She me st elevation and how to determine
Reading File
Finding Sources
Searching Images
ST elevation ECG criteria determination STEMI
Reading File
Reading File
Loading Image
Reading File
Loading Image
I now have comprehensive content. Let me compile the full answer.
ST Elevation — What It Is and How to Determine It
What Is ST Elevation?
The ST segment is the portion of the ECG between the end of the QRS complex (J point) and the start of the T wave. It normally lies on or near the isoelectric baseline. ST elevation (STE) means the J point and ST segment are displaced upward above the baseline, reflecting acute myocardial injury — or several mimics.
In the context of acute chest pain, ST elevation is considered to represent STEMI (ST-Elevation Myocardial Infarction) until proven otherwise.
— Rosen's Emergency Medicine, p. 1007
How to Measure ST Elevation
- Identify the isoelectric (baseline): Use the TP segment (between the T wave and the next P wave) or the PR segment as your reference.
- Find the J point: The junction where the QRS complex ends and the ST segment begins.
- Measure from the isoelectric line to the J point (or 60–80 ms after the J point for sloping segments).
Diagnostic Thresholds (STEMI criteria)
| Lead Group | Required STE |
|---|---|
| Leads V2–V3 (men ≥40 yrs) | ≥ 2 mm |
| Leads V2–V3 (men <40 yrs) | ≥ 2.5 mm |
| Leads V2–V3 (women) | ≥ 1.5 mm |
| All other leads | ≥ 1 mm in ≥2 contiguous leads |
| V7–V9 (posterior STEMI) | ≥ 0.5 mm |
| V3R–V4R (right ventricular MI) | ≥ 0.5 mm (≥1 mm in men <30 yrs) |
Localization by Lead Territory
The leads showing STE tell you which artery is occluded and which wall is infarcting:
| Territory | Leads with STE | Artery |
|---|---|---|
| Anterior | V1–V4 | LAD |
| Lateral | I, aVL, V5–V6 | LCx |
| Inferior | II, III, aVF | RCA (or LCx) |
| Right ventricular | V3R–V6R | RCA proximal |
| Posterior | V7–V9 (and reciprocal depression V1–V3) | RCA or LCx |
Always check for reciprocal ST depression in the mirror-image leads — its presence strongly supports true STEMI over a mimic.
Example ECG — Anterior STEMI

Prominent convex ST elevation across V1–V6, most marked in V2–V4. This is classic anterior STEMI (LAD occlusion). Note the upwardly convex ("tombstone") morphology.
Example ECG — Inferolateral STEMI
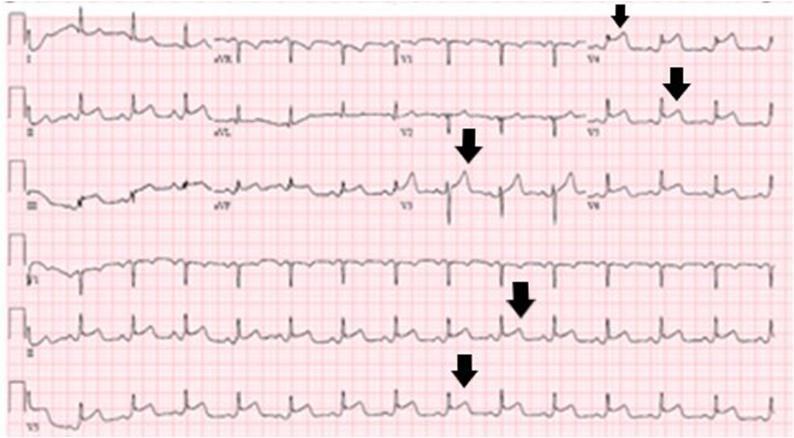
ST elevation in V4–V6 and inferior leads with reciprocal depression in aVL — inferolateral STEMI.
ST Morphology Matters
The shape of the ST segment helps distinguish STEMI from mimics:
| Morphology | Meaning |
|---|---|
| Convex ("tombstone" or "domed") | Strongly suggests STEMI |
| Concave (smiley-face) | More typical of benign causes |
| Obliquely flat | Can be either — be cautious |
Key Differential Diagnosis of ST Elevation
These conditions can all produce STE but are not STEMI:
1. Benign Early Repolarization (BER)
- Concave STE, typically ≤2 mm in precordial leads (V2–V5)
- J-point notching at the terminal QRS
- Large, concordant (upright) T waves
- Stable over time; diffuse distribution
- STE is usually <3.5 mm at the J point
2. Acute Pericarditis
- Diffuse STE in nearly all leads (except aVR, which shows depression)
- Concave-upward ST morphology
- PR segment depression (best seen in II and V6) — insensitive but specific
- PR elevation in aVR is the mirror-image finding
- No reciprocal depression (except aVR)
— Rosen's Emergency Medicine, p. 1007–1008
3. Left Bundle Branch Block (LBBB)
- Rule of appropriate discordance: ST and T waves are normally opposite to the main QRS direction
- In V1–V3: LBBB normally has STE with tall T waves → mimics anterior STEMI
- Use Sgarbossa criteria to detect AMI in LBBB:
- Concordant STE ≥1 mm (same direction as QRS) — most specific
- Concordant ST depression ≥1 mm in V1–V3
- Discordant STE ≥5 mm (less specific; modified criterion uses ≥25% of S-wave depth)
4. Left Ventricular Aneurysm (LVA)
- Regional STE (usually anterior, V1–V4), persistent for weeks/months
- Differentiate from STEMI: if T/QRS ratio <0.36 in all leads, likely LVA rather than acute STEMI
5. Left Ventricular Hypertrophy (LVH)
- Can produce STE in right precordial leads similar to LBBB pattern
- Context and clinical history key
Summary Decision Approach
Chest pain + STE on ECG
↓
Are ≥2 contiguous leads affected at threshold?
↓ Yes
What is the morphology?
→ Convex + regional + reciprocal depression = STEMI → activate cath lab
→ Concave + diffuse + PR depression = Pericarditis
→ Concave + J-point notch + stable = BER
→ LBBB present → apply Sgarbossa criteria
→ Old ECG unchanged + anterior only = consider LV aneurysm
The 12-lead ECG is the pivotal triage tool — it drives the STEMI vs. NSTEMI distinction and determines whether emergent reperfusion (PCI or fibrinolysis) is indicated. — Harrison's Principles of Internal Medicine 22e, p. 1015
This is a shared conversation. Sign in to Orris to start your own chat.