Memory | Long-lived memory B cells | Long-lived memory T cells |
| Secondary response | Faster, higher-affinity antibodies (class switching) | Faster, larger expansion of antigen-specific T cells |
"The principal difference is that instead of releasing antibodies, whole activated T cells are formed and released into the lymph... circulate again and again throughout the body, sometimes lasting months or even years." - Guyton and Hall, p.467
7. Anatomic Location in Lymph Nodes
- B cells reside in follicles in the cortex. Primary follicles = naive B cells. Secondary follicles with germinal centers = activated B cells undergoing somatic hypermutation and affinity maturation
- T cells reside in the paracortical cords (deep cortex / T-cell zone), packed around high endothelial venules (HEVs). ~70% are CD4+, ~30% CD8+
Their segregation is maintained by chemokines - CXCL13 (by follicular dendritic cells) attracts B cells; CCL19/CCL21 (by fibroblastic reticular cells) attract T cells. - Cellular and Molecular Immunology, p.112-115
8. Interaction Between B and T Cells
B cells require T-cell help (for T-dependent antigens) to undergo:
- Class switch recombination (IgM → IgG/IgA/IgE)
- Affinity maturation in germinal centers
- Memory cell formation
This help is provided by follicular helper T cells (Tfh) through CD40L-CD40 interaction and secretion of IL-21, IL-4. T-independent antigens (e.g., polysaccharides) can activate B cells without T-cell help but produce only IgM and no memory.
9. Clinical Differences (Immunodeficiency Patterns)
This table from Cellular and Molecular Immunology summarizes the clinical pattern perfectly:
| Feature | B Cell Deficiency | T Cell Deficiency |
|---|---|---|
| Infections | Pyogenic bacteria (otitis, pneumonia, meningitis, osteomyelitis), enteric bacteria/viruses, some parasites | Pneumocystis jirovecii, viruses, fungi, intracellular bacteria, protozoa |
| Organisms missed | Encapsulated organisms (Strep. pneumoniae, H. influenzae, Neisseria) | Intracellular pathogens, herpesviruses, CMV, EBV, Candida |
| Example diseases | X-linked agammaglobulinemia (Bruton's), Common Variable Immunodeficiency (CVID), IgA deficiency, Hyper-IgM syndrome | DiGeorge syndrome, SCID (T-cell component) |
| Diagnosis | Low serum Ig, absent B cells on flow cytometry, poor antibody responses to vaccination | Reduced blood T cells, poor lymphoproliferative response to PHA, absent DTH reactions, absent TRECs on neonatal screen |
| Age of onset | After 6 months (maternal IgG wanes) | Infancy (shortly after birth) |
| Cancer risk | Lymphoma (EBV-associated) | EBV-related lymphoma, HPV-associated cancers |
- Cellular and Molecular Immunology, Table 21.1, pp.1362-1363
10. Key Clinical Diseases Linked to Each
B Cell-Associated Clinical Conditions
- X-linked agammaglobulinemia (Bruton's): Absent B cells due to BTK mutation; recurrent bacterial infections after 6 months
- Common Variable Immunodeficiency (CVID): B cells present but fail to differentiate into plasma cells; low IgG/IgA/IgM
- Hyper-IgM syndrome: Defect in CD40L (T cells) or CD40 (B cells) - impairs class switching; elevated IgM, absent IgG/IgA/IgE
- Multiple myeloma: Malignant plasma cell proliferation
- B-cell ALL/CLL: Malignancies of B-cell lineage (CD19+, CD20+, CD10 in precursor B-ALL)
T Cell-Associated Clinical Conditions
- DiGeorge syndrome: Thymic aplasia → absent T cells → viral/fungal infections; associated with 22q11 deletion
- SCID: Combined loss of T and B function (often due to ADA or γ-chain deficiency); screened by TRECs at birth
- AIDS (HIV): Selective destruction of CD4+ T helper cells → CD4 count <200/µL defines AIDS; susceptibility to Pneumocystis, CMV, toxoplasma
- T-cell ALL: Malignancy of T-cell precursors (CD3+, CD7+, TdT+)
- Autoimmune diseases: Failure of Treg function or T-cell tolerance (e.g., Type 1 DM, MS, SLE)
11. Quick Summary Table
| Parameter | B Lymphocytes | T Lymphocytes |
|---|---|---|
| Processing site | Bone marrow (liver in fetus) | Thymus |
| % in blood | 20-30% | 60-80% |
| Surface markers | CD19, CD20, sIg | CD3, CD4 or CD8 |
| Receptor | BCR (immunoglobulin) | TCR (alpha/beta or gamma/delta) |
| Antigen recognition | Free/intact antigen | Peptide + MHC complex |
| Effector product | Antibodies (humoral immunity) | Activated T cells (cell-mediated immunity) |
| Main function | Fight extracellular pathogens, toxins | Fight intracellular pathogens, viruses, tumors |
| Location in lymph node | Follicles (cortex) | Paracortex |
| Memory | Yes (memory B cells) | Yes (memory T cells) |
| Deficiency pattern | Recurrent bacterial infections | Opportunistic viral/fungal infections |
| Key clinical disease | Agammaglobulinemia, CVID | DiGeorge, AIDS, SCID |
Sources:
- Guyton and Hall Textbook of Medical Physiology, pp. 462-470
- Cellular and Molecular Immunology (Abbas et al.), pp. 112-115, 1360-1363
- Roitt's Essential Immunology, pp. 37-38
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology, pp. 716-717
This is a shared conversation. Sign in to Orris to start your own chat.