Femoral artery saq
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
Reading File
I now have all the material needed for a thorough SAQ answer. Let me compile the complete response.
Femoral Artery - Short Answer Question (SAQ)
Origin
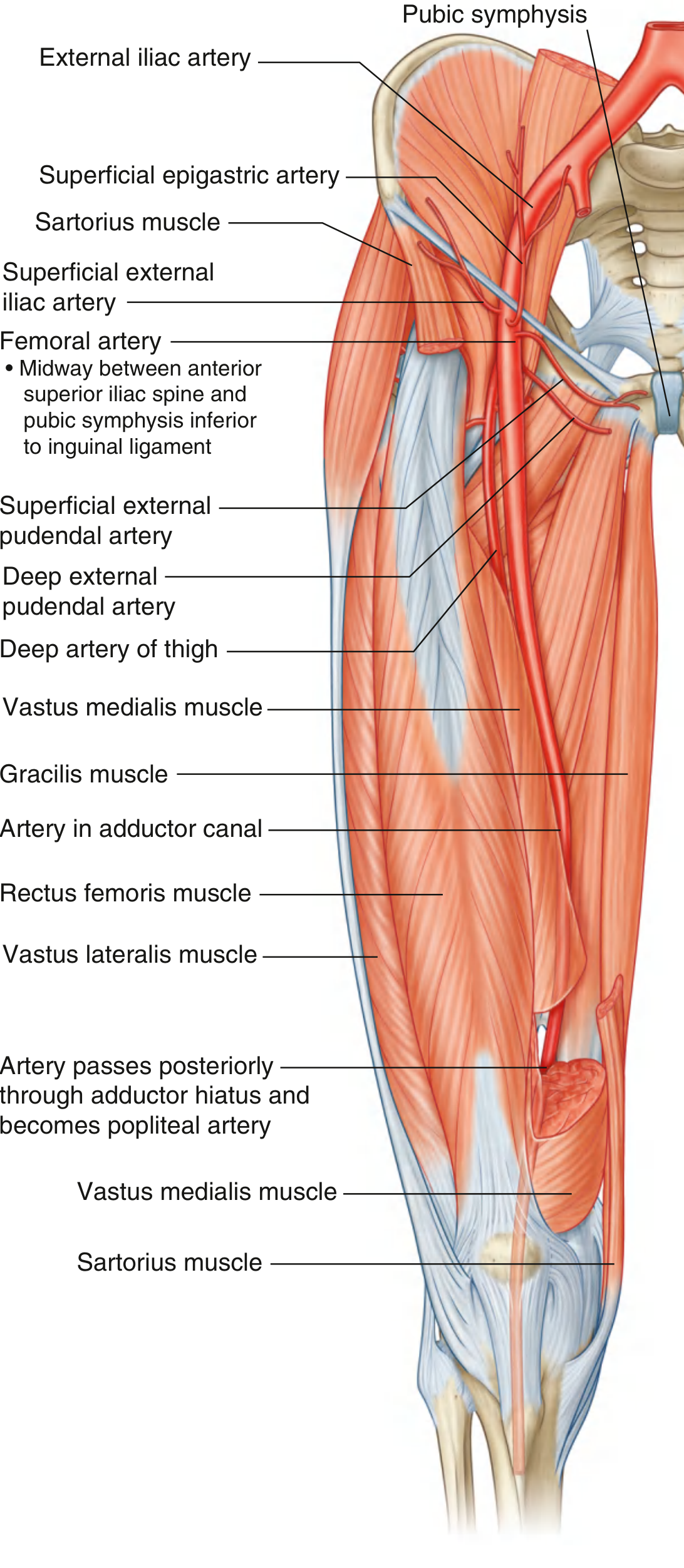
The femoral artery is the direct continuation of the external iliac artery. It begins where the external iliac artery passes deep to the inguinal ligament at the mid-inguinal point (midway between the anterior superior iliac spine and the pubic symphysis).
Course
The femoral artery has three distinct segments:
1. In the Femoral Triangle
- Enters the femoral triangle by passing deep to the inguinal ligament
- Lies within the femoral sheath (lateral compartment), with the femoral vein immediately medial and the femoral nerve lateral (but outside the sheath)
- Reliably bisects the inguinal ligament at its midpoint - useful landmark when no palpable pulse exists
- Pulse is palpable here just inferior to the inguinal ligament
2. In the Adductor Canal (Hunter's Canal)
- Leaves the femoral triangle and enters the adductor canal
- The femoral vein shifts from medial to posterior to the artery as it travels distally
- Accompanied by the saphenous nerve, which crosses the artery within the canal
- The canal is bounded by: vastus medialis (laterally), adductor longus and adductor magnus (medially/posteriorly), sartorius (anteriorly as its roof)
3. Exits via Adductor Hiatus
- Passes through the adductor hiatus in the adductor magnus muscle
- Becomes the popliteal artery in the popliteal fossa behind the knee
Relations in the Femoral Triangle
Mnemonic: NAVY (lateral to medial)
- N - Femoral Nerve (outside sheath, most lateral)
- A - Femoral Artery (lateral compartment of sheath)
- V - Femoral Vein (medial compartment of sheath)
- Y - Lymphatics/femoral canal (most medial compartment of sheath)
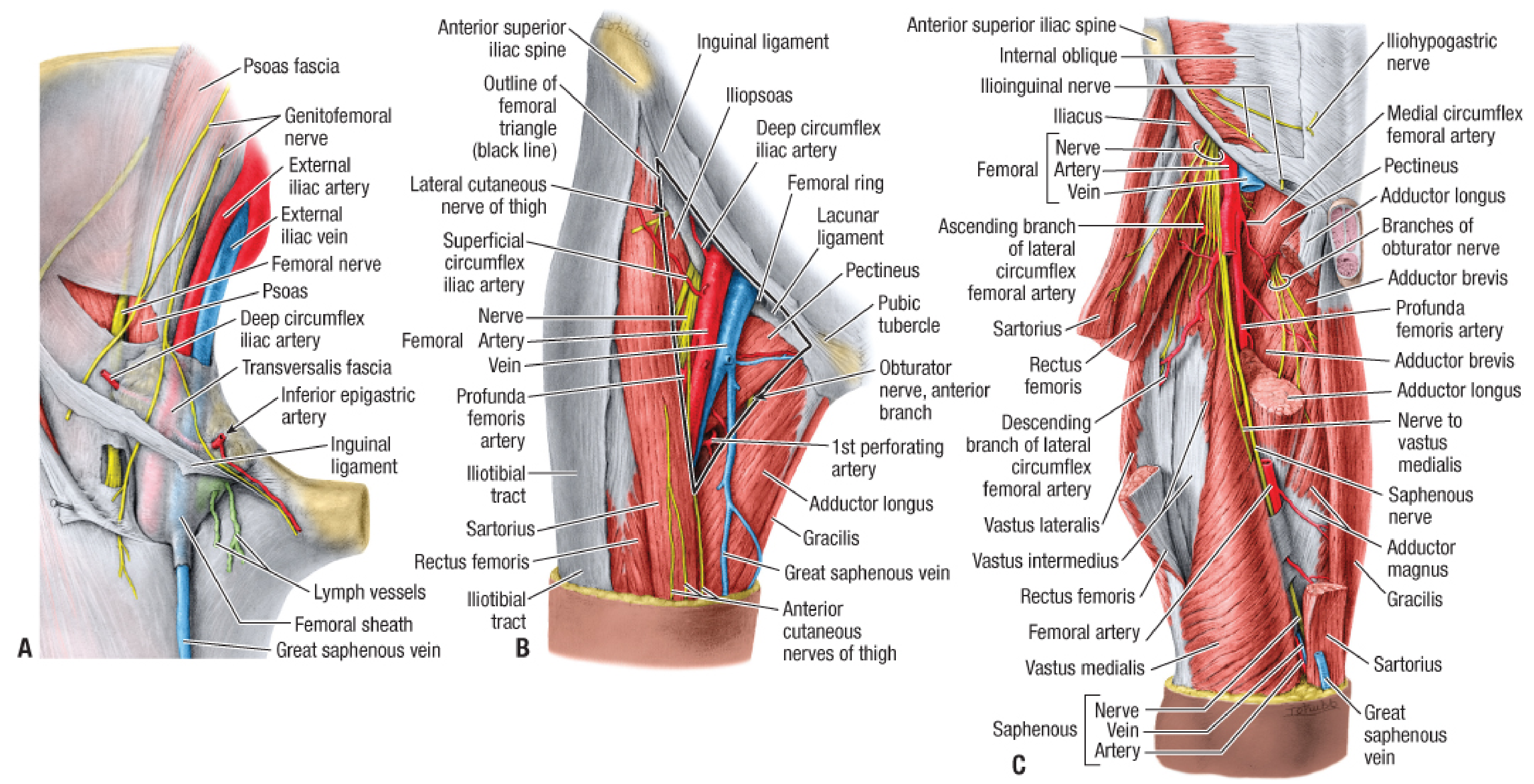
Femoral Triangle (Boundaries)
| Feature | Structure |
|---|---|
| Superior (base) | Inguinal ligament |
| Lateral border | Sartorius |
| Medial border | Adductor longus (medial border) |
| Floor | Iliopsoas, pectineus, adductor longus |
| Roof | Fascia lata + cribriform fascia |
Femoral Sheath
A funnel-shaped fascial sleeve, continuous superiorly with:
- Transversalis fascia (anteriorly)
- Iliac fascia (posteriorly)
Contains 3 compartments (lateral to medial):
- Lateral - Femoral artery
- Middle - Femoral vein
- Medial - Femoral canal (contains lymphatics; the femoral ring is its upper opening - site of femoral hernias)
The femoral nerve is NOT inside the femoral sheath.
Branches
Small branches in the femoral triangle:
- Superficial epigastric artery - runs to the anterior abdominal wall
- Superficial circumflex iliac artery - runs laterally toward ASIS
- Superficial external pudendal artery - supplies scrotum/labia majora
- Deep external pudendal artery - supplies perineum
Major branch:
- Profunda femoris artery (Deep artery of thigh) - arises from the posterolateral aspect of the femoral artery, approximately 4-5 cm below the inguinal ligament; this is the main blood supply to the thigh muscles
Branches of profunda femoris:
- Medial circumflex femoral artery - provides the principal blood supply to the head and neck of the femur (passes between pectineus/iliopsoas, then obturator externus/adductor brevis)
- Lateral circumflex femoral artery - gives ascending, descending, and transverse branches; participates in the cruciate anastomosis around the hip
- Three perforating arteries - penetrate adductor magnus to supply the posterior compartment of the thigh and form longitudinal anastomotic chains
Cruciate Anastomosis
Formed around the hip by:
- Medial circumflex femoral artery
- Lateral circumflex femoral artery (transverse branch)
- Inferior gluteal artery
- First perforating artery of profunda femoris
This provides collateral circulation if the femoral or iliac artery is obstructed.
Termination
At the adductor hiatus in adductor magnus → becomes the popliteal artery.
Before passing through the hiatus, the femoral artery gives off the descending genicular artery, which joins the genicular anastomosis around the knee.
Clinical Relevance
| Application | Details |
|---|---|
| Pulse palpation | Felt at mid-inguinal point, below inguinal ligament |
| Vascular access / catheterization | Coronary angiography, cardiac catheterization, peripheral angiography |
| Femoral hernia | Protrudes through the femoral ring (medial compartment of femoral sheath), more common in females |
| Femoral artery aneurysm | Most commonly involves the common femoral artery (>80%); may involve profunda femoris |
| Superficial femoral artery occlusion | Common site of atherosclerosis causing intermittent claudication |
| Nerve injury risk | Saphenous nerve and nerve to vastus medialis lie lateral to the artery in the femoral sheath - at risk if excessive lateral dissection is performed |
| Groin access point | The inguinal skin crease is 3-4 cm distal to the true inguinal ligament - important when locating the vessel surgically |
Sources: Gray's Anatomy for Students (pp. 669-704); Fischer's Mastery of Surgery, 8th ed. (Chapter 238); Imaging Anatomy, Vol. 3 (pp. 359-365)
Thorax all mbbs topic explain
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
Loading Image
Reading File
Reading File
Reading File
Reading File
THORAX - Complete MBBS Anatomy Notes
Source: Gray's Anatomy for Students, Fischer's Mastery of Surgery, Imaging Anatomy Vol. 3
PART 1: THORACIC WALL & SKELETON
Thoracic Cage Components
- Sternum (anteriorly): Manubrium + Body + Xiphoid process
- 12 pairs of ribs (laterally and posteriorly)
- 12 thoracic vertebrae (posteriorly)
Sternum Landmarks
| Part | Level | Clinical Importance |
|---|---|---|
| Manubrium | T3-T4 | Manubriosternal joint = Sternal angle (angle of Louis) |
| Sternal angle | TIV-TV disc level | Most important landmark in thorax |
| Body | T5-T9 | Xiphisternal joint at T9 |
| Xiphoid process | Variable | Lower sternal boundary |
The Sternal Angle (Angle of Louis) - HIGH YIELD
At the level of TIV-TV disc:
- Junction of manubrium and body of sternum
- Level of 2nd costal cartilage (rib counting starts here)
- Bifurcation of trachea (carina)
- Arch of aorta begins and ends here
- Divides mediastinum into superior and inferior
Classification of Ribs
| Type | Ribs | Details |
|---|---|---|
| True (vertebrosternal) | 1-7 | Attach directly to sternum via own costal cartilage |
| False (vertebrochondral) | 8-10 | Costal cartilage joins rib above, not sternum directly |
| Floating (vertebral) | 11-12 | No anterior attachment; end free in abdominal wall muscles |
Intercostal Space - Contents (VAN)
Order from superior to inferior, sheltered in costal groove:
- V - Vein (most superior)
- A - Artery
- N - Nerve (most inferior - most exposed)
The posterior intercostal arteries (1st and 2nd from superior intercostal artery; 3rd-11th from thoracic aorta) supply the posterior chest wall.
The anterior intercostal arteries arise from the internal thoracic artery (a branch of subclavian artery).
Clinical point: When inserting a chest drain/needle, always go over the upper border of the rib below to avoid the neurovascular bundle sheltered under the upper rib.
Thoracic Apertures
| Aperture | Structures passing through |
|---|---|
| Superior thoracic aperture (inlet) | Trachea, esophagus, vessels (brachiocephalic, subclavian, carotid), phrenic and vagus nerves, thoracic duct, sympathetic trunks |
| Inferior thoracic aperture (outlet) | Closed by the diaphragm |
PART 2: PLEURAL CAVITIES & PLEURA
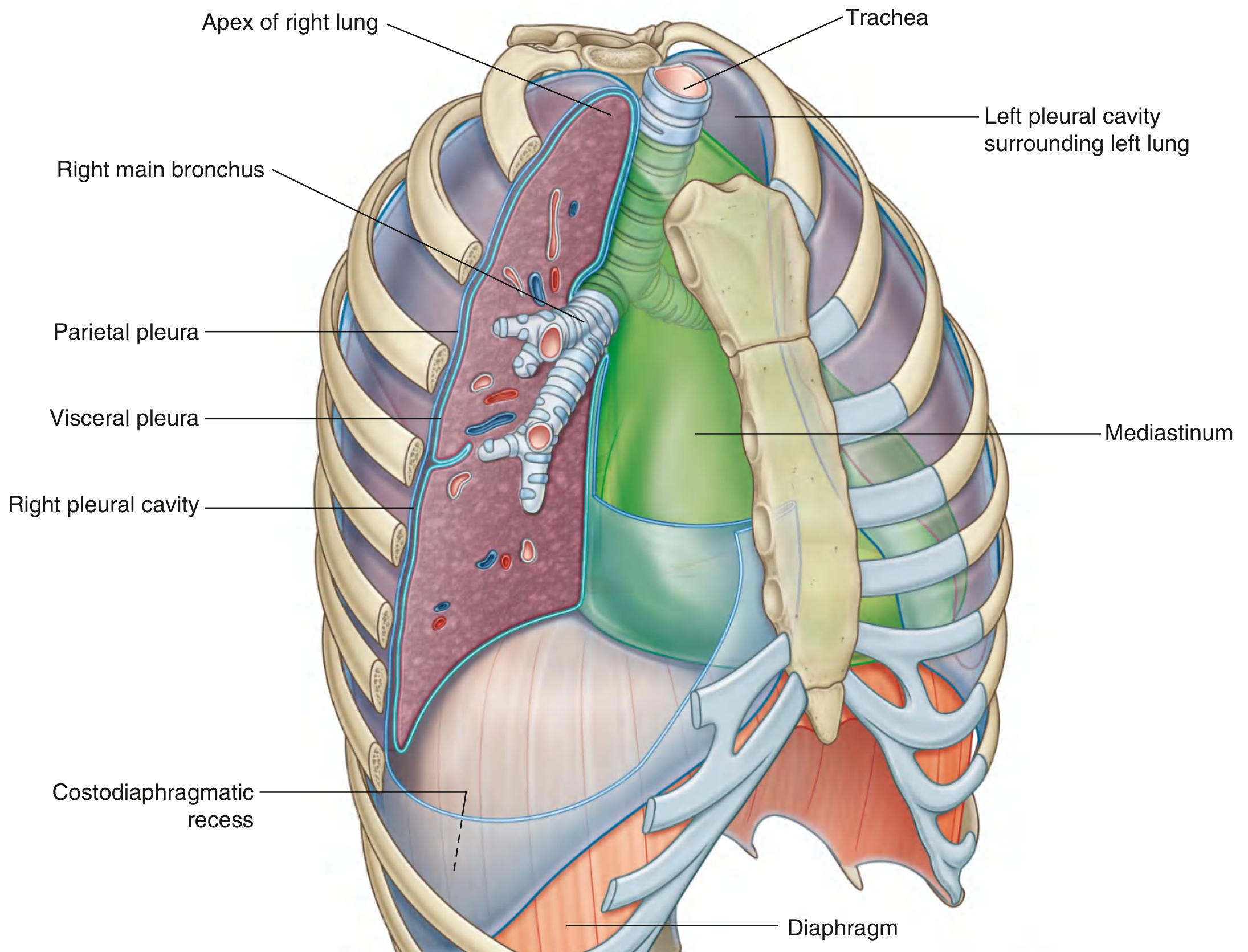
Pleura Types
- Parietal pleura - lines the walls of the thoracic cavity (has 4 named parts):
- Costal pleura (lines ribs)
- Diaphragmatic pleura
- Mediastinal pleura
- Cervical pleura (cupola) - extends 2-3 cm above rib I into neck
- Visceral pleura - adheres to lung surface
- Both are continuous at the lung root
Pleural Recesses
- Costodiaphragmatic recess (most important) - between chest wall and diaphragm; site where fluid collects first
- Costomediastinal recess - between costal and mediastinal pleura, anterior
Nerve Supply of Pleura
- Parietal pleura - somatic innervation (intercostal nerves and phrenic nerves) = can feel PAIN
- Visceral pleura - autonomic = INSENSITIVE to pain (visceral afferents only)
Clinical: Pleural Effusion
Fluid collects first in the costodiaphragmatic recess. Dullness on percussion from below upward. Diagnosed on CXR and ultrasound.
Clinical: Pneumothorax
Air enters pleural space → lung collapses. Tension pneumothorax is a medical emergency with mediastinal shift away.
PART 3: MEDIASTINUM
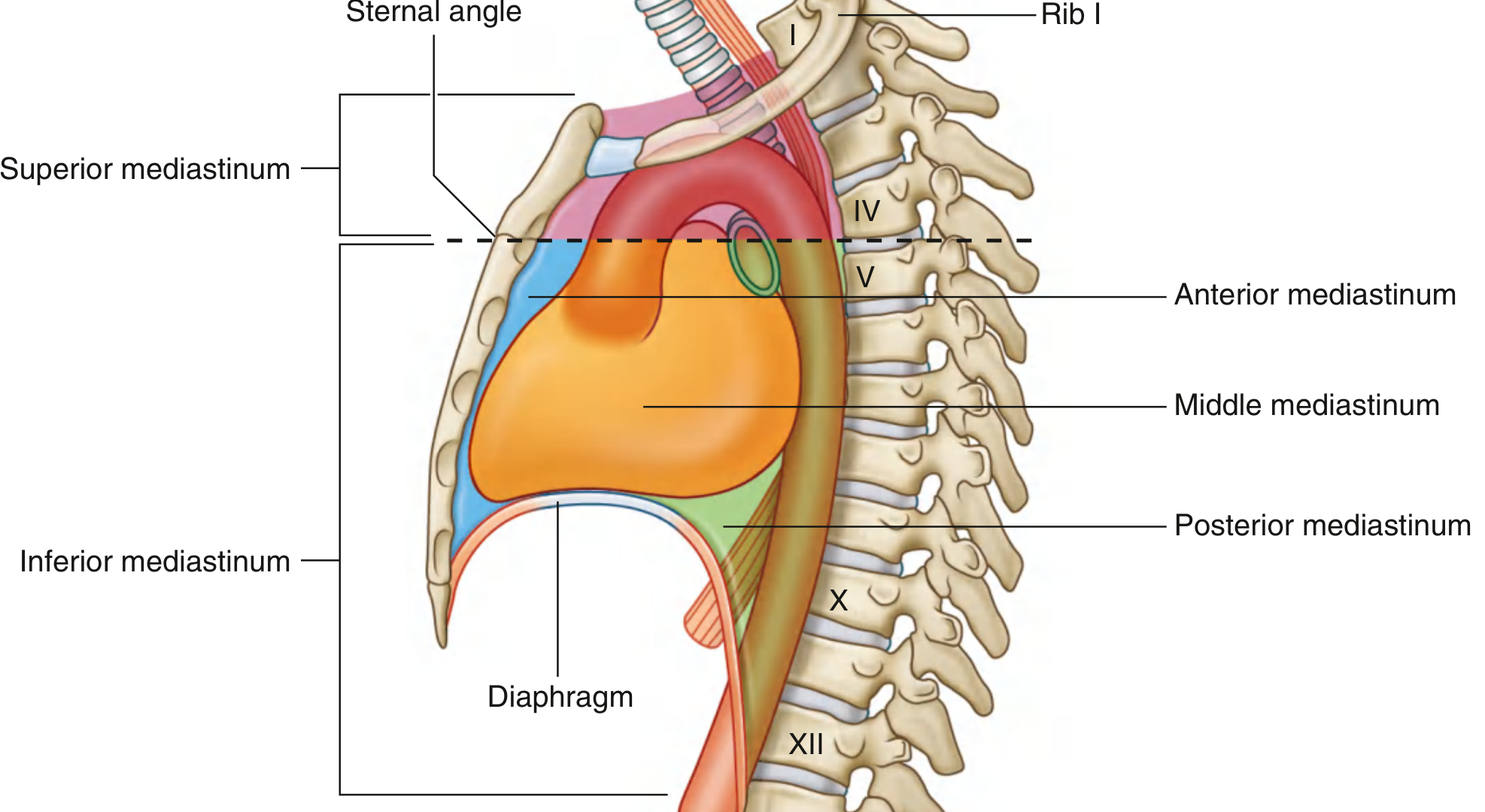
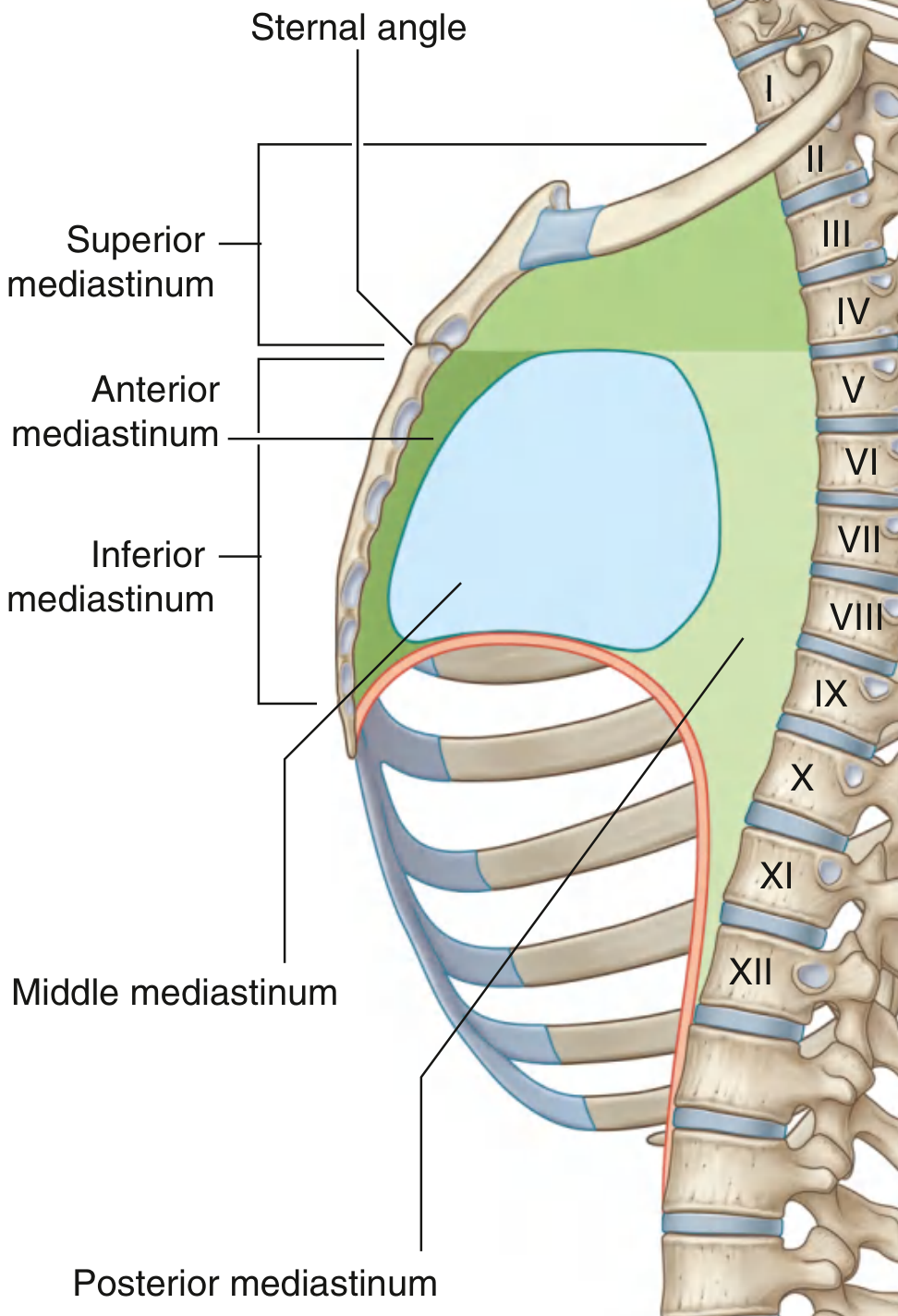
Division of Mediastinum
Dividing plane: Horizontal plane through the sternal angle (TIV-TV disc)
| Division | Location |
|---|---|
| Superior mediastinum | Above sternal angle plane |
| Inferior mediastinum | Below sternal angle plane, further divided by pericardium into: anterior, middle, posterior |
Superior Mediastinum - Contents
- Thymus gland (or its remnant/fat)
- Brachiocephalic veins (left and right) → form Superior Vena Cava
- Arch of aorta and its 3 branches:
- Brachiocephalic trunk (→ right subclavian + right common carotid)
- Left common carotid artery
- Left subclavian artery
- Trachea (bifurcates at carina at sternal angle level)
- Oesophagus (posterior to trachea)
- Thoracic duct (upper part)
- Phrenic nerves (bilateral)
- Vagus nerves (bilateral)
- Left recurrent laryngeal nerve (hooks under arch of aorta at ligamentum arteriosum)
- Sympathetic trunks (bilateral)
- Lymph nodes
Key clinical: Left recurrent laryngeal nerve passes through the aortopulmonary window. Lung cancer / enlarged lymph nodes here compress it → hoarseness of voice.
Anterior Mediastinum - Contents
- Inferior extension of thymus
- Fat and connective tissue
- Mediastinal branches of internal thoracic vessels
- Sternopericardial ligaments
- Lymph nodes
Masses here: Thymic tumours, Teratoma, Thymoma, Lymphoma ("4 T's of anterior mediastinum")
Middle Mediastinum - Contents
- Pericardium
- Heart (the main occupant)
- Ascending aorta and pulmonary trunk (proximal)
- Superior and inferior vena cava (proximal)
- Pulmonary veins (proximal)
- Phrenic nerves (along pericardium)
- Pericardiacophrenic vessels
Posterior Mediastinum - Contents
- Oesophagus (with oesophageal plexus of vagus)
- Descending thoracic aorta
- Azygos vein (right side) and hemiazygos / accessory hemiazygos veins (left side)
- Thoracic duct
- Thoracic sympathetic trunks
- Splanchnic nerves
- Posterior intercostal vessels
- Lymph nodes
PART 4: LUNGS
General Features
- Right lung: 3 lobes (upper, middle, lower), 2 fissures (oblique + horizontal), 10 bronchopulmonary segments, shorter and wider
- Left lung: 2 lobes (upper, lower), 1 fissure (oblique), 9-10 bronchopulmonary segments; has lingula (homologue of right middle lobe), cardiac notch on anterior border
Lung Root (Hilum) Contents - Order
At the hilum of both lungs: bronchus, pulmonary artery, pulmonary veins (2 each), bronchial vessels, lymphatics, nerves
Right hilum (superior to inferior): Pulmonary artery, bronchus, pulmonary veins
Left hilum: Pulmonary artery is highest, then bronchus
Bronchi
- Trachea bifurcates at carina (T4-T5 level, sternal angle)
- Right main bronchus: Shorter, wider, more vertical (foreign bodies enter right side more often)
- Left main bronchus: Longer, narrower, more horizontal
Bronchopulmonary Segments
Each segment is:
- A distinct structural and functional unit
- Supplied by its own segmental (tertiary) bronchus
- Has its own segmental artery (branch of pulmonary artery)
- Can be surgically resected independently
Blood Supply of Lungs
- Pulmonary arteries (deoxygenated blood for gas exchange)
- Bronchial arteries (oxygenated blood for lung tissue nutrition) - from thoracic aorta (left) and right intercostal/subclavian (right)
Nerve Supply
- Pulmonary plexus (anterior and posterior) - sympathetic + parasympathetic (vagus)
- Sympathetic = bronchodilation + vasoconstriction
- Parasympathetic = bronchoconstriction + secretion
Surface Markings of Lungs and Pleura
| Feature | Level |
|---|---|
| Lung apex (both) | 2.5 cm above medial clavicle |
| Anterior border diverges on left | At 4th costal cartilage (cardiac notch) |
| Lower border of lung | Rib 6 (MCL), Rib 8 (MAL), Rib 10 (posteriorly) |
| Lower border of pleura | Rib 8 (MCL), Rib 10 (MAL), Rib 12 (posteriorly) |
| Difference lung-pleura | 2 ribs (the pleura extends 2 ribs lower = costodiaphragmatic recess) |
PART 5: PERICARDIUM & HEART
Pericardium
Two layers:
- Fibrous pericardium (outer) - tough; apex is continuous with adventitia of great vessels; base is attached to central tendon of diaphragm; attached to sternum by sternopericardial ligaments
- Serous pericardium (inner) - two layers:
- Parietal serous pericardium (lines fibrous pericardium)
- Visceral serous pericardium = Epicardium (covers the heart)
Between parietal and visceral serous layers = Pericardial cavity (contains small amount of fluid)
Pericardial Sinuses
- Transverse pericardial sinus - between arteries (aorta + pulmonary trunk) anteriorly and veins (SVC + pulmonary veins) posteriorly. A finger placed here during surgery separates arteries from veins.
- Oblique pericardial sinus - J-shaped recess posterior to left atrium (between pulmonary veins)
Nerve Supply of Pericardium
- Phrenic nerves (C3, C4, C5) carry somatic sensation (pain) from parietal pericardium
- Pain referred to shoulder and lateral neck (C3-C5 dermatomes)
- Also receives vagus nerve and sympathetic trunk fibers (visceral)
Clinical: Pericarditis
- Inflammation of pericardium - diffuse ST elevation on ECG
- Pain relieved by sitting forward (unlike MI)
- Causes: viral, bacterial, post-MI, uraemia, autoimmune
Clinical: Cardiac Tamponade
- Fluid in pericardial sac compresses heart
- Beck's triad: hypotension + raised JVP + muffled heart sounds
- Treatment: pericardiocentesis (needle inserted below xiphoid process at a 45° angle toward left shoulder)
PART 6: THE HEART
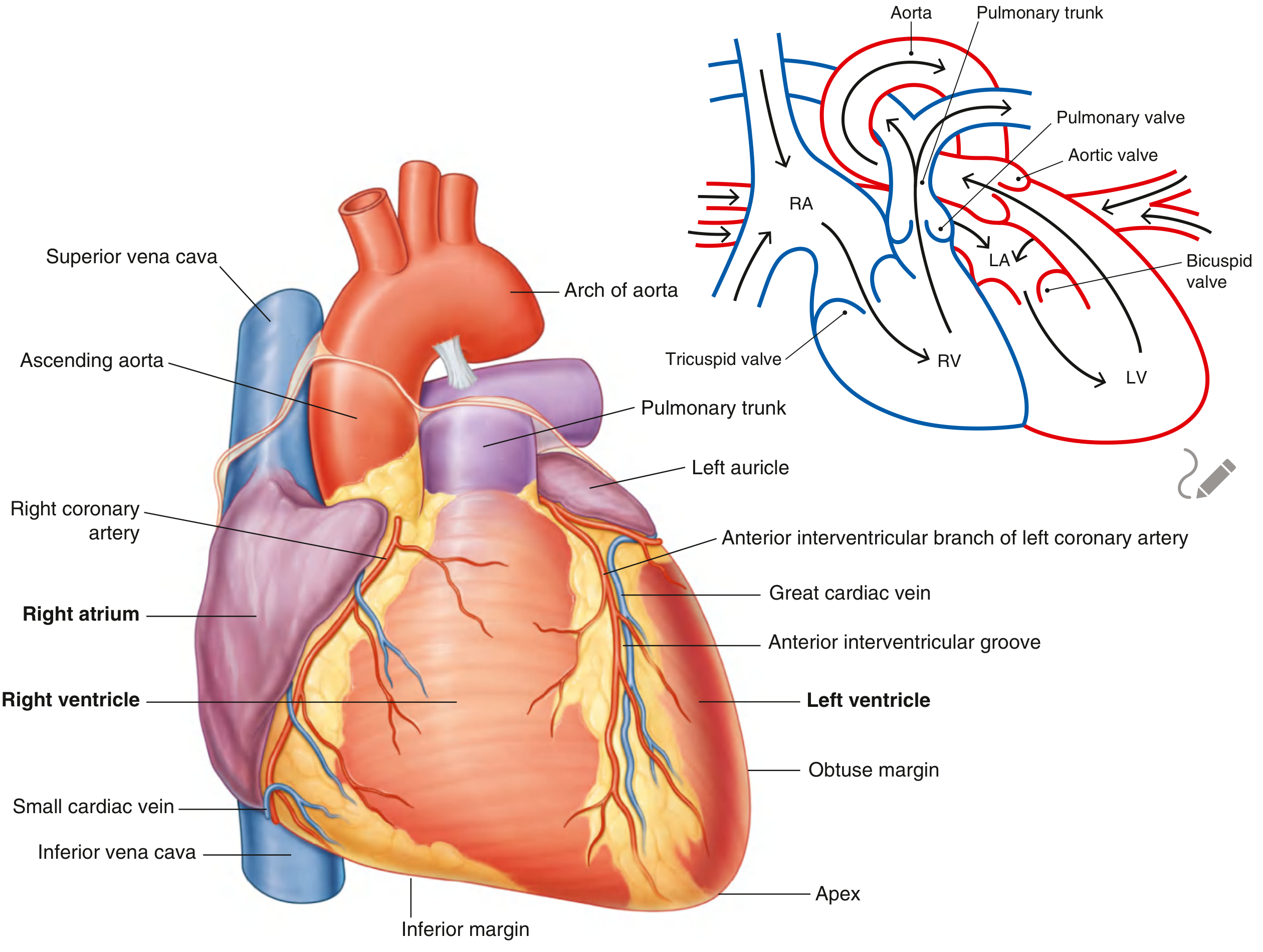
Position and Orientation
- Located in the middle mediastinum
- Base faces posteriorly (at T5-T8 level)
- Apex points inferolaterally to the left
- Apex beat: Left 5th intercostal space, 8-9 cm from midsternal line (mid-clavicular line)
Surfaces of the Heart
| Surface | Formed by |
|---|---|
| Anterior (sternocostal) | Mainly right ventricle, some right atrium and left ventricle |
| Inferior (diaphragmatic) | Left ventricle (mainly) + small part of right ventricle |
| Left pulmonary surface | Left ventricle |
| Right surface | Right atrium |
| Base (posterior) | Left atrium (mainly) + right atrium |
Chambers - Key Points
Right Atrium:
- Receives: Superior vena cava (above) + Inferior vena cava (below) + Coronary sinus
- Internal features: Crista terminalis (divides into sinus venarum and atrium proper), Musculi pectinati, Fossa ovalis (remnant of foramen ovale)
- The crista terminalis marks the SA node location superiorly
Right Ventricle:
- Forms most of anterior surface
- Inflow (rough, trabeculated) + Conus arteriosus/Infundibulum (smooth outflow to pulmonary trunk)
- Valve: Tricuspid valve (3 cusps: anterior, posterior, septal)
- Contains: trabeculae carneae, papillary muscles (3: anterior, posterior, septal), moderator band (septomarginal trabecula) carrying right bundle branch
Left Atrium:
- Receives 4 pulmonary veins (2 from each lung)
- Predominantly smooth walled; small auricle has pectinate muscles
- Most posterior chamber - esophagus lies directly behind
Left Ventricle:
- Thick-walled (wall thickness ~3x right ventricle)
- Inflow (rough) + Aortic vestibule (smooth outflow)
- Valve: Mitral (bicuspid) valve (2 cusps: anterior and posterior); guarded by 2 papillary muscles
Cardiac Valves - Surface Markings & Auscultation Sites
| Valve | Anatomical location | Auscultation site |
|---|---|---|
| Pulmonary | Left 3rd costal cartilage, sternal border | Left 2nd ICS, sternal border |
| Aortic | Right 3rd costal cartilage, sternal border | Right 2nd ICS, sternal border |
| Mitral | Left 4th costal cartilage, sternal border | Apex (5th ICS, MCL) |
| Tricuspid | Right 4th-5th ICS, sternal border | Left 4th-5th ICS, sternal border |
Coronary Arteries
Two main arteries arise from the aortic sinuses (just above aortic valve):
Right Coronary Artery (RCA) - from right aortic sinus:
- Travels in right atrioventricular groove
- Branches: SA nodal artery (60%), right marginal artery, AV nodal artery (most cases)
- Terminates as posterior interventricular artery (PDA) in right-dominant hearts (70%)
- Supplies: Right atrium, right ventricle, SA node, AV node (usually), posterior LV
Left Coronary Artery (LCA) - from left aortic sinus:
- Short left main stem → divides into:
- Anterior interventricular artery (LAD) - descends in anterior interventricular groove; supplies most of interventricular septum, anterior LV, anterior RV
- Circumflex artery (LCx) - travels in left AV groove; supplies left atrium, lateral/posterior LV; gives left marginal artery
Dominance: The artery that supplies the posterior descending artery (PDA)
- Right dominant: 70%
- Left dominant: 10%
- Co-dominant: 20%
Cardiac Veins
- Great cardiac vein - runs with LAD, drains into coronary sinus
- Middle cardiac vein - runs with PDA
- Small cardiac vein - runs with right marginal artery
- All drain into Coronary sinus → empties into right atrium
- Some small anterior cardiac veins drain directly into right atrium
Cardiac Conduction System
SA node (Sinu-atrial node):
- "Pacemaker of the heart" - intrinsic rate 60-100 bpm
- Located at the superior end of crista terminalis (junction of SVC and right atrium)
- Blood supply: Right coronary artery (60%), LCx (40%)
AV node (Atrioventricular node):
- Located in the interatrial septum near the opening of the coronary sinus (Triangle of Koch)
- Intrinsic rate 40-60 bpm
- Blood supply: Right coronary artery (usually)
Bundle of His: Passes through fibrous skeleton from AV node → divides into right and left bundle branches
Left bundle branch: Divides into anterior and posterior fascicles
Purkinje fibres: Subendocardial plexus - terminal fibres causing ventricular contraction from apex upward
PART 7: GREAT VESSELS
Arch of Aorta
- Begins and ends at sternal angle (T4-T5 level)
- Arches over the left main bronchus
- 3 branches (right to left):
- Brachiocephalic trunk (→ right subclavian + right common carotid arteries)
- Left common carotid artery
- Left subclavian artery
- Ligamentum arteriosum (remnant of ductus arteriosus) connects arch to left pulmonary artery
Clinical: Coarctation of Aorta
- Narrowing usually just distal to origin of left subclavian artery (juxtaductal)
- Collateral circulation via intercostal arteries → rib notching on X-ray (lower borders of 3rd-9th ribs)
- Higher BP in arms vs legs; radio-femoral delay
Pulmonary Trunk
- Arises from right ventricle, passes upward and left
- Divides at T5-T6 (under arch of aorta) into right and left pulmonary arteries
- Right PA: passes posterior to ascending aorta and SVC → right lung
- Left PA: passes anteriorly to descending aorta → left lung
Superior Vena Cava (SVC)
- Formed by union of left + right brachiocephalic veins
- Drains: Upper half of body
- SVC syndrome: Obstruction causes facial and upper limb edema, dilated chest wall veins
Azygos Vein System
- Azygos vein (right side): drains posterior thoracic wall, enters SVC at T4 level
- Hemiazygos vein (left side, lower): crosses midline at T9 to join azygos
- Accessory hemiazygos (left side, upper): crosses midline at T8 to join azygos
- The azygos system is a major collateral pathway when IVC or SVC is obstructed
PART 8: DIAPHRAGM
Structure
- Musculotendinous dome separating thorax from abdomen
- Peripheral muscle + Central tendon
- Two domes: Right dome higher (T8-T9) due to liver; Left dome lower (T9-T10)
Attachments (origins of muscular parts)
- Sternal part: posterior surface of xiphoid process
- Costal part: inner surfaces of lower 6 ribs and costal cartilages
- Vertebral part: by crura (right crus from L1-L3, left crus from L1-L2) and arcuate ligaments
Openings and Levels - HIGH YIELD EXAM TOPIC
| Opening | Level | Structures passing through |
|---|---|---|
| Caval foramen (Vena caval hiatus) | T8 (in central tendon) | IVC + right phrenic nerve |
| Oesophageal hiatus | T10 (in muscular part - right crus) | Oesophagus + vagus nerves (anterior and posterior trunks) + oesophageal branches of left gastric vessels |
| Aortic hiatus | T12 (technically behind diaphragm - between crura) | Aorta + thoracic duct + azygos vein |
Mnemonic: I (IVC) 8 (T8) 10 (T10) Eggs (oesophagus) At (Aorta) 12 (T12)
Nerve Supply
- Motor: Phrenic nerve only (C3, C4, C5 - "C3, 4, 5 keeps the diaphragm alive")
- Sensory:
- Central (tendinous) portion - phrenic nerve (referred pain to shoulder, C3-C5)
- Peripheral portion - lower 6 intercostal nerves
Blood Supply
- Superior surface: Pericardiacophrenic, musculophrenic, superior phrenic arteries
- Inferior surface: Inferior phrenic arteries (from abdominal aorta or coeliac)
Diaphragmatic Hernias
- Hiatus hernia - stomach herniation through esophageal hiatus (most common)
- Sliding (type I) - 90%: gastroesophageal junction moves up
- Rolling/Para-oesophageal (type II): gastric fundus herniates alongside normal GEJ
- Bochdalek hernia (congenital, posterolateral) - left side more common
- Morgagni hernia (congenital, anterior) - right side more common
PART 9: KEY NERVES IN THORAX
Phrenic Nerve (C3, C4, C5)
- Right phrenic: Down right of SVC → along right side of pericardium → exits through caval foramen (T8) with IVC
- Left phrenic: Crosses over aortic arch superficial to left vagus → along left side of pericardium → pierces diaphragm near apex
Vagus Nerve (CN X) in Thorax
- Right vagus: Crosses anterior to right subclavian artery → gives right recurrent laryngeal nerve (hooks under right subclavian) → passes posteriorly → joins oesophageal plexus → exits as posterior vagal trunk through oesophageal hiatus (T10)
- Left vagus: Crosses aortic arch → gives left recurrent laryngeal nerve (hooks under arch of aorta at ligamentum arteriosum) → passes posteriorly → joins oesophageal plexus → exits as anterior vagal trunk
Clinical: Left RLN: hoarseness in lung cancer, aortic aneurysm. Right RLN: hoarseness in right apex lung cancer.
Thoracic Duct
- Largest lymphatic vessel
- Enters thorax through aortic hiatus (T12)
- Ascends in posterior mediastinum between oesophagus and azygos vein
- Crosses midline at T5, ascends in superior mediastinum
- Drains into left venous angle (junction of left internal jugular + left subclavian veins)
- Drains ALL lymph EXCEPT: right side of head/neck/thorax + right upper limb (drained by right lymphatic duct)
PART 10: CLINICAL ANATOMY SUMMARY TABLE
| Topic | Key Point |
|---|---|
| Sternal angle | T4-T5 disc; 2nd rib; tracheal bifurcation; arch of aorta |
| Chest drain | Above upper border of rib below (to avoid VAN bundle) |
| Safe triangle for drain | Anterior to latissimus dorsi, lateral to pectoral border, above 5th rib, apex near axilla |
| Foreign body aspiration | Goes to right main bronchus (shorter, wider, vertical) |
| Pericardiocentesis | Below xiphoid, 45° angle toward left shoulder |
| Cardiac apex | Left 5th ICS, mid-clavicular line |
| Left RLN hoarseness | Aortopulmonary window compression by lung cancer/nodes |
| Rib notching on X-ray | Coarctation of aorta (collateral intercostal vessels) |
| Referred pain shoulder | Phrenic nerve compression/irritation (C3-C5) from pericardium, diaphragm, or gallbladder |
| Hazard of left brachiocephalic vein | Rises above manubrium in infants - injured by tracheostomy |
| Tension pneumothorax | Mediastinal shift AWAY from the side of pneumothorax |
Sources: Gray's Anatomy for Students (Chapters 3 & 6), Fischer's Mastery of Surgery 8e (Chapter 238), Imaging Anatomy Vol. 3
This is a shared conversation. Sign in to Orris to start your own chat.