Coagulation cascade and how it affects bleeding
Reading File
Finding Sources
Searching Images
coagulation cascade intrinsic extrinsic pathway diagram
Searching the Web
coagulation cascade intrinsic extrinsic pathway hemostasis 2024
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Loading Image
I now have comprehensive information from Robbins, Basic Medical Biochemistry, and Harrison's, plus excellent diagrams. Let me compile the full answer.
The Coagulation Cascade and Its Role in Bleeding
Overview
The coagulation cascade is a series of amplifying enzymatic reactions that culminate in deposition of an insoluble fibrin clot. Circulating coagulation factors exist as inactive plasma proteins (zymogens). Upon activation, each cleaves and activates the next factor in sequence — producing enormous amplification from a small initial stimulus to a large fibrin mesh. — Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 122
The Cascade Diagram (Traditional Model)
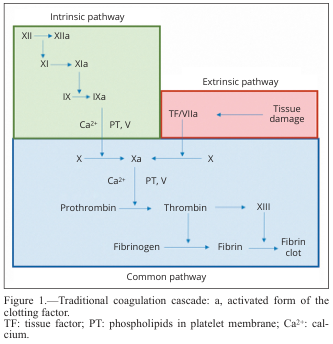
The Three Pathways
1. Extrinsic Pathway (Tissue Factor Pathway) — Primary In Vivo Initiator
| Step | Event |
|---|---|
| Vascular injury | Tissue factor (TF / Factor III) is exposed to blood |
| TF + Factor VII → Factor VIIa | Forms the extrinsic tenase complex |
| TF–VIIa complex | Activates Factor X → Xa directly |
| TF–VIIa complex | Also activates Factor IX → IXa (cross-activation) |
TF is constitutively expressed on sub-endothelial cells and is only exposed after tissue injury. This makes the extrinsic pathway the dominant initiator of coagulation in vivo. — Harrison's Principles of Internal Medicine 22E, p. 2401
Lab test: Prothrombin time (PT) — measures factors VII, X, V, II, and fibrinogen.
2. Intrinsic Pathway (Contact Activation Pathway)
| Step | Event |
|---|---|
| Negatively charged surfaces (collagen, glass in lab) | Activate Factor XII → XIIa |
| XIIa | Activates XI → XIa |
| XIa | Activates IX → IXa |
| IXa + Factor VIIIa + Ca²⁺ + phospholipid | Forms the intrinsic tenase complex |
| Intrinsic tenase complex | Activates Factor X → Xa |
The intrinsic tenase complex activates Factor X at a rate 50× faster than the extrinsic tenase complex, making it critical for the amplification phase of clotting, even though initiation comes from the extrinsic pathway. — Basic Medical Biochemistry, 6e, p. 1557
Lab test: Partial thromboplastin time (PTT) — measures factors XII, XI, IX, VIII, X, V, II, and fibrinogen.
3. Common Pathway
Both pathways converge at Factor X activation:
| Step | Complex/Reaction |
|---|---|
| Xa + Va + Ca²⁺ + phospholipid | = Prothrombinase complex |
| Prothrombin (II) → Thrombin (IIa) | Key enzymatic step |
| Thrombin cleaves fibrinogen (I) → Fibrin (Ia) | Fibrin monomers polymerize |
| Thrombin activates Factor XIII → XIIIa | XIIIa cross-links fibrin covalently → stable clot |
Thrombin — The Master Regulator
Thrombin (Factor IIa) is the most important coagulation factor. Its actions extend far beyond fibrin generation:
- Fibrin formation — cleaves fibrinogen; activates Factor XIII to cross-link fibrin
- Amplification feedback — activates Factors V, VIII, XI (positive feedback loops)
- Platelet activation — via protease-activated receptor 1 (PAR-1), linking coagulation to primary hemostasis
- Proinflammatory effects — PAR activation on endothelial cells and leukocytes promotes PDGF release, tissue repair, angiogenesis
- Anticoagulant switch — when thrombin binds normal endothelium, it activates Protein C (via thrombomodulin), which then inactivates Factors Va and VIIIa, preventing clot extension beyond the injury site
— Robbins, Cotran & Kumar, p. 123
Reaction Assembly Requirements
Each step requires assembly of enzyme + substrate + cofactor on a negatively charged phospholipid surface (provided by activated platelets):
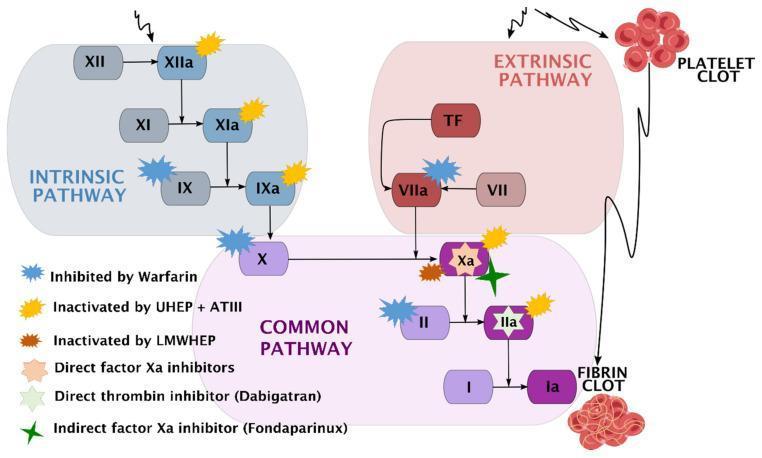
- Calcium ions (Ca²⁺) — bind γ-carboxylated glutamic acid residues on Factors II, VII, IX, and X
- Vitamin K — cofactor for the γ-carboxylation enzyme; antagonized by warfarin
- Phospholipids — platelet surface scaffold
How Anticoagulant Mechanisms Limit Bleeding (and Prevent Thrombosis)
| Mechanism | Action |
|---|---|
| Antithrombin (AT) | Inhibits thrombin, Xa, IXa, XIa, XIIa; enhanced by heparin |
| Tissue Factor Pathway Inhibitor (TFPI) | Blocks TF–VIIa–Xa complex |
| Protein C / Protein S | Thrombomodulin-bound thrombin activates Protein C → inactivates Va and VIIIa |
| Simple dilution | Blood flow washes away activated factors |
— Harrison's, p. 2405
Coagulation Cascade with Anticoagulant Drug Targets
Coagulation Cascade and Fibrinolysis
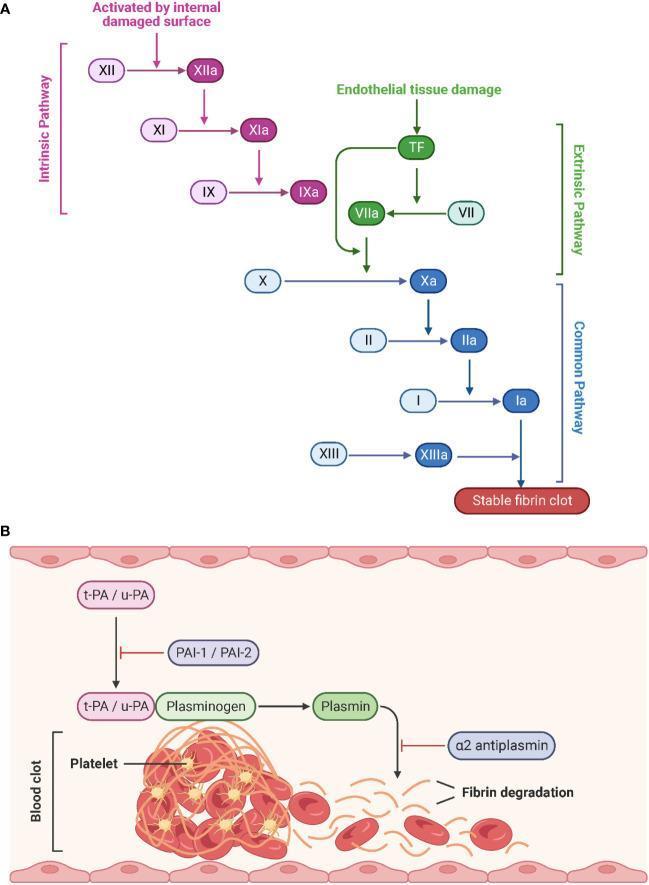
After clot formation, fibrinolysis dissolves the clot: tissue plasminogen activator (t-PA) and urokinase (u-PA) convert plasminogen → plasmin, which degrades fibrin into D-dimers. This is inhibited by PAI-1, PAI-2, and α2-antiplasmin.
How Factor Deficiencies Cause Bleeding
| Factor Deficient | Pathway Affected | Clinical Effect |
|---|---|---|
| Factor VIII (Hemophilia A) | Intrinsic (cofactor for IXa) | Severe bleeding |
| Factor IX (Hemophilia B) | Intrinsic | Severe bleeding |
| Factor VII | Extrinsic | Moderate–severe bleeding |
| Factor V or X | Common pathway | Moderate–severe bleeding |
| Prothrombin (II) | Common pathway | Likely incompatible with life |
| Factor XI | Intrinsic | Only mild bleeding — because thrombin feedback can activate XI |
| Factor XII | Intrinsic (contact) | No clinical bleeding — Hageman factor critical in lab but not in vivo |
| Fibrinogen (I) | End product | Bleeding + poor clot quality |
| Factor XIII | Cross-linking | Clot forms but is mechanically unstable |
| Vitamin K deficiency / Warfarin | Factors II, VII, IX, X | Prolonged PT and PTT |
— Robbins, Cotran & Kumar, p. 183
Key insight: Factor XI deficiency causes only mild bleeding despite being in the "intrinsic pathway" — because thrombin itself provides positive feedback to activate XI. This explains why the classic lab-based intrinsic/extrinsic model does not fully represent in vivo hemostasis.
Lab Tests Summary
| Test | Pathway Assessed | Prolonged By |
|---|---|---|
| PT (Prothrombin Time) | Extrinsic + Common | Factor VII, X, V, II deficiency; warfarin |
| PTT (Partial Thromboplastin Time) | Intrinsic + Common | Factors VIII, IX, XI, XII deficiency; heparin; lupus anticoagulant |
| Thrombin Time (TT) | Fibrinogen → Fibrin step | Hypofibrinogenemia, direct thrombin inhibitors |
| D-dimer | Fibrinolysis | DIC, PE, DVT (elevated when fibrin being degraded) |
In summary: The coagulation cascade is a tightly regulated amplification system where vascular injury exposes tissue factor, triggering the extrinsic pathway to rapidly generate small amounts of thrombin. Thrombin then amplifies its own production via the intrinsic pathway, ultimately converting fibrinogen to a stable cross-linked fibrin clot. Deficiencies in any factor — especially VIII, IX, X, V, or prothrombin — impair this cascade and cause bleeding disorders proportional to the factor's importance in amplification.
This is a shared conversation. Sign in to Orris to start your own chat.