Pathology of lung disease caused by air pollutants Add microscopy & gross picture, add mnemonic if possible
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
I now have all the images and content needed. Let me compose the comprehensive answer.
Pathology of Lung Diseases Caused by Air Pollutants (Pneumoconioses)
Master Mnemonic: "CABSA-B"
Coal workers' pneumoconiosis
Asbestosis
Berylliosis
Silicosis
Anthracosis
Byssinosis (cotton dust)
For remembering what each one does to the lung:
"Coal Slings Arrows at the Lung"
- Coal - upper lobe, macules/nodules, black lung
- Silica - "S"whorled nodules, "S"tone-mason's disease
- Asbestos - All cancers (meso + lung ca), Asbestos bodies, lower lobe first
- Berylliosis - Big granulomas (non-caseating), like sarcoidosis
1. Anthracosis
Source: Carbon particles (urban air pollution, tobacco smoke)
Pathogenesis: Inhaled carbon pigment engulfed by alveolar macrophages → accumulate along pulmonary lymphatics and pleura → no cellular reaction
Gross: Black pigment deposits along lymphatics and in hilar lymph nodes. No palpable nodules. Considered a harmless incidental finding.
Microscopy: Carbon-laden macrophages clustered in peribronchial connective tissue. No fibrosis, no inflammation.
Clinical: Asymptomatic. Found in virtually all urban adults and smokers.
2. Coal Workers' Pneumoconiosis (CWP)
Mnemonic: "Coal Makes Progressive, Massive Fibrosis" (CMF → PMF)
Source: Coal mine dust (carbon + silica + trace metals)
Spectrum: Anthracosis → Simple CWP → Complicated CWP (Progressive Massive Fibrosis)
Pathogenesis
Coal dust particles phagocytosed by alveolar macrophages → inflammasome activation → IL-1, TNF, free radicals → fibroblast proliferation + collagen deposition → lymphatic spread amplifies reaction.
Gross Pathology
Simple CWP: Coal macules (1-2 mm) + larger coal nodules, predominantly upper lobes and upper zones of lower lobes. Centrilobular emphysema may develop.
Complicated CWP / PMF: Multiple, jet-black scars >2 cm (up to 10 cm), dense collagen + pigment:
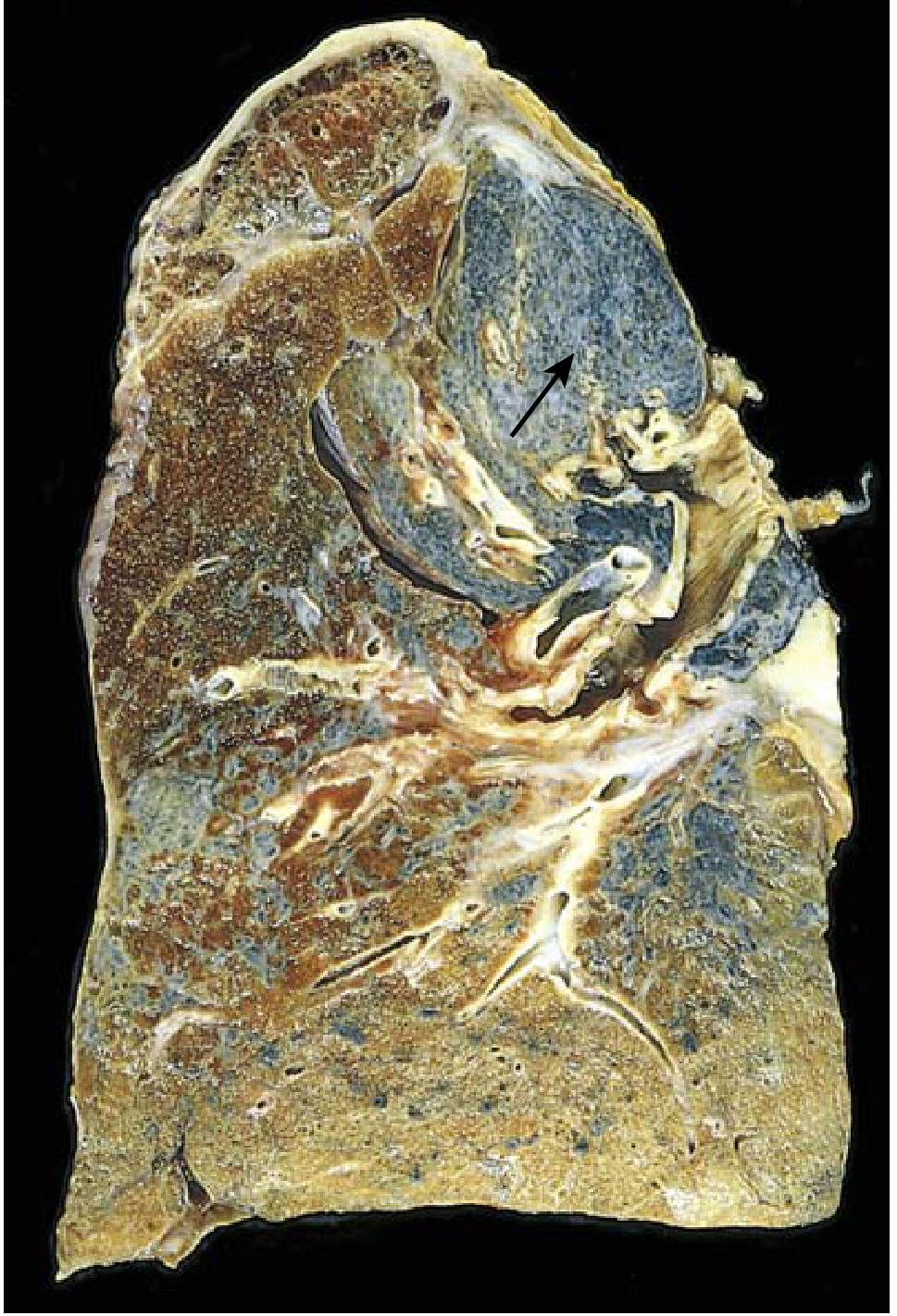
Advanced silicosis/PMF: Scarring has contracted the upper lobe into a small dark mass. Note dense pleural thickening (arrow). - Robbins Pathology
Microscopy
Coal macule: Dust-laden macrophages + delicate network of collagen fibers.
PMF: Dense collagen with black pigment, large confluent scars:
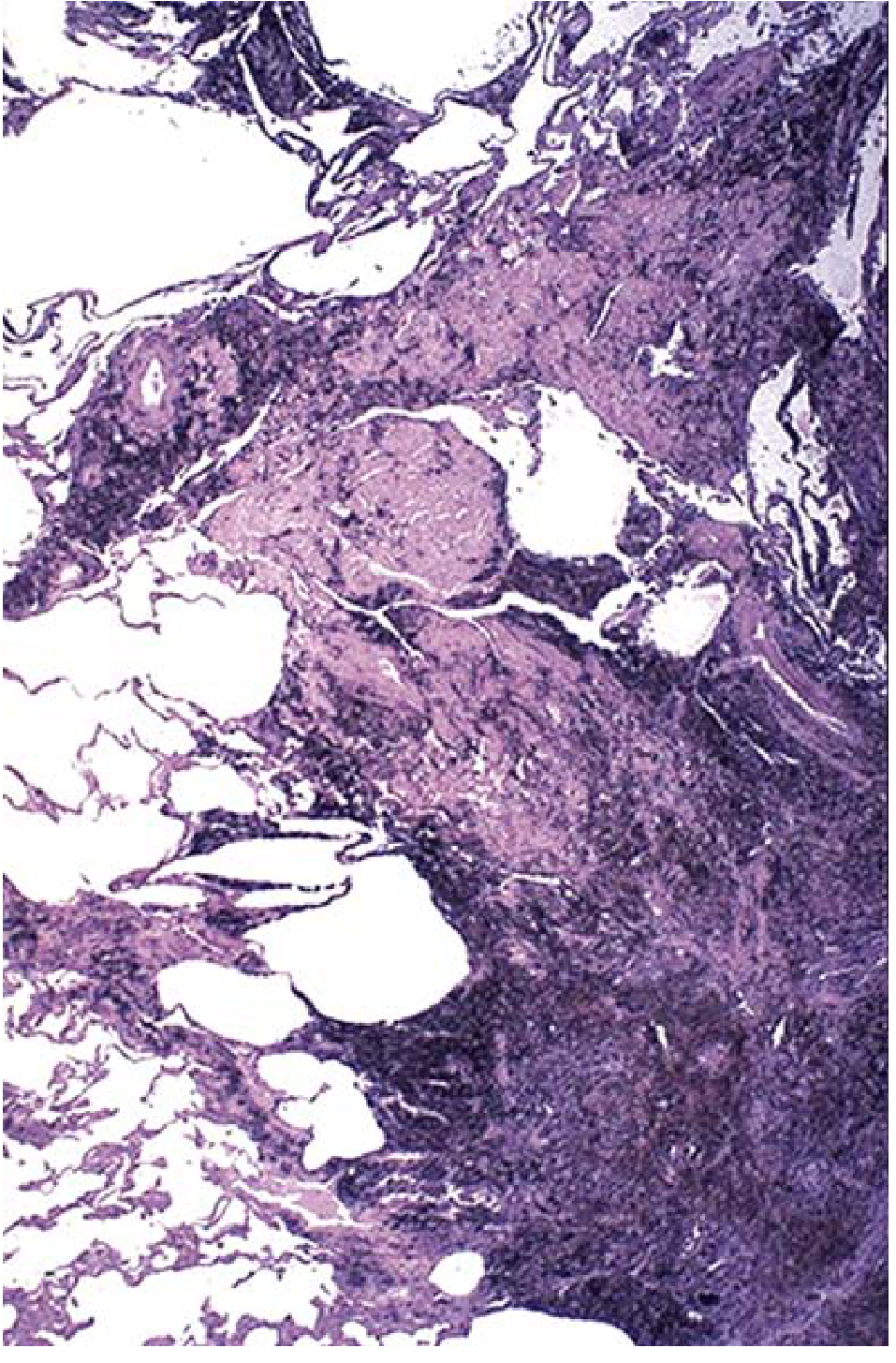
PMF in a coal worker - large amount of black pigment associated with fibrosis. - Robbins Pathology
Clinical
- Simple CWP: benign, minimal lung dysfunction
- PMF: progressive dyspnea, pulmonary hypertension, cor pulmonale
- No increased lung cancer risk (unlike silica/asbestos)
- Caplan syndrome: Pulmonary nodules + rheumatoid arthritis + coal/silica exposure
3. Silicosis
Mnemonic: "Stone SWIRLs in the Upper lobe"
- Stone-masons, Sand-blasters
- Whorled collagen (onion-skin pattern)
- Increased TB susceptibility
- Radiograph: fine nodularity upper zones
- Lung cancer risk (modest increase)
Source: Crystalline silica (quartz, cristobalite, tridymite) - sandblasters, hard-rock miners, stone cutters
Pathogenesis: Silica inhaled → macrophage phagocytosis → lysosomal damage → inflammasome activation → IL-1, TNF, lipid mediators, O₂ free radicals, fibrogenic cytokines → progressive fibrosis
Gross
Early: Tiny, barely palpable, pale-to-black nodules in upper zones. Late: Nodules coalesce into hard collagenous scars → PMF → honeycomb pattern. Hilar lymph nodes and pleura also involved with fibrotic lesions ("eggshell calcification" of hilar nodes on X-ray).
Microscopy
Classic silicotic nodule: Concentrically arranged hyalinized collagen fibers surrounding an amorphous center - the "whorled" onion-skin appearance is pathognomonic. Polarized microscopy: weakly birefringent silica particles at the center.
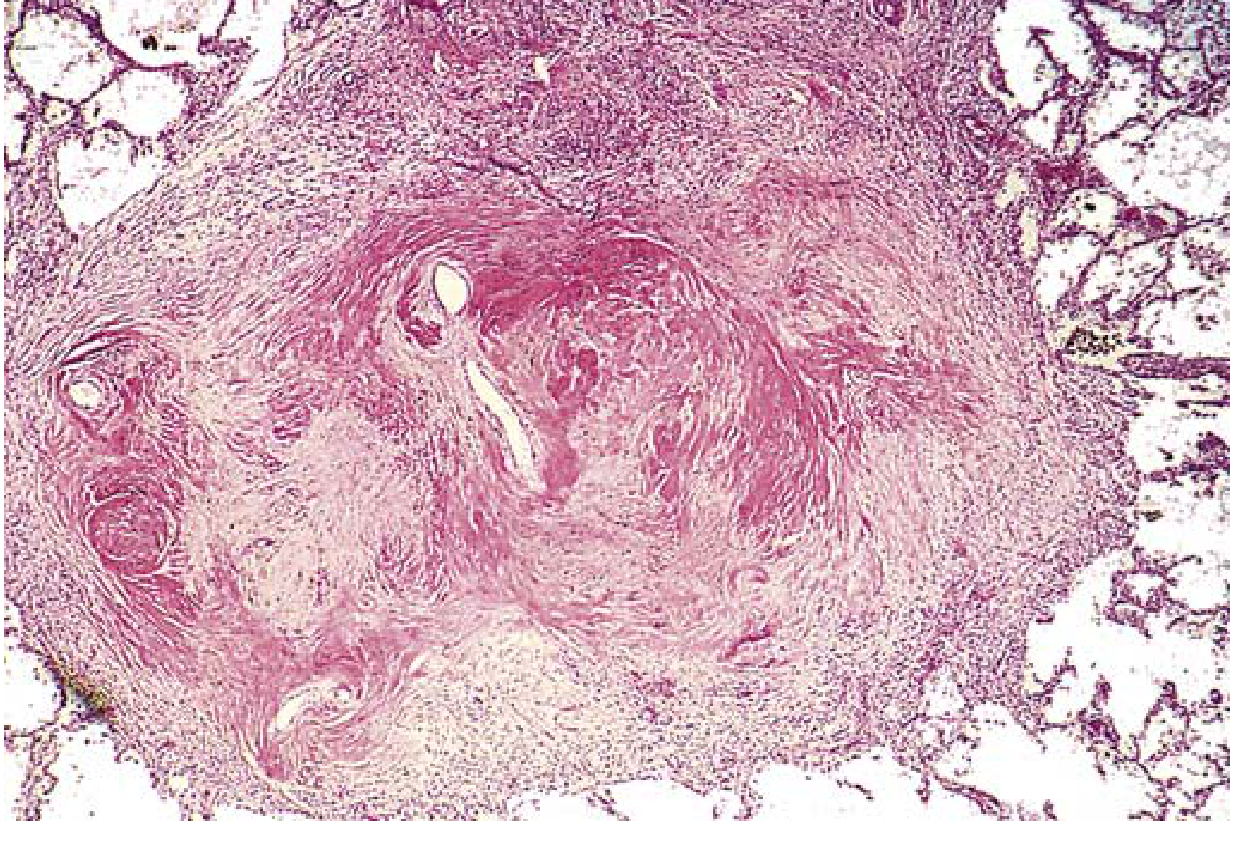
Coalescent collagenous silicotic nodules showing the characteristic whorled/onion-skin pattern. - Robbins Pathology
Clinical
- Often detected incidentally on CXR (fine upper zone nodularity) in asymptomatic workers
- Dyspnea only in advanced PMF
- Silicotuberculosis: Silica inhibits macrophage killing of mycobacteria; nodules show central caseation
- Modestly increased lung cancer risk
4. Asbestosis
Mnemonic: "Asbestos = PLEASE"
Pleural plaques (parietal)
Lower lobe fibrosis (starts there)
Eggshell? No - pleural effusion
Asbestos bodies (golden-brown, beaded)
Smoking synergizes for lung Ca
Extremely high mesothelioma risk (>1000x)
Source: Asbestos fibers (serpentine/amphibole types) - construction, shipbuilding, insulation workers
Pathogenesis: Asbestos fibers phagocytosed → inflammasome activation → phagolysosomal membrane damage → proinflammatory mediators + fibrogenic cytokines → diffuse interstitial fibrosis. Fibers also act as tumor initiators and promoters (free radicals, carcinogen adsorption from tobacco smoke).
Gross
- Asbestosis (parenchymal): Diffuse interstitial fibrosis starting in lower lobes subpleurally, spreading upward. Visceral pleural fibrosis causing lung-chest wall adhesions. Enlarged air spaces creating honeycomb pattern in advanced disease.
- Pleural plaques: Discrete calcified densities on parietal pleura (diaphragm, posterior thorax) - most common asbestos-related finding, usually asymptomatic.
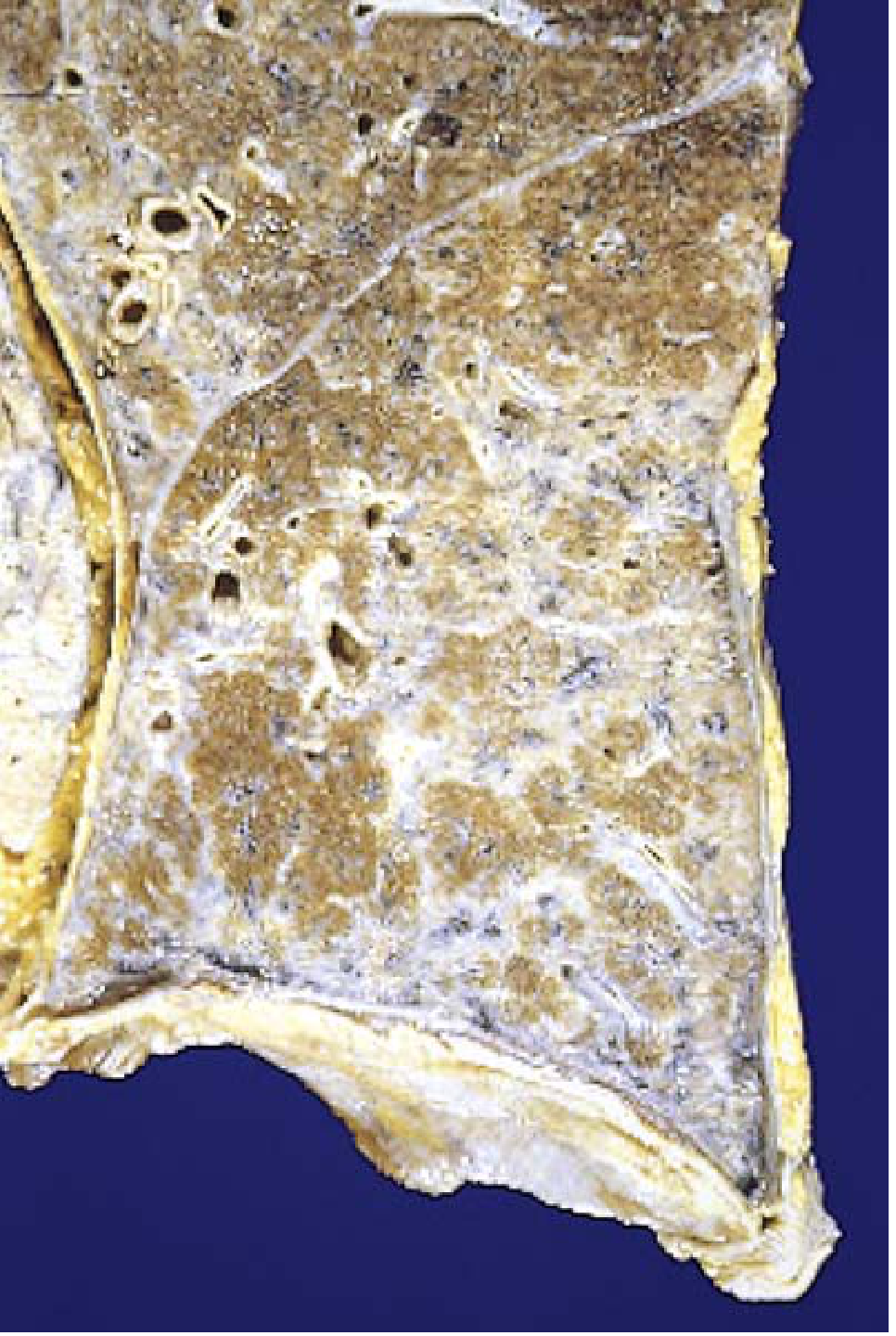
Asbestosis: Markedly thickened visceral pleura covers the lateral and diaphragmatic lung surface. Note severe interstitial fibrosis diffusely affecting the lower lobe. - Robbins Pathology
Microscopy
Asbestos bodies: Golden-brown, fusiform or beaded rods with a translucent fiber center, coated with iron-containing proteinaceous material (ferritin from macrophages). Background shows diffuse interstitial fibrosis.
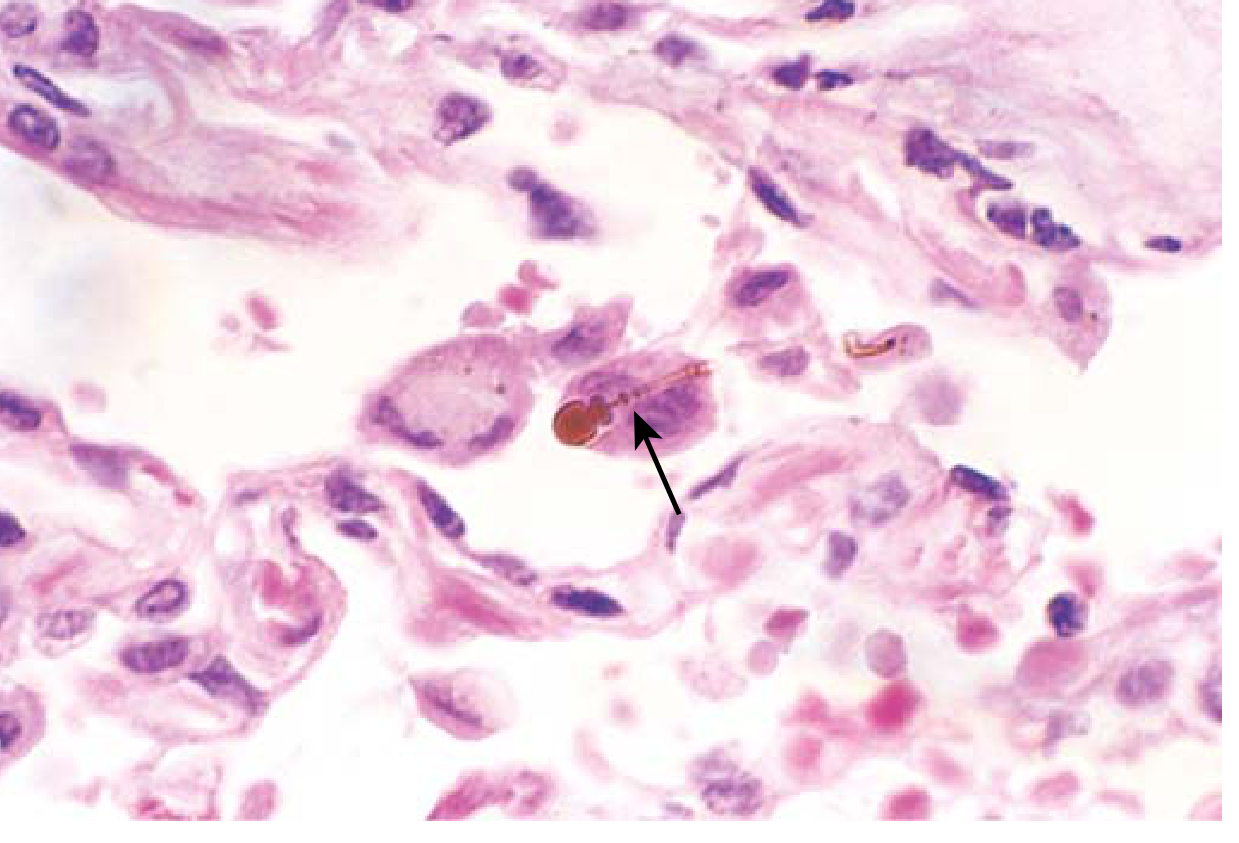
Asbestos body: typical beading and knobbed ends (arrow). - Robbins Pathology
Clinical
- Latency 10-20 years from exposure
- Progressive dyspnea, cough, sputum
- Bibasilar crackles, clubbing
- End-stage: cor pulmonale, congestive heart failure
- Lung carcinoma: 5x increased risk (synergistic with smoking - multiplicative, not additive)
- Mesothelioma: >1000x increased risk; smoking does NOT increase mesothelioma risk (unlike lung Ca)
| Cancer | Asbestos alone | Asbestos + Smoking |
|---|---|---|
| Lung Ca | 5x | ~55x |
| Mesothelioma | >1000x | No added risk |
5. Berylliosis
Mnemonic: "Beryllium = Sarcoidosis-lookalike" - non-caseating granulomas, cannot be distinguished histologically from sarcoidosis
Source: Beryllium/beryllium compounds - aerospace industry, atomic energy plants, beryllium mining, fluorescent light manufacturing
Pathogenesis: Immune-mediated (CD4+ T-cell hypersensitivity) - unlike silicosis/asbestosis which are direct toxic
Gross/Microscopy: Non-caseating epithelioid granulomas indistinguishable from sarcoidosis (beryllium lymphocyte proliferation test needed to differentiate)
Clinical: Clinically identical to pulmonary sarcoidosis. Distinguished by beryllium lymphocyte proliferation test (BeLPT) and occupational history.
6. Byssinosis (Cotton Dust / "Brown Lung")
Source: Cotton, flax, hemp dust - textile mills
Mnemonic: "Monday Morning Tightness" - symptoms worst on return after weekend off, improve as week progresses ("Monday morning disease")
Pathogenesis: Endotoxins and tannins in cotton bracts → release of histamine, leukotrienes → bronchoconstriction
Microscopy/Gross: No characteristic structural change (unlike other pneumoconioses). Chronic cases may show peribronchial fibrosis.
Clinical: Reversible bronchoconstriction initially → chronic obstructive disease with prolonged exposure.
Comparison Table
| Feature | Anthracosis | CWP | Silicosis | Asbestosis | Berylliosis |
|---|---|---|---|---|---|
| Source | Carbon/smoke | Coal dust | Quartz/silica | Asbestos fibers | Beryllium |
| Location | Lymphatics | Upper lobes | Upper lobes | Lower lobes (start) | Diffuse |
| Key lesion | Pigment deposits | Coal macules/PMF | Whorled nodules | Asbestos bodies | Non-caseating granulomas |
| Pattern | No fibrosis | Progressive fibrosis | Progressive fibrosis | Interstitial fibrosis | Granulomatous |
| Cancer risk | None | None (lung Ca) | Modest lung Ca | Lung Ca + Mesothelioma | None established |
| Special associations | Ubiquitous | Caplan syndrome | Silicotuberculosis | Pleural plaques, effusion | Mimics sarcoidosis |
Overall Key Mnemonic: "Silica Attacks UPPER, Asbestos Attacks LOWER"
- Silicosis - upper zone nodules, whorled collagen, birefringent crystals by polarized light
- Asbestosis - lower lobe subpleural fibrosis, asbestos bodies, golden-brown beaded rods
Sources: Robbins & Kumar Basic Pathology, The Washington Manual of Medical Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.