Brachial plexus
Reading File
Finding Sources
Searching the Web
brachial plexus anatomy overview roots trunks divisions cords branches
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Reading File
Here is a thorough overview of the brachial plexus, drawn from Gray's Anatomy for Students and Bradley & Daroff's Neurology.
Brachial Plexus

Fig. 7.52A - Major components of the brachial plexus in the neck and axilla (Gray's Anatomy for Students)
Formation & Overview
The brachial plexus is a somatic nerve plexus formed by the anterior rami of C5-C8 and most of T1. It originates in the neck (posterior triangle), passes laterally and inferiorly over rib I, and enters the axilla. The plexus runs between the anterior and middle scalene muscles at its root level, then travels with (and surrounds) the axillary artery in the axilla. The roots receive gray rami communicantes from the sympathetic trunk, distributing postganglionic sympathetic fibers to the upper limb.
The classic mnemonic for its organization: R - T - D - C - B (Roots, Trunks, Divisions, Cords, Branches)
Step-by-Step Structure
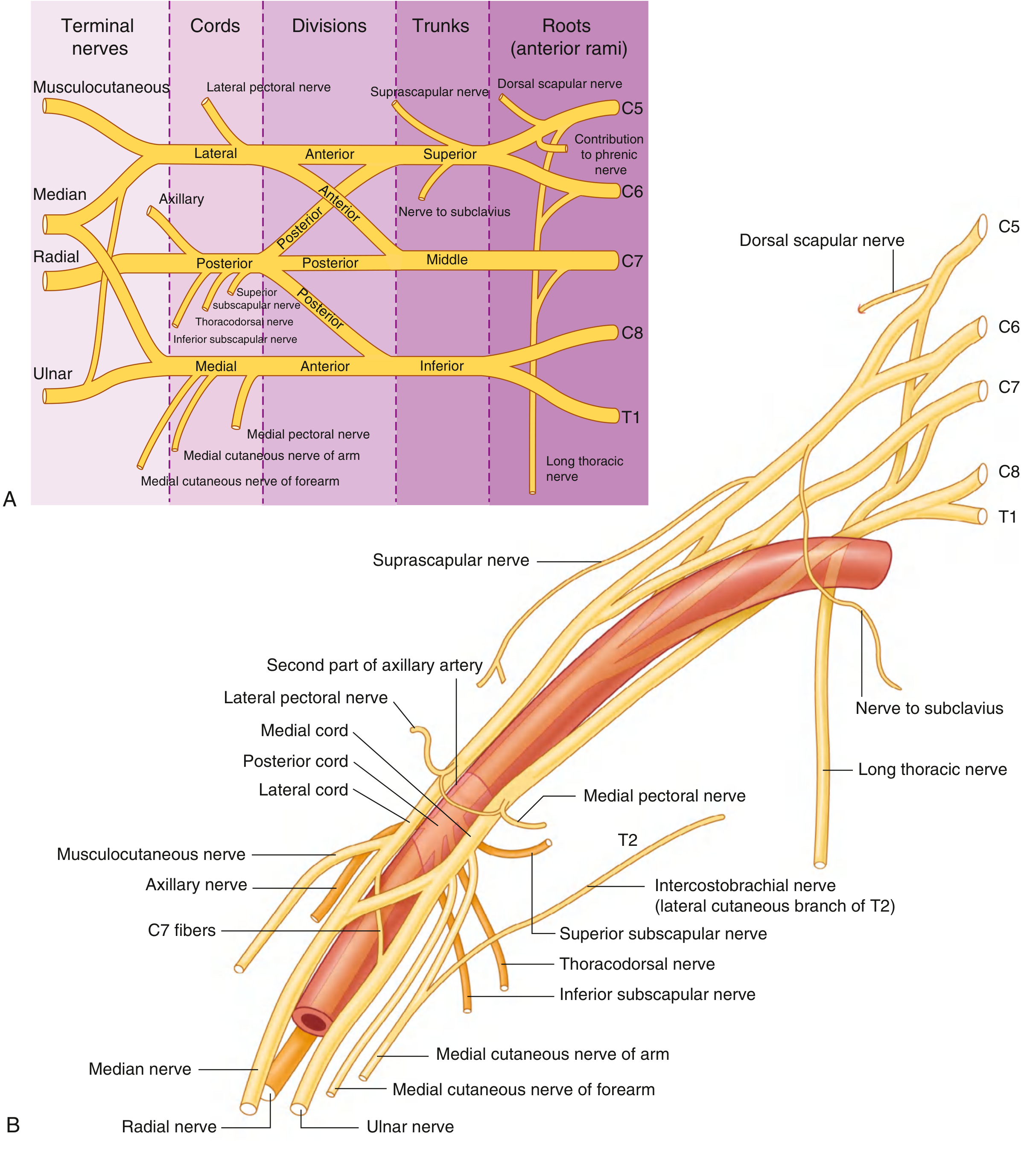
Fig. 7.53 - Schematic of all branches, and relationships to the axillary artery (Gray's Anatomy for Students)
1. Roots (5 roots)
The anterior rami of C5, C6, C7, C8, and T1. They emerge between the anterior and middle scalene muscles.
2. Trunks (3 trunks)
| Trunk | Formation |
|---|---|
| Superior trunk | C5 + C6 |
| Middle trunk | C7 alone |
| Inferior trunk | C8 + T1 |
The inferior trunk lies on rib I, posterior to the subclavian artery. The middle and superior trunks are more superior.
3. Divisions (6 divisions)
Each trunk splits into an anterior and a posterior division (total 6). No peripheral nerves branch directly from the divisions.
- Anterior divisions - supply anterior (flexor) compartments
- Posterior divisions - supply posterior (extensor) compartments
4. Cords (3 cords)
Named by their position relative to the 2nd part of the axillary artery:
| Cord | Formation | Roots | Position |
|---|---|---|---|
| Lateral cord | Anterior divisions of superior + middle trunks | C5-C7 | Lateral to axillary a. |
| Medial cord | Anterior division of inferior trunk | C8-T1 | Medial to axillary a. |
| Posterior cord | All three posterior divisions | C5-T1 | Posterior to axillary a. |
5. Terminal Branches (5 major)
| Nerve | Origin | Roots | Key Supply |
|---|---|---|---|
| Musculocutaneous | Lateral cord | C5-C7 | Anterior arm muscles; lateral forearm skin |
| Median | Lateral + medial cords (two roots) | C5-T1 | Most anterior forearm muscles; thenar muscles; lateral 3.5 fingers |
| Ulnar | Medial cord | C8-T1 | Intrinsic hand muscles; medial 1.5 fingers |
| Axillary | Posterior cord | C5-C6 | Deltoid, teres minor; lateral shoulder skin |
| Radial | Posterior cord | C5-T1 | All posterior arm & forearm muscles; posterior arm/forearm/hand skin |
The musculocutaneous nerve, lateral root of median, median nerve, medial root of median, and ulnar nerve form a characteristic "M" shape over the 3rd part of the axillary artery - a key anatomical landmark.
Collateral (Pre-Terminal) Branches
These arise proximal to the cords:
From the roots:
- Dorsal scapular nerve (C5) - rhomboids major & minor
- Long thoracic nerve (C5-C7) - serratus anterior; injury causes winging of the scapula
From the superior trunk:
- Suprascapular nerve (C5-C6) - supraspinatus, infraspinatus
- Nerve to subclavius (C5-C6) - subclavius
From the lateral cord:
- Lateral pectoral nerve (C5-C7) - pectoralis major (and minor via communication)
From the medial cord:
- Medial pectoral nerve (C8-T1) - pectoralis major and minor
- Medial cutaneous nerve of arm (C8-T1) - medial distal arm skin
- Medial cutaneous nerve of forearm (C8-T1) - medial forearm skin
From the posterior cord:
- Superior subscapular nerve - subscapularis
- Thoracodorsal nerve - latissimus dorsi
- Inferior subscapular nerve - subscapularis, teres major
- (plus axillary and radial as terminal branches above)
Clinical: Brachial Plexus Injuries
Injuries are classified by level of damage:
Erb's Palsy (Upper trunk - C5, C6)
- Typically from shoulder dystocia at birth, or violent downward traction of the shoulder in adults
- "Waiter's tip" posture: arm adducted, medially rotated, forearm pronated
- Loss of: shoulder abduction (deltoid), elbow flexion (biceps), forearm supination
- Absent biceps reflex
Klumpke's Palsy (Lower trunk / Inferior trunk - C8, T1)
- Caused by forced upward traction of the arm (e.g., grabbing a branch to break a fall)
- Weakness/paralysis of intrinsic hand muscles; clawing of ring and little fingers
- Absent grasp reflex
- May be accompanied by Horner's syndrome (ptosis, miosis, anhidrosis) if T1 root avulsed - due to damage to sympathetic fibers
Pancoast Tumor (C8-T1)
- Apical lung tumor infiltrating the inferior trunk; classically produces Horner's syndrome + pain down the medial arm/forearm + intrinsic hand weakness
Total plexus palsy (C5-T1)
- Flail arm with complete anesthesia of the limb
- Usually from high-energy trauma (motorcycle accidents)
Neonatal brachial plexus injury
- Erb palsy (C5-C6) is most common; deficits persist in ~25% of cases
- Surgical reconstruction should be considered if no spontaneous recovery at 3 months (Bradley & Daroff's Neurology)
Key clinical tools
- Electrodiagnostics (NCS/EMG) - assess latency of muscle contraction with nerve stimulation, localize level of injury
- MRI or CT myelography - identifies nerve root avulsions (preganglionic vs postganglionic)
- Avulsion injuries (preganglionic) cannot regenerate; stretch/rupture injuries (postganglionic) may recover spontaneously or with nerve grafting
Anatomical Relations
-
Supraclavicular part (roots + trunks): in the posterior triangle of the neck, between anterior and middle scalene muscles, above rib I
-
Infraclavicular part (cords + branches): in the axilla, arranged around the axillary artery
-
Compression can occur between rib I and clavicle or below pectoralis minor (thoracic outlet syndrome)
-
Gray's Anatomy for Students, p. 858-866
-
Bradley & Daroff's Neurology in Clinical Practice, p. 2870
This is a shared conversation. Sign in to Orris to start your own chat.