Dka detailed
Reading File
Finding Sources
Searching PubMed
"diabetic ketoacidosis"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive textbook content from Rosen's Emergency Medicine and Goldman-Cecil Medicine to write a detailed DKA review. Let me compile everything:
Diabetic Ketoacidosis (DKA) - Detailed Review
Definition and Diagnostic Triad
DKA is defined by three fundamental biochemical features - the "DKA triad":
- D - Hyperglycemia (glucose >250 mg/dL) or known diabetes (euglycemic DKA can occur in up to 18% of cases, especially with SGLT-2 inhibitor use)
- K - Ketonemia/ketonuria (urine ketones 2+ or higher, or serum beta-hydroxybutyrate ≥3.0 mmol/L)
- A - Acidosis (arterial/venous pH <7.3, serum bicarbonate <18 mmol/L)
Goldman-Cecil Medicine, p. 2483
Severity Classification
| Parameter | Mild | Moderate | Severe |
|---|---|---|---|
| Blood glucose (mg/dL) | >250 | >250 | >250 |
| pH | 7.25-7.30 | 7.00-7.25 | <7.00 |
| Serum HCO3 (mEq/L) | 15-18 | 10-14 | <10 |
| Anion gap | >10 | >12 | >12 |
| Mental status | Alert | Drowsy | Stupor/Coma |
Pathophysiology
The core driver is combined insulin deficiency + counter-regulatory hormone excess (glucagon, catecholamines, cortisol, growth hormone).
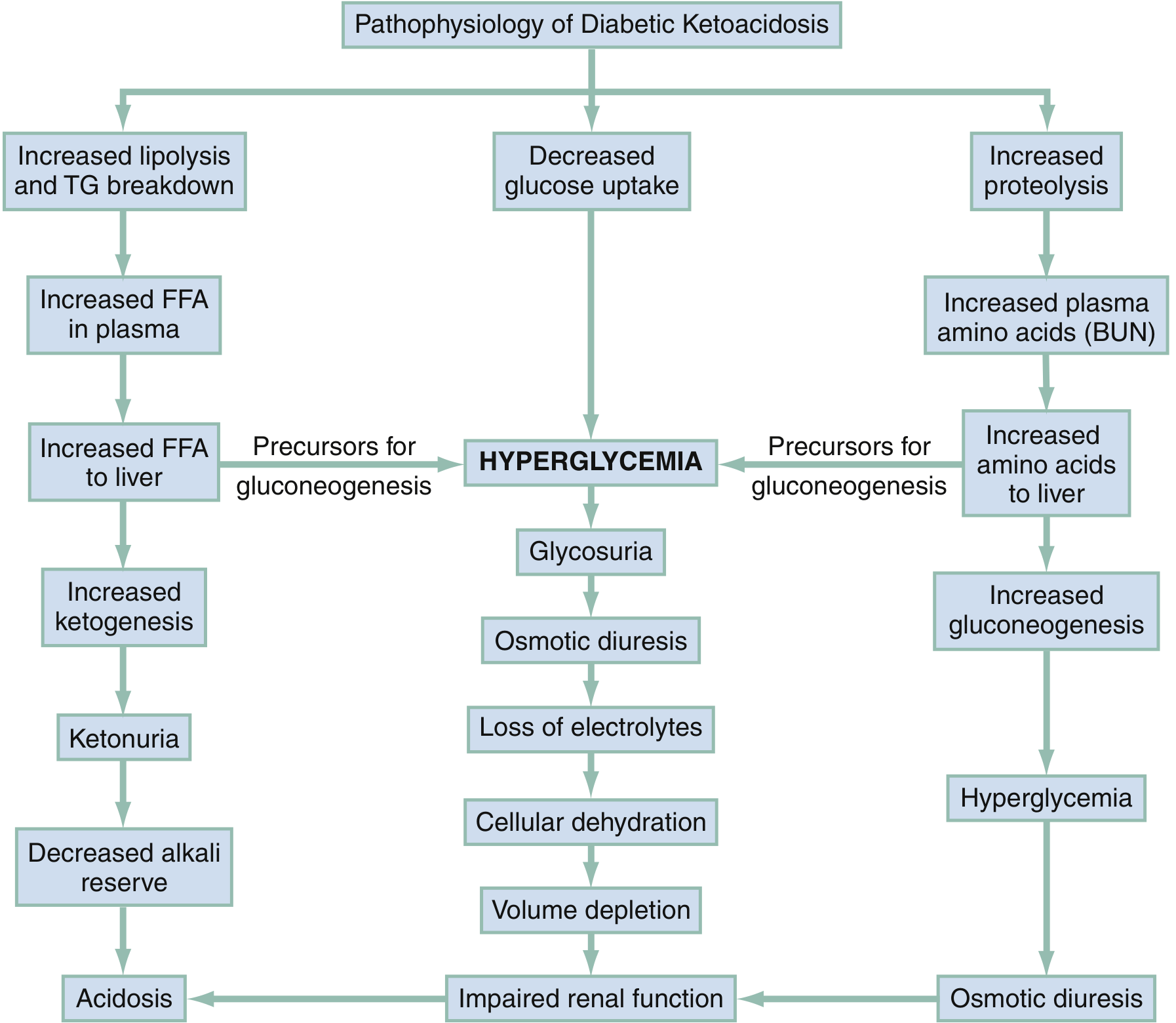
Fig. Syndrome of DKA - Rosen's Emergency Medicine
Three parallel metabolic derangements occur simultaneously:
1. Ketogenesis (Left pathway)
- Insulin deficiency triggers lipolysis in adipose tissue
- Free fatty acids (FFAs) flood the liver
- Hepatic oxidation of FFAs produces ketone bodies: beta-hydroxybutyrate (predominant), acetoacetate, and acetone
- Decreased peripheral ketone utilization (cells act as in starvation) further accumulates ketones
- Consumed bicarbonate leads to anion gap metabolic acidosis
2. Hyperglycemia (Central pathway)
- Decreased glucose uptake by peripheral tissues
- Glycosuria exceeds the renal threshold
- Osmotic diuresis - glucose in renal tubules drags water, Na+, K+, Mg2+, Ca2+, PO4 into urine
- Combined with poor intake and vomiting: profound dehydration and electrolyte loss
- Cellular dehydration + volume depletion lead to impaired renal function
3. Gluconeogenesis (Right pathway)
- Insulin deficiency accelerates proteolysis in muscle
- Amino acids, lactate, and pyruvate are released to the liver
- Hepatic conversion to glucose amplifies hyperglycemia
- Increased gluconeogenesis competes with impaired glucose uptake
- Continued osmotic diuresis worsens the cycle
Rosen's Emergency Medicine, p. 2542; Goldman-Cecil Medicine, p. 2483
Precipitating Factors
| Most Common | Other Factors |
|---|---|
| Infections (UTI, pneumonia) | Cerebrovascular accident |
| Inadequate insulin / nonadherence | Acute pulmonary embolism |
| New-onset diabetes | Acute pancreatitis |
| Acute coronary syndrome | Alcohol intoxication |
| Unknown | Severe burns |
| Drugs: corticosteroids, clozapine, olanzapine, cocaine, lithium, sympathomimetics, thiazides, SGLT-2 inhibitors | |
| Cushing syndrome, thyrotoxicosis, acromegaly |
Approximately 25% of DKA episodes occur in patients with previously undiagnosed diabetes.
Goldman-Cecil Medicine, p. 2483
Clinical Features
Symptoms (Gradual onset over hours to days)
- Classic triad of diabetes: polyuria, polydipsia, polyphagia
- Weakness, lethargy, malaise
- Nausea, vomiting, anorexia
- Abdominal pain - present in ~50% of patients (especially children, usually idiopathic from gastric distension/liver capsule stretch; in adults it more often indicates an actual abdominal precipitant)
- Visual blurring, weight loss
Physical Examination
| Finding | Mechanism |
|---|---|
| Kussmaul breathing (deep, rapid) | Respiratory compensation for metabolic acidosis |
| Fruity/acetone odor on breath | Exhaled acetone |
| Tachycardia | Dehydration |
| Hypotension / orthostatic changes | Volume depletion |
| Dry skin and mucous membranes | Dehydration |
| Depressed sensorium / coma | Hyperosmolarity + acidosis |
| Elevated temperature | Suggests infection (not DKA itself) |
Rosen's Emergency Medicine, p. 2543; Goldman-Cecil Medicine, p. 2484
Laboratory Findings and Interpretation
Key Workup
- ABG or VBG: pH, HCO3, pCO2
- BMP/CMP: glucose, Na+, K+, Cl-, HCO3-, BUN, creatinine
- Serum/urine ketones (beta-hydroxybutyrate preferred)
- CBC with differential (band neutrophilia suggests infection; leukocytosis reflects ketosis, not necessarily infection)
- Urinalysis (confirm ketonuria + screen for UTI precipitant)
- ECG (assess for hypo/hyperkalemia, ACS as precipitant)
- Lipase if pancreatitis suspected (must be >3x upper normal to diagnose pancreatitis)
- Cultures if infection suspected
Critical Lab Interpretations
Sodium:
- Measured Na+ is often falsely low due to dilutional hyponatremia from osmotic water shift and hypertriglyceridemia (pseudohyponatremia)
- Corrected Na+ formula: Add 1.6 mEq/L per 100 mg/dL glucose above normal
- Example: Na+ 130 mEq/L with glucose 700 mg/dL → corrected Na+ = 130 + (6 × 1.6) = 139.6 mEq/L
Potassium:
- Initial serum K+ is usually normal or high despite total body deficit (acidosis shifts K+ out of cells; H+ enters cells in exchange for K+)
- Corrected K+ formula: Subtract 0.6 mEq/L per 0.1 decrease in pH below normal
- Example: K+ = 5.0 mEq/L with pH 6.94 → corrected K+ = 5.0 - (6 × 0.6) = ~2.0 mEq/L (severe hypokalemia)
- With insulin therapy and acidosis correction, K+ shifts back intracellularly - life-threatening hypokalemia can develop rapidly
Anion gap:
- Elevated due to accumulation of beta-hydroxybutyrate and acetoacetate
- AG = Na+ - (Cl- + HCO3-), normal is 8-12 mEq/L
Ketone testing pitfall:
- Nitroprusside reagent strips only detect acetoacetate (weakly) and acetone
- Beta-hydroxybutyrate does NOT react with nitroprusside
- In severe DKA, the BHB:acetoacetate ratio is high (intracellular acidosis shifts equilibrium toward BHB) - can give a falsely low ketone reading
- After insulin treatment, BHB converts to acetoacetate - this can appear as worsening ketosis when acidosis is actually improving
Other findings:
- WBC is often elevated - reflects degree of ketosis, not necessarily infection
- Serum creatinine may be falsely elevated on autoanalyzer
- Serum amylase often elevated (non-pancreatic origin) - do not diagnose pancreatitis on amylase alone; use lipase
Rosen's Emergency Medicine, p. 2543-2544; Goldman-Cecil Medicine, p. 2484
Average Fluid and Electrolyte Deficits (Severe DKA)
| Body Weight | Water (mL/kg) | Na+ (mEq/kg) | K+ (mEq/kg) | Cl- (mEq/kg) | Phosphorus (mEq/kg) |
|---|---|---|---|---|---|
| ≤10 kg | 100-120 | 8-10 | 5-7 | 6-8 | 3 |
| 10-20 kg | 80-100 | 8-10 | 5-7 | 6-8 | 3 |
| ≥20 kg | 70-90 | 8-10 | 5-7 | 6-8 | 3 |
Rosen's Emergency Medicine, Table 115.3
Treatment
Step 1 - Airway
- Avoid intubation when possible - patients have a tremendous respiratory drive; matching this with a ventilator is difficult
- Intubation is necessary for comatose/vomiting patients
- Once intubated: maintain hyperventilation to prevent worsening acidosis
Step 2 - Fluid Resuscitation
Adults:
- If in hypovolemic shock: isotonic crystalloid as rapidly as possible until systolic BP ≥80 mmHg
- If markedly dehydrated but not in shock: 1 L NS in the first hour, then 2 L total over 1-3 hours
- Follow with 0.45% NS (hypotonic solution) at a slower rate
- When glucose drops to ≤300 mg/dL: switch IV fluid to D5W/0.45% NS (to prevent hypoglycemia while continuing insulin)
Children:
- Initial bolus: 20 mL/kg NS in the first hour
- Adjust rate to achieve urine output of 1-2 mL/kg/h
Recent evidence (2024): A systematic review and meta-analysis found that balanced electrolyte solutions (e.g., Plasmalyte) result in faster DKA resolution compared to 0.9% normal saline, likely by avoiding the hyperchloremic metabolic acidosis caused by large-volume NS. [PMID: 38925619]
Step 3 - Potassium Replacement
| Serum K+ | Action |
|---|---|
| <3.3 mEq/L | DO NOT give insulin yet - Replace K+ first (20-40 mEq/h IV) until K+ ≥3.3 |
| 3.3-5.5 mEq/L | Add 20-40 mEq KCl per liter of IV fluid |
| >5.5 mEq/L | Hold K+ replacement; monitor closely |
This is one of the most critical steps - giving insulin to a severely hypokalemic patient can cause fatal cardiac arrhythmias.
Step 4 - Insulin
- Start insulin only after K+ ≥3.3 mEq/L is confirmed
- Regular insulin IV infusion: 0.1 unit/kg/hour
- Do not give an IV bolus of insulin (increases risk of hypokalemia and hypoglycemia without added benefit in most adults)
- Target: blood glucose reduction of 50-75 mg/dL/hour
- Continue insulin infusion until anion gap closes and ketoacidosis resolves (not just until glucose normalizes)
- Add dextrose to IV fluids when glucose ≤300 mg/dL to allow continued insulin infusion
Recent evidence (2026): Early subcutaneous basal insulin overlapping with IV insulin infusion may reduce hypoglycemia risk and shorten total treatment time. [PMID: 41208563]
Recent evidence (2024): Subcutaneous insulin protocols have shown comparable outcomes to continuous IV infusion in adults with uncomplicated DKA in select studies. [PMID: 39090718]
Step 5 - Phosphorus
- Routine phosphorus replacement is generally not recommended
- Replace only if severe hypophosphatemia with cardiac/skeletal muscle weakness or respiratory depression
Step 6 - Magnesium
- Correct with 1-2 g MgSO4 IV
- Note: serum magnesium levels may not accurately reflect body stores
Step 7 - Bicarbonate
- Not routinely recommended
- Consider only if pH <6.9 and hemodynamic instability persists despite fluids
- Risks: paradoxical CNS acidosis, hypokalemia, sodium overload, delayed ketone clearance
Step 8 - Identify and Treat the Precipitant
- Blood/urine cultures if infection suspected
- ECG and troponins for ACS
- Head CT if neurologic deficit present
Step 9 - Monitoring (Meticulous Flow Sheets)
- Vital signs hourly
- Fluid intake and urine output
- Blood glucose every 1-2 hours
- Electrolytes (K+, HCO3-, Cl-, anion gap) every 2-4 hours
- pH until normalized
Rosen's Emergency Medicine, Box 115.1 and pp. 2544-2545; Goldman-Cecil Medicine, p. 2484
Resolution Criteria
DKA is considered resolved when all three are met:
- Blood glucose <200-250 mg/dL
- Serum bicarbonate ≥15 mEq/L
- Anion gap closed (<12 mEq/L) OR venous pH >7.3
At resolution, transition to subcutaneous insulin (give SQ dose 1-2 hours before stopping the infusion to prevent rebound ketosis).
Complications of DKA and Its Treatment
| Complication | Mechanism |
|---|---|
| Cerebral edema | Most feared in children; rapid osmotic shifts during treatment |
| Hypokalemia | Intracellular K+ shift with insulin + acidosis correction |
| Hypoglycemia | Continued insulin without adequate glucose supplementation |
| Hyperchloremic non-AG acidosis | Large-volume 0.9% NS administration |
| Aspiration pneumonia | Altered sensorium + vomiting |
| Thromboembolism | Hypercoagulable state + dehydration |
| Acute kidney injury | Prerenal from severe dehydration |
Special Considerations
Euglycemic DKA
- Blood glucose ≤300 mg/dL despite full ketoacidosis
- Increasingly recognized with SGLT-2 inhibitors (canagliflozin, empagliflozin, dapagliflozin)
- Mechanism: SGLT-2 inhibitors increase urinary glucose excretion + increase glucagon - can trigger ketogenesis without marked hyperglycemia
- Must maintain high suspicion in diabetic patients on these drugs presenting with acidosis
DKA in Pregnancy
- More severe and faster progression (reduced buffering capacity)
- Can occur at lower glucose levels
- Fetal mortality is high (20-35%) - requires urgent management and fetal monitoring
Euglycemic DKA vs. Alcoholic Ketoacidosis
- Alcoholic ketoacidosis: euglycemia or hypoglycemia, history of recent alcohol binge + sudden cessation, elevated BHB, often with alkalemia (from vomiting)
- DKA: hyperglycemia, history of diabetes
DKA vs. Hyperosmolar Hyperglycemic State (HHS)
| Feature | DKA | HHS |
|---|---|---|
| Typical diabetes type | Type 1 (also Type 2) | Type 2 |
| Onset | Rapid (hours) | Gradual (days-weeks) |
| Blood glucose | 250-600 mg/dL | Often >600 mg/dL |
| Ketosis | Marked | Absent or mild |
| pH | <7.3 | >7.3 (rarely <7.3) |
| Serum HCO3 | <18 mEq/L | >18 mEq/L |
| Anion gap | Wide | Normal or mildly elevated |
| Serum osmolality | Mildly elevated | >320 mOsmol/L |
| Mental status change | Variable | Correlates with osmolality |
| Mortality | 1-5% | 10-20% |
The distinction is not always clear - mixed DKA/HHS presentations exist, particularly in Type 2 diabetes with severely depressed insulin secretion.
Goldman-Cecil Medicine, p. 2484
Key Mnemonics
Precipitants of DKA - "5 I's":
- Infection
- Insulin non-adherence
- Initial presentation (new-onset T1DM)
- Ischemia (ACS, stroke)
- Intoxication / Drugs
Treatment - "FIFE":
- Fluids (isotonic first)
- Insulin (after K+ ≥3.3)
- Fix electrolytes (K+ especially)
- Find the precipitant
Sources:
Pneumothorax approach
Reading File
Finding Sources
Searching PubMed
"pneumothorax"[MeSH Terms] AND management
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive material. Let me compile the full detailed pneumothorax approach:
Pneumothorax - Detailed Clinical Approach
Definition
Pneumothorax is the accumulation of air in the pleural space, causing partial or complete lung collapse. It is present in 15-50% of significant chest trauma patients and is invariably present with transpleural penetrating injuries.
Classification
By Mechanism
| Type | Description | Key Feature |
|---|---|---|
| Simple (Closed) | No communication with atmosphere; no mediastinal shift | Air trapped in pleural space |
| Communicating (Open) | Chest wall defect with free air communication - "sucking chest wound" | Paradoxical breathing |
| Tension | Progressive air accumulation under pressure; one-way valve effect | Mediastinal shift + hemodynamic compromise |
| Occult | Not visible on CXR; detected only on CT | Increasingly common with widespread CT use |
By Etiology
| Category | Subtypes | Key Notes |
|---|---|---|
| Spontaneous - Primary (PSP) | No underlying lung disease | Tall, thin young males <30 yrs; subpleural blebs at apex |
| Spontaneous - Secondary (SSP) | Underlying lung disease (COPD most common) | More severe; poor reserve |
| Traumatic | Blunt or penetrating | Rib fracture, stab, gunshot |
| Iatrogenic | Central line, thoracentesis, biopsy, PPV | ~6% complication rate with thoracentesis |
| Catamenial | Menstruation-related; endometriosis | Recurrent right-sided PTX in women |
Pathophysiology
Simple PTX
- Rib fracture driven inward lacerates the visceral pleura, OR
- Alveolar rupture from sudden intra-alveolar pressure surge (blunt trauma at full inspiration with closed glottis), OR
- Spontaneous bleb rupture (apical subpleural bullae in PSP)
- Air enters the pleural space but no one-way valve - pressure equilibrates
Communicating (Open) PTX
- Chest wall defect creates direct atmosphere-pleural communication
- On inspiration: diaphragm contracts, negative pressure draws air through wound (not trachea) → involved lung collapses
- On expiration: small re-expansion through wound
- Creates large functional dead space and severe ventilatory disturbance
- Paradoxical lung movement
Tension PTX
- A one-way valve is created at the site of injury
- Air enters pleural space on each breath but cannot escape
- Progressive positive pressure builds up
- Mediastinum shifts to the contralateral side
- Compresses contralateral lung (reducing its ventilation)
- Compresses vena cava - impairs venous return to the heart
- Reduced cardiac output → hemodynamic collapse → DEATH if untreated
Rosen's Emergency Medicine, p. 466
Radiological Appearance
CXR - Simple/Spontaneous PTX (left image: A = 40% left-sided PTX, B = tension)
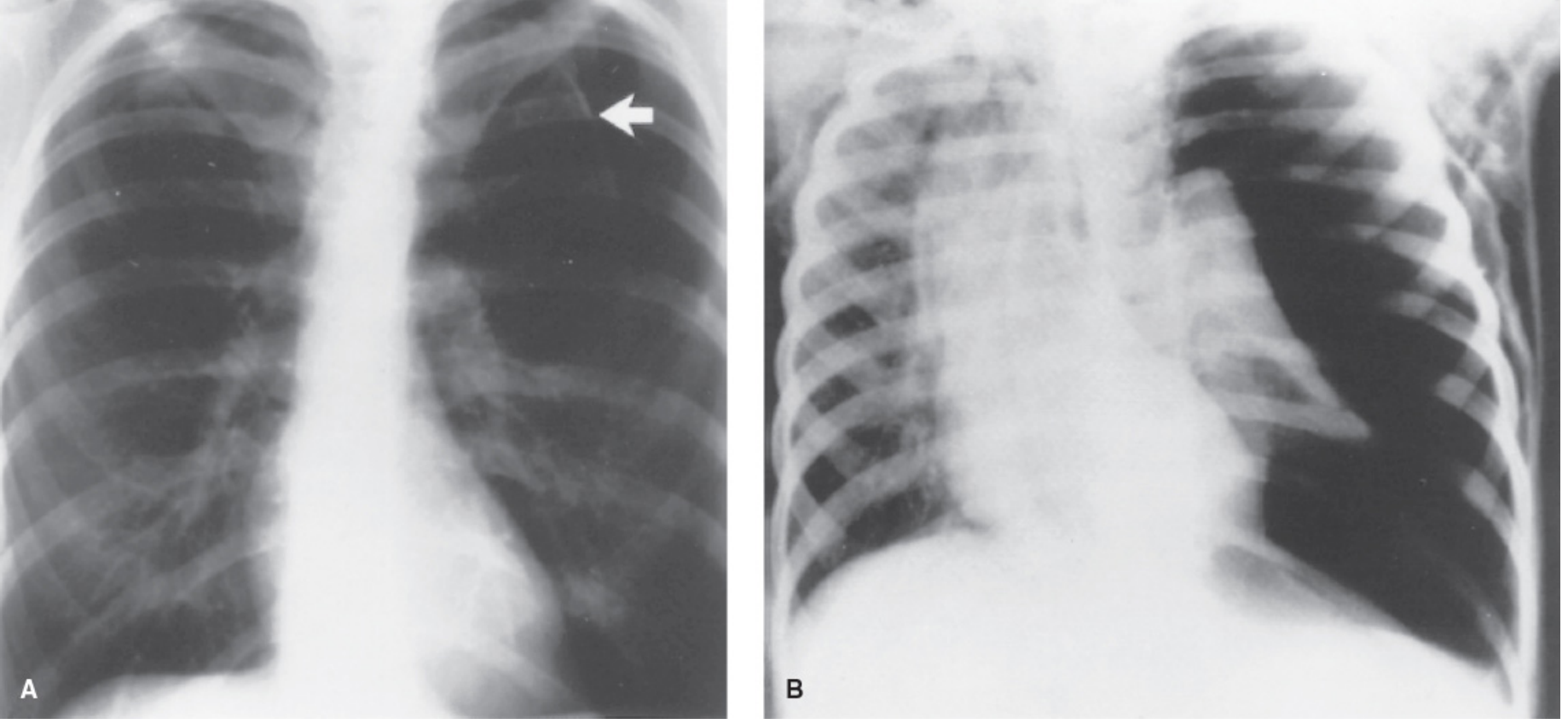
Figure 80.26 - Greenfield's Surgery. A: 40% left-sided spontaneous pneumothorax (arrow). B: Tension pneumothorax - virtual collapse of entire lung, mediastinal shift to contralateral side, contralateral lung compression, and subcutaneous air
CXR - Tension PTX (post-tube thoracostomy in intubated patient)

Fig. 37.9 - Rosen's Emergency Medicine. Resolution of tension PTX after left-sided tube thoracostomy
CXR Findings by Type:
| Feature | Simple PTX | Tension PTX |
|---|---|---|
| Visible pleural line | Yes | Yes (or complete collapse) |
| Lung collapse | Partial | Complete (involved side) |
| Tracheal deviation | None | Away from affected side |
| Mediastinal shift | None | Away from affected side |
| Contralateral lung | Normal | Compressed |
| Hemidiaphragm | Normal | Depressed/flattened (ipsilateral) |
Size assessment:
- Small: <20% or apex-to-cupola distance <3 cm
- Large: ≥20% or apex distance ≥3 cm
Occult PTX
- Not seen on CXR but visible on CT
- Increasingly diagnosed with routine CT trauma scans
- Stable, asymptomatic patients may be observed even on PPV in some cases
POCUS (Point-of-Care Ultrasound)
Ultrasound is fast, bedside, and avoids radiation - extremely useful in trauma bay.
| Sign | Meaning | Significance |
|---|---|---|
| Pleural sliding (lung sliding on B-mode) | Visceral and parietal pleura in apposition and moving | EXCLUDES pneumothorax at that location |
| Sea-shore sign (M-mode) | Normal linear + granular pattern at pleural level | Normal; pleura moving |
| Bar code / Stratosphere sign (M-mode) | Uniform linear pattern throughout (A-lines only, no movement) | Absent pleural sliding - suggests PTX |
| B-lines | Vertical hyperechoic lines from pleura | Lung in contact with pleura - excludes PTX |
| Lung pulse | Cardiac pulsations transmitted through lung | Lung in contact with chest wall - excludes PTX |
| Lung point | Transition from sliding to no-sliding at one location | Highly specific for PTX - marks the edge of the pneumothorax |
The lung point is the most specific ultrasound sign for pneumothorax. Its location allows estimation of PTX size.
Murray & Nadel's Respiratory Medicine, p. 1100
Clinical Features
Symptoms
- Acute pleuritic chest pain - sudden onset, ipsilateral, sharp
- Dyspnea - proportional to PTX size and underlying reserve
- In PSP: symptoms can range from minimal to severe; most occur at rest
- Polyuria, polydipsia are NOT features (those are DKA)
- 50% of PSP patients have minimal symptoms despite significant PTX
Physical Examination
| Finding | Simple PTX | Tension PTX |
|---|---|---|
| Tachycardia | + | +++ |
| Respiratory distress | + | +++ |
| Hypotension | Absent | Present (late sign) |
| Tracheal deviation | Absent | Away from affected side |
| Chest expansion | Reduced ipsilateral | Markedly reduced ipsilateral |
| Percussion | Hyperresonant ipsilateral | Hyperresonant ipsilateral |
| Breath sounds | Reduced/absent ipsilateral | Absent ipsilateral |
| JVD (jugular venous distension) | Absent | Present |
| SpO2 | Mildly reduced | Severely reduced |
Not all signs are present in all patients with tension PTX. Clinical suspicion alone is sufficient to treat.
Diagnosis
Workup
- CXR - upright PA preferred; expiratory film increases sensitivity for small PTX
- CT chest - gold standard; detects occult PTX; defines size and underlying pathology (blebs, bullae)
- POCUS - rapid bedside diagnosis; particularly useful in trauma
- ABG - may show hypoxemia, respiratory alkalosis (or mixed in large PTX)
- ECG - may show sinus tachycardia; useful to exclude ACS
When NOT to wait for CXR
- Tension PTX is a clinical diagnosis - treat immediately based on clinical signs
- Do not delay decompression for imaging if hemodynamically unstable with clinical features of tension PTX
Management - Decision Framework
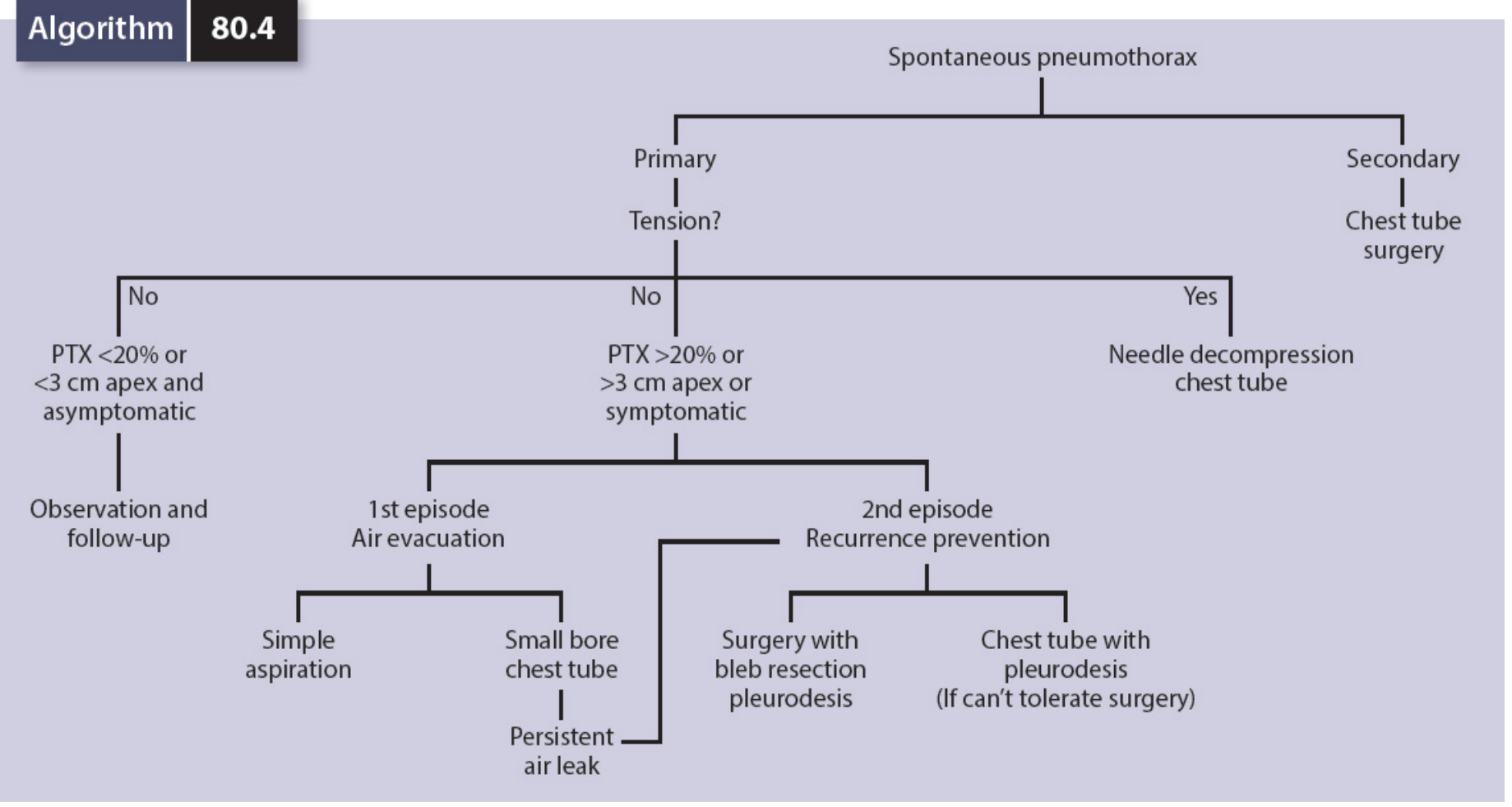
Algorithm 80.4 - Greenfield's Surgery (Spontaneous Pneumothorax Management)
1. Tension Pneumothorax - EMERGENCY
Do NOT wait for imaging. Act immediately.
Step 1 - Needle Decompression (Immediate)
- Large-bore needle (14-gauge), at least 5 cm in length
- Preferred site: 4th-5th intercostal space, midaxillary line (lateral approach - more reliable as chest wall is thinner here; avoids the mediastinum)
- Alternative site: 2nd intercostal space, midclavicular line (traditional ATLS, but higher failure rate due to chest wall thickness)
- Insert above the superior border of the rib (avoid neurovascular bundle below each rib)
- Escape of air + clinical improvement confirms diagnosis
2025 meta-analysis (PMID: 40383767): The 4th-5th ICS at the midaxillary line is now recommended over the 2nd ICS MCL due to greater reliability of reaching the pleural space, especially in obese patients. This aligns with updated ATLS and ETC guidelines.
Step 2 - Tube Thoracostomy (Definitive)
- Needle decompression is only a temporizing measure
- Chest tube (tube thoracostomy) is always required after needle decompression
- In the ED: finger thoracostomy then formal tube thoracostomy is equally or more expeditious than needle decompression
2. Simple/Closed Traumatic PTX
Indications for tube thoracostomy (Box 37.2):
- Traumatic cause (except: small, asymptomatic, apical stab wound)
- Moderate to large pneumothorax
- Respiratory symptoms regardless of size
- Expanding PTX after initial observation
- Recurrence after initial tube removal
- Requires mechanical ventilation
- Requires general anesthesia
- Associated hemothorax
Preferred insertion site:
- 4th or 5th intercostal space, midaxillary line (lateral approach)
- Preferred over the anterior 2nd ICS MCL: more efficient drainage, no visible cosmetic scar
- Tube size: Large (36-40 Fr in adults, 16-32 Fr in children) if hemothorax likely; small-bore for pure pneumothorax
Suction:
- Attach to water-seal drainage
- If significant air leak or large hemothorax: suction at 20-30 cm H2O
- Reduce to water-seal once air leak resolves
- 4-hour clamping trial before removal; confirm no re-expansion on CXR
Prophylactic antibiotics for chest tube:
- Cefazolin 1-2 g IV (within 1 hour of insertion) for trauma/hemothorax patients
- Vancomycin 1 g or clindamycin 600 mg if cephalosporin allergy
3. Primary Spontaneous PTX (PSP)
| Size | Symptoms | Management |
|---|---|---|
| Small (<20% or <3 cm apex) | Asymptomatic | Observation + supplemental O2 (speeds resorption), 4-6 hr repeat CXR |
| Large (≥20% or ≥3 cm) | Any | Air evacuation |
| Any | Symptomatic | Air evacuation |
Air Evacuation Options (first episode):
- Simple aspiration (needle aspiration): Associated with less pain, lower analgesia requirements, lower hospitalization rate; comparable immediate success to tube drainage
- Small-bore chest tube (pigtail or 24 Fr): Alternative; attach to Heimlich valve or underwater seal
Recurrence prevention (2nd episode or more):
- Patients with one PTX have a 30-50% chance of recurrence within 2 years
- After 2nd PTX: 50-80% chance of a 3rd
- Options:
- VATS (video-assisted thoracoscopic surgery) with bleb resection + mechanical pleurodesis - lowest recurrence rate; preferred if patient can tolerate surgery
- Chemical pleurodesis via chest tube (talc) - for patients who cannot tolerate surgery
Indications for surgery on FIRST episode:
- Life-threatening tension PTX
- Massive air leaks with incomplete re-expansion
- Air leak persisting >4 days after 2nd tube
- Associated hemothorax with complications
- Identifiable bullous disease
- Cystic fibrosis (failure of easy re-expansion)
2024 ERS/EACTS/ESTS Guideline (PMID: 38806203): Conservative management (observation) is increasingly favored for stable PSP. Invasive intervention is reserved for large or symptomatic cases.
4. Secondary Spontaneous PTX (SSP)
- More clinically severe due to poor underlying pulmonary reserve
- COPD, malignancy, cystic fibrosis, TB, PCP are common causes
- Observation has NO role - all SSP should undergo chest tube placement at first episode
- Pleurodesis evaluation recommended at first occurrence
- VATS may be more effective for adequate pleurodesis and evaluation of air leak sources
5. Communicating PTX (Open - "Sucking Chest Wound")
Prehospital:
- Apply a vented chest seal or 3-sided occlusive dressing immediately
- This converts the open PTX to a closed PTX
- Do NOT pack the wound - negative inspiratory pressure can suck the packing into the chest
- Monitor continuously for conversion to tension PTX (especially on PPV)
In-hospital:
- Formal tube thoracostomy
- PPV can be safely initiated after tube placement
- Surgical repair of chest wall defect
6. Iatrogenic PTX
- Treat according to the same algorithm as spontaneous PTX
- Small, asymptomatic, stable PTX in patients without underlying lung disease: observe
- Immediate aspiration after CT-guided lung biopsy: 85% success rate in avoiding chest tube
- ALL patients on PPV with iatrogenic PTX: chest tube (risk of tension PTX)
7. PTX on PPV (Mechanical Ventilation)
- Any pneumothorax in a ventilated patient should be drained - risk of rapid progression to tension PTX
- Earliest sign: increased peak airway pressure (increased resistance to ventilation)
- Loculated PTX: drain under US or CT guidance
- Do NOT delay decompression in deteriorating ventilated patient
Supplemental Oxygen
- Supplemental O2 accelerates pleural air resorption (increases gradient for nitrogen reabsorption)
- 100% O2 can increase resorption rate 3-4x
- Important adjunct in observation management of small PTX
Complications of PTX and Treatment
| Complication | Notes |
|---|---|
| Tension PTX | Can develop from any type; fatal without decompression |
| Hemopneumothorax | Requires large chest tube drainage |
| Re-expansion pulmonary edema | Rapid re-expansion of chronically collapsed lung; manage with supportive care |
| Persistent air leak (bronchopleural fistula) | >4 days → surgical evaluation |
| Empyema | Post-chest tube infection; prophylactic antibiotics reduce risk in trauma |
| Recurrence | 30-50% after first PSP within 2 years |
| Subcutaneous emphysema | Air tracking into soft tissues; usually self-limiting |
| Chest tube malposition | Assess with CXR; all drain holes must be within chest cavity |
Risk Factors for PSP Recurrence / SSP
- Smoking (most important modifiable risk factor)
- Male sex, tall thin body habitus
- Age <30 years (PSP)
- Marfan syndrome
- Prior history of PTX
- Underlying COPD, CF, malignancy (SSP)
Summary Management Algorithm
Pneumothorax
│
├── Tension PTX (hemodynamic instability, tracheal deviation, absent BS)?
│ → YES: Immediate needle decompression (4-5th ICS MAL) + chest tube
│
├── Traumatic PTX?
│ → Moderate/large or symptomatic or needs PPV: Chest tube (4-5th ICS MAL, large bore)
│ → Small, asymptomatic, stable, no PPV: Observe x 4-6 hrs + repeat CXR
│
├── Primary Spontaneous PTX?
│ → Small (<3 cm apex) + asymptomatic: Observe + O2 + follow-up CXR
│ → Large or symptomatic, 1st episode: Simple aspiration or small chest tube
│ → 2nd episode or persistent leak: VATS/pleurodesis
│
├── Secondary Spontaneous PTX?
│ → All cases: Chest tube + pleurodesis evaluation (VATS preferred)
│
└── Communicating PTX?
→ Prehospital: 3-sided/vented dressing; In-hospital: chest tube + surgical repair
Sources:
- Rosen's Emergency Medicine: Concepts and Clinical Practice, Chapter 37, pp. 466-468
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, Chapter 10, pp. 2613-2625
- Mulholland and Greenfield's Surgery: Scientific Principles and Practice, 7e, Chapter 80, pp. 4342-4343
- Murray & Nadel's Textbook of Respiratory Medicine, Chapter 23, pp. 1086-1105
- 2024 ERS/EACTS/ESTS Practice Guideline - spontaneous PTX management: PMID 38806203
- 2025 Meta-analysis on needle decompression site for tension PTX: PMID 40383767
Can you always give reffrances from harrisons
Finding Sources
Yes - Harrison's Principles of Internal Medicine, 22nd Edition (2025) is in the library. From now on, I will always prioritize Harrison's as the primary reference source for your questions.
A couple of things to note:
- Harrison's is primarily an internal medicine textbook, so it covers medical topics extremely well - DKA, pneumothorax (medical aspects), cardiology, nephrology, infectious disease, endocrinology, neurology, etc.
- For surgical procedures, emergency techniques (e.g., chest tube insertion technique), or highly specialized surgical content, I may still supplement with a procedural textbook (like Rosen's or Roberts & Hedges') since Harrison's doesn't cover those in depth - but I'll always cite Harrison's first and foremost.
Just ask your next question and I'll pull directly from Harrison's 22e!
This is a shared conversation. Sign in to Orris to start your own chat.