Simple pathogenesis of hurshprungs disease
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a simple breakdown of the pathogenesis of Hirschsprung's disease, sourced from Robbins Pathologic Basis of Disease and Sabiston Textbook of Surgery:
Hirschsprung's Disease - Pathogenesis
The Core Problem
Hirschsprung's disease (also called congenital aganglionic megacolon) is caused by the absence of ganglion cells in the distal bowel wall. This is not something acquired - it is a developmental failure during fetal life.
Step-by-Step Pathogenesis
Step 1 - Normal development (what should happen)
During embryogenesis, neural crest cells migrate from the proximal bowel downward (cecum → rectum), populating the bowel wall and forming two nerve networks:
- Meissner's submucosal plexus
- Auerbach's (myenteric) plexus
These plexuses coordinate peristalsis and allow the bowel to relax and propel contents forward.
Step 2 - The defect
In Hirschsprung's disease, this caudal migration is arrested prematurely OR the ganglion cells undergo premature apoptosis before reaching the distal segment. The result: the distal bowel (always including the rectum) has no ganglion cells - aganglionosis.
Step 3 - Consequence
Without ganglion cells:
- The aganglionic distal segment cannot relax - it stays in a state of tonic contraction
- Peristaltic waves cannot propagate through it
- This creates a functional obstruction
- Stool backs up, and the normally innervated colon proximal to the obstruction dilates progressively, forming the characteristic megacolon
Key point to remember: The narrow, normal-looking distal segment is the diseased one (aganglionic). The wide, dilated proximal segment is actually normal bowel that is secondarily distended from obstruction.
Molecular Basis (Genetics)
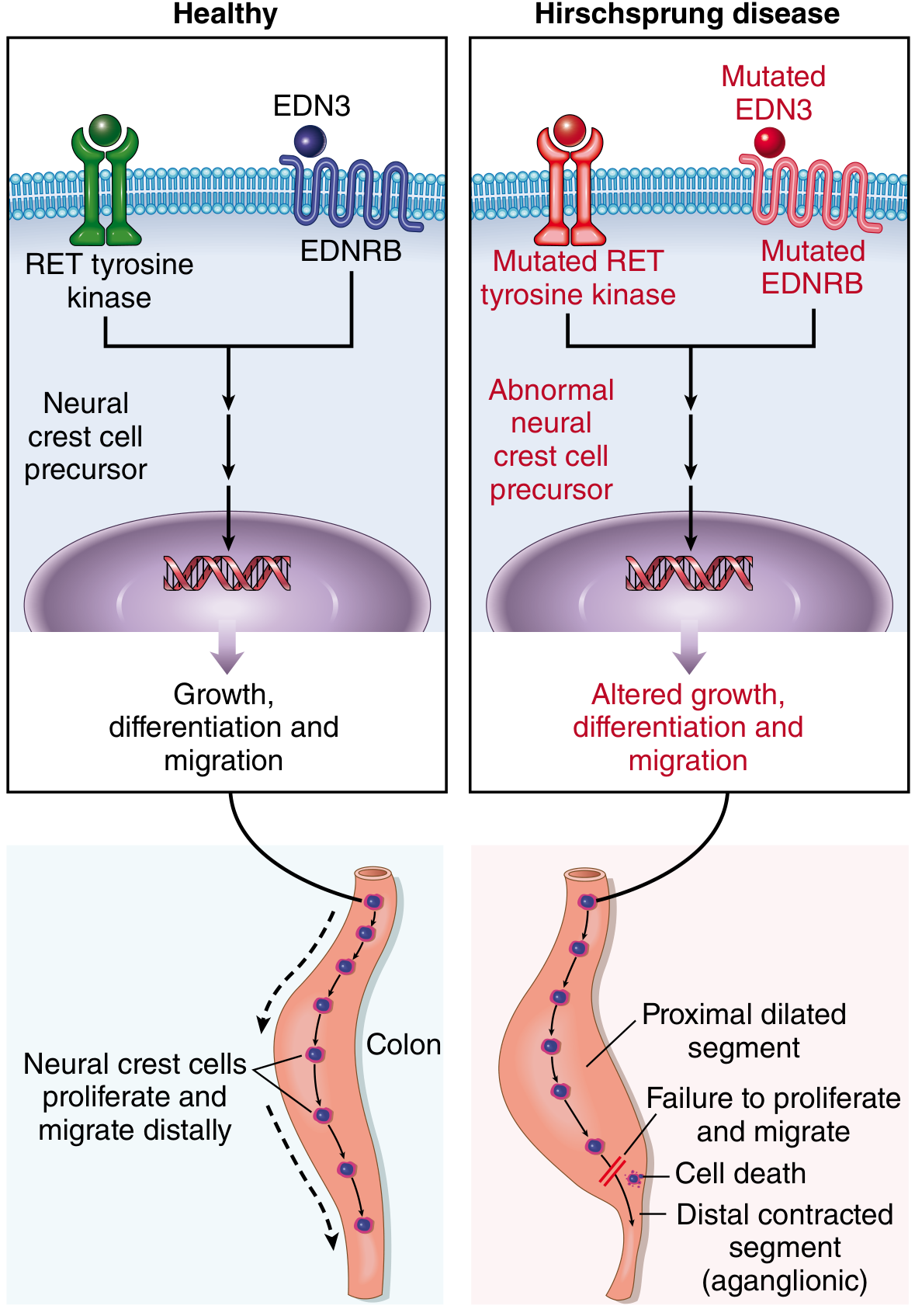
The diagram above shows the key molecular mechanisms:
| Gene/Protein | Normal Role | Disease Result When Mutated |
|---|---|---|
| RET receptor tyrosine kinase | Promotes neural crest cell proliferation, differentiation, and migration | Loss-of-function mutation: majority of familial cases, ~15% of sporadic cases |
| EDNRB (endothelin receptor B) | Regulates neural crest cell development | Germline mutation: impairs migration |
| EDN3 (endothelin-3 ligand for EDNRB) | Signals via EDNRB to guide migration | Mutation: same failure of migration |
When any of these signals are disrupted, neural crest cells fail to proliferate, differentiate, or migrate - leading to cell death and aganglionosis of the distal segment.
Gross Appearance
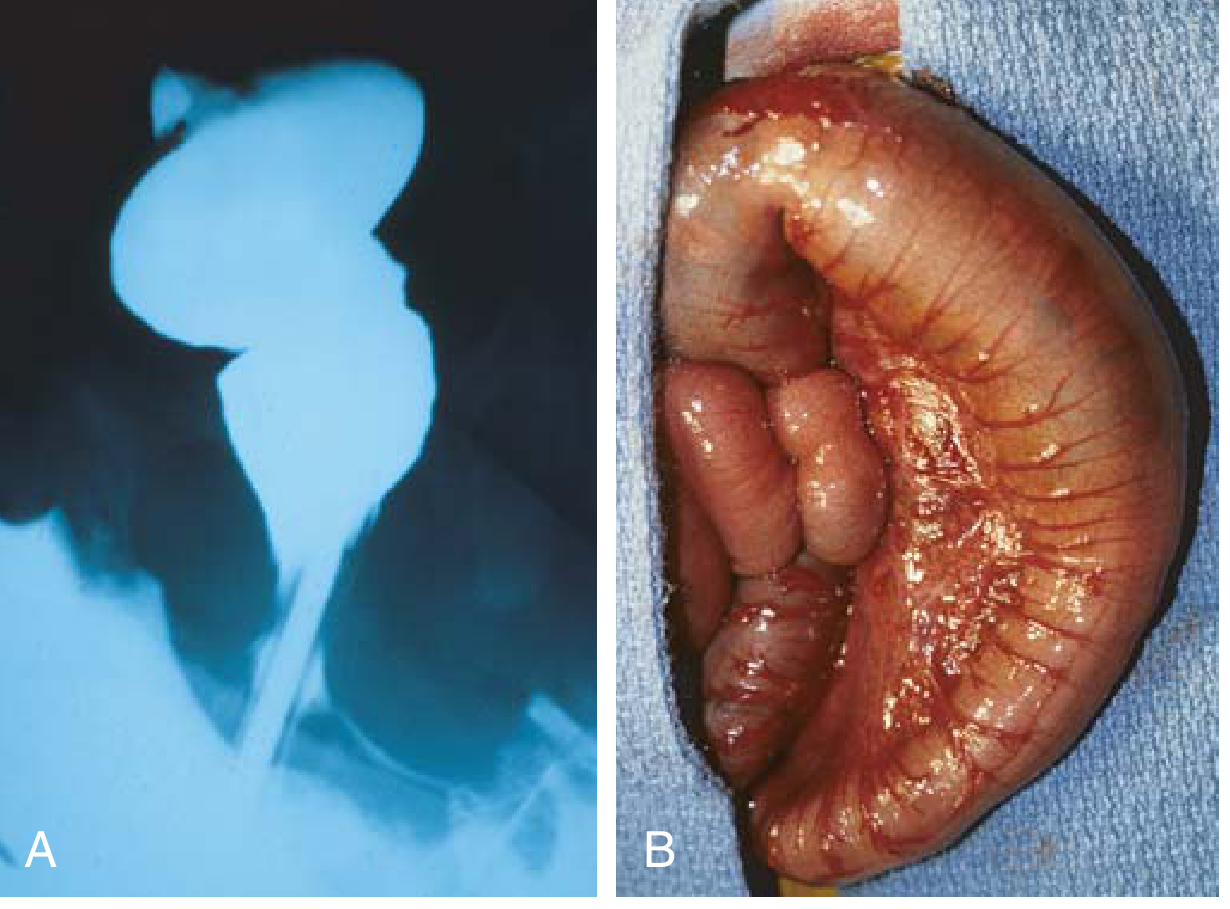
(A) Barium enema: narrow aganglionic rectum at the bottom, dilated sigmoid above - the classic "transition zone"
(B) Intraoperative appearance of the massively dilated proximal sigmoid colon
Summary in One Sentence
Neural crest cells fail to complete their caudal migration into the distal colon during fetal development → no ganglion cells → tonic contraction of the distal bowel → functional obstruction → proximal colon dilates.
Quick Facts
- Incidence: 1 in 5000 live births
- More common in males (4:1), but females tend to have more severe (longer segment) disease
- Rectum is always involved; extends to rectosigmoid in ~80% of cases
- 10% of cases occur in children with Down syndrome
- Leading cause of death in untreated cases: enterocolitis
- Gold standard diagnosis: rectal suction biopsy showing absent ganglion cells + hypertrophied nerve trunks
Sources: Robbins & Kumar Basic Pathology, p. 563; Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 703; Sabiston Textbook of Surgery
Mkcroacopic features
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
Reading File
Loading Image
Here are the complete microscopic features of Hirschsprung's disease:
Hirschsprung's Disease - Microscopic Features
The Gold Standard: Rectal Suction Biopsy
Diagnosis requires histologic confirmation - biopsy is taken 1-1.5 cm above the dentate line (to avoid the normal physiological hypoganglionic zone at the anal canal).
What You See on H&E (Hematoxylin & Eosin)
1. Absence of Ganglion Cells (CARDINAL FEATURE)
- No ganglion cells in both plexuses:
- Meissner's submucosal plexus
- Auerbach's myenteric plexus
- Normal bowel has large, round, vesicular ganglion cells with prominent nucleoli - these are completely absent in the aganglionic segment
2. Hypertrophied (Thickened) Nerve Trunks
- Large, prominent, non-myelinated nerve fibers are seen in:
- Lamina propria
- Muscularis mucosae
- Submucosa
- Myenteric (Auerbach's) intermuscular plexus
- This is the characteristic finding that replaces the normal ganglion cells
3. Both Adrenergic and Cholinergic Fibers Are Prominent
- Increased nerve fiber density is noted in the aganglionic segment across both fiber types
Histochemical / Immunohistochemical Stains
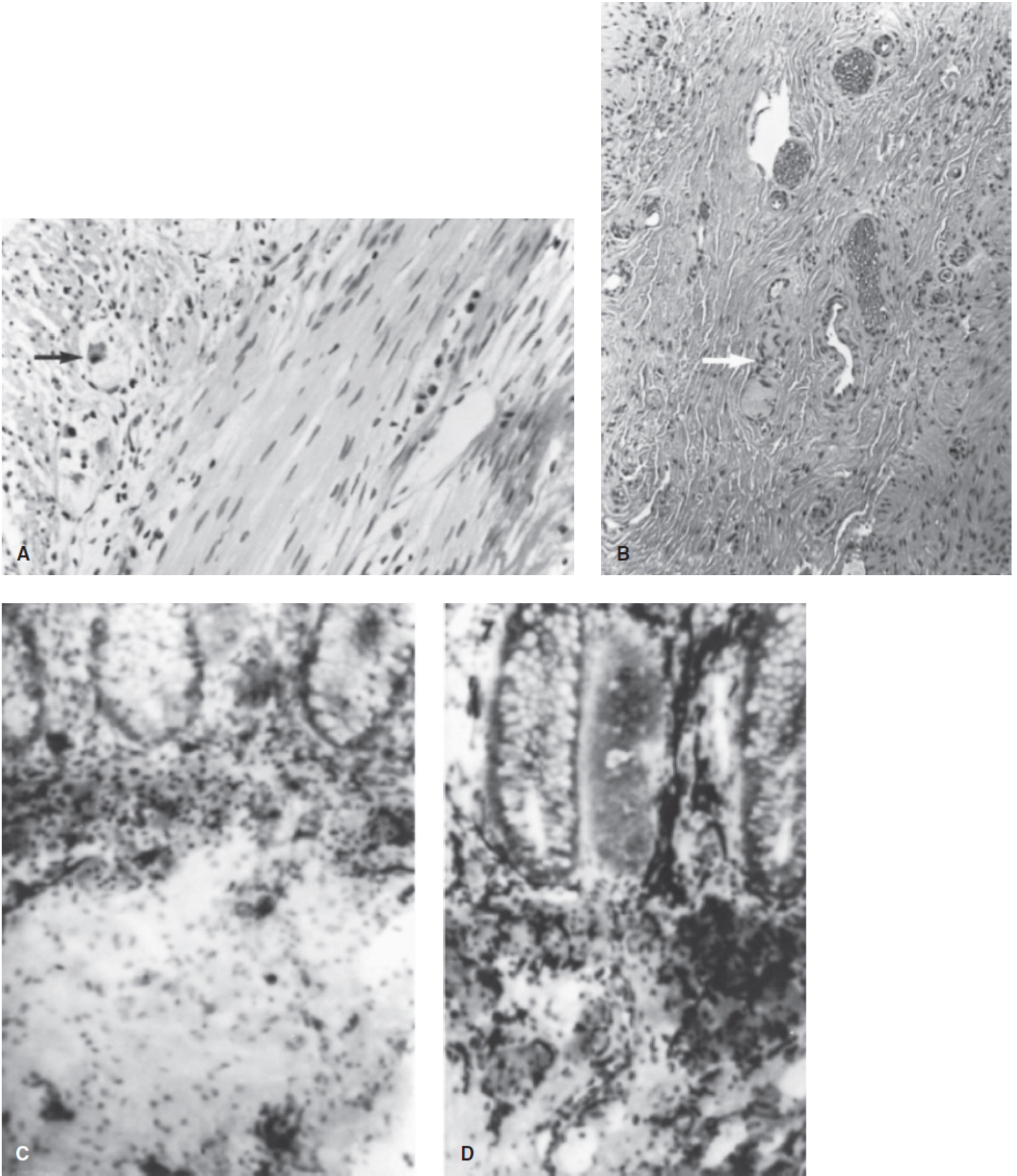
Figure: (A) Normal rectal biopsy - ganglion cell shown by arrow (H&E). (B) Aganglionic biopsy - note the characteristic thickened nerve fiber (arrow), no ganglion cells (H&E). (C) Normal acetylcholinesterase staining. (D) Hirschsprung's disease - many thickened submucosal nerve fibers stain densely black.
| Stain | Normal | Hirschsprung's |
|---|---|---|
| H&E | Ganglion cells visible in submucosa/myenteric plexus | Absent ganglion cells + hypertrophied nerve trunks |
| Acetylcholinesterase (AChE) | Fine, scattered nerve fibers in lamina propria | Densely staining, thickened nerve trunks stain dark black |
| Calretinin (IHC) | Positive in normal ganglion cells and small nerve fibers | Loss of calretinin-positive fibers in lamina propria |
| Nitric oxide synthase | Present in ganglion cells | Absent (important - NOS mediates smooth muscle relaxation) |
Summary Table of Microscopic Features
| Feature | Aganglionic Segment | Proximal (Normal) Segment |
|---|---|---|
| Ganglion cells | Absent | Present |
| Nerve trunks | Hypertrophied, thickened | Normal calibre |
| Peristalsis | Absent | Present |
| Calibre | Narrow (contracted) | Dilated (megacolon) |
| Muscularis | May be hypertrophied in proximal dilated segment | - |
Key Points to Remember
- The absence of ganglion cells combined with hypertrophied nerve trunks is the diagnostic pair
- AChE stain shows intensely staining thick nerve fibers in the aganglionic zone - a very reliable marker
- Calretinin immunostaining is now a standard adjunct - it marks ganglion cells and their thin nerve fibers; loss of calretinin in the lamina propria supports aganglionosis
- The biopsy must be taken at least 1-1.5 cm above the dentate line because the normal anal canal normally has reduced ganglion cells (physiologic hypoganglionosis), which would give a false positive if sampled
Sources: Mulholland & Greenfield's Surgery, p. 5533; Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 703; Sabiston Textbook of Surgery
Write full long qurstion answer for hurrshprungs fisease
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Here is the full comprehensive question-and-answer on Hirschsprung's disease:
Q. Write a detailed note on Hirschsprung's Disease (Congenital Aganglionic Megacolon)
DEFINITION
Hirschsprung's disease (HD) is a congenital disorder of colonic innervation characterized by the absence of ganglion cells (aganglionosis) in the myenteric (Auerbach's) and submucosal (Meissner's) plexuses of the distal bowel, resulting in a functional intestinal obstruction.
It is also called congenital aganglionic megacolon.
INCIDENCE & EPIDEMIOLOGY
| Feature | Detail |
|---|---|
| Incidence | 1 in 5000 live births |
| Sex | Males > Females (4:1); females tend to have longer segment disease |
| Association with Down syndrome | 10% of all HD cases; 3-5% of HD patients have Down syndrome |
| Familial risk | Increased if family history present; RET gene mutations in some families |
| Neurological abnormalities | Present in ~5% of affected infants |
EMBRYOLOGY & PATHOGENESIS
Normal Development
During embryogenesis, neural crest cells migrate craniocaudally into the bowel wall, ultimately forming the enteric nervous system - specifically:
- Meissner's submucosal plexus
- Auerbach's myenteric plexus
This migration is complete by the 12th week of gestation. The migration from the mid-transverse colon to the anus takes approximately 4 weeks - making this the most vulnerable window.
The Defect in Hirschsprung's Disease
Migration of neural crest cells is either:
- Arrested prematurely before reaching the distal bowel, OR
- Ganglion cell precursors undergo premature apoptosis (cell death)
The result: the distal bowel segment is completely devoid of ganglion cells (aganglionic).
Consequence
- The aganglionic distal segment cannot relax - it remains in tonic contraction
- Peristaltic waves cannot propagate through it
- A functional obstruction develops
- The normally innervated proximal bowel dilates progressively - forming the characteristic megacolon
Important: The narrow, normal-caliber distal segment is the diseased (aganglionic) bowel. The wide, dilated proximal segment is normal bowel distended from obstruction.
MOLECULAR / GENETIC BASIS
| Gene | Protein | Role | Mutation Effect |
|---|---|---|---|
| RET (chr 10) | RET receptor tyrosine kinase | Promotes neural crest cell proliferation, differentiation, migration | Loss-of-function = majority of familial cases, ~15% of sporadic cases |
| EDNRB | Endothelin receptor B | Regulates neural crest cell development | Mutation impairs migration |
| EDN3 | Endothelin-3 (ligand for EDNRB) | Guides neural crest cell migration | Mutation causes same failure |
| GDNF | Glial cell line-derived neurotrophic factor | Chemoattractant for neural crest cells | Mutation impairs migration |
| GFRA-1 | Co-receptor for GDNF/RET | Works alongside RET | Mutation causes aganglionosis |
EXTENT OF AGANGLIONOSIS
The rectum is always involved. Extension varies:
| Segment Involved | % of Cases | Type |
|---|---|---|
| Rectosigmoid colon | ~80% | Short-segment HD (most common) |
| Splenic flexure / Transverse colon | ~17% | Long-segment HD |
| Entire colon (+ small intestine) | ~8% | Total colonic aganglionosis |
The transition zone is the area between the dilated normal proximal bowel and the contracted aganglionic distal bowel - ganglion cells begin to appear here but in reduced numbers.
CLINICAL FEATURES
Neonatal Presentation (Most Common - >90%)
| Symptom | Details |
|---|---|
| Failure to pass meconium | Within first 24-48 hours of life - any infant not passing meconium by 48 hours must be investigated |
| Abdominal distention | Due to functional obstruction |
| Bilious vomiting | From backed-up intestinal contents |
| Forceful expulsion of foul-smelling liquid stool on rectal examination | From accumulated stool under pressure |
Presentation Beyond Neonatal Period (~20% of cases)
- Chronic constipation since birth
- Abdominal distention
- Failure to thrive
- Ribbon-like stools
- The diagnosis is sometimes missed if only a short rectal segment is involved
Hirschsprung-Associated Enterocolitis (HAEC)
This is the most feared and life-threatening complication, occurring in ~25% of cases either before or up to 20 months after surgical repair.
Features include:
- Abdominal distention and tenderness
- Alternating episodes of diarrhea and obstipation
- Fever
- Hematochezia
- Explosive, foul-smelling liquid stools on rectal exam
- Leukocytosis with increased band forms
- Peritonitis, shock, and death if untreated
- Enterocolitis is the leading cause of death in uncorrected Hirschsprung's disease
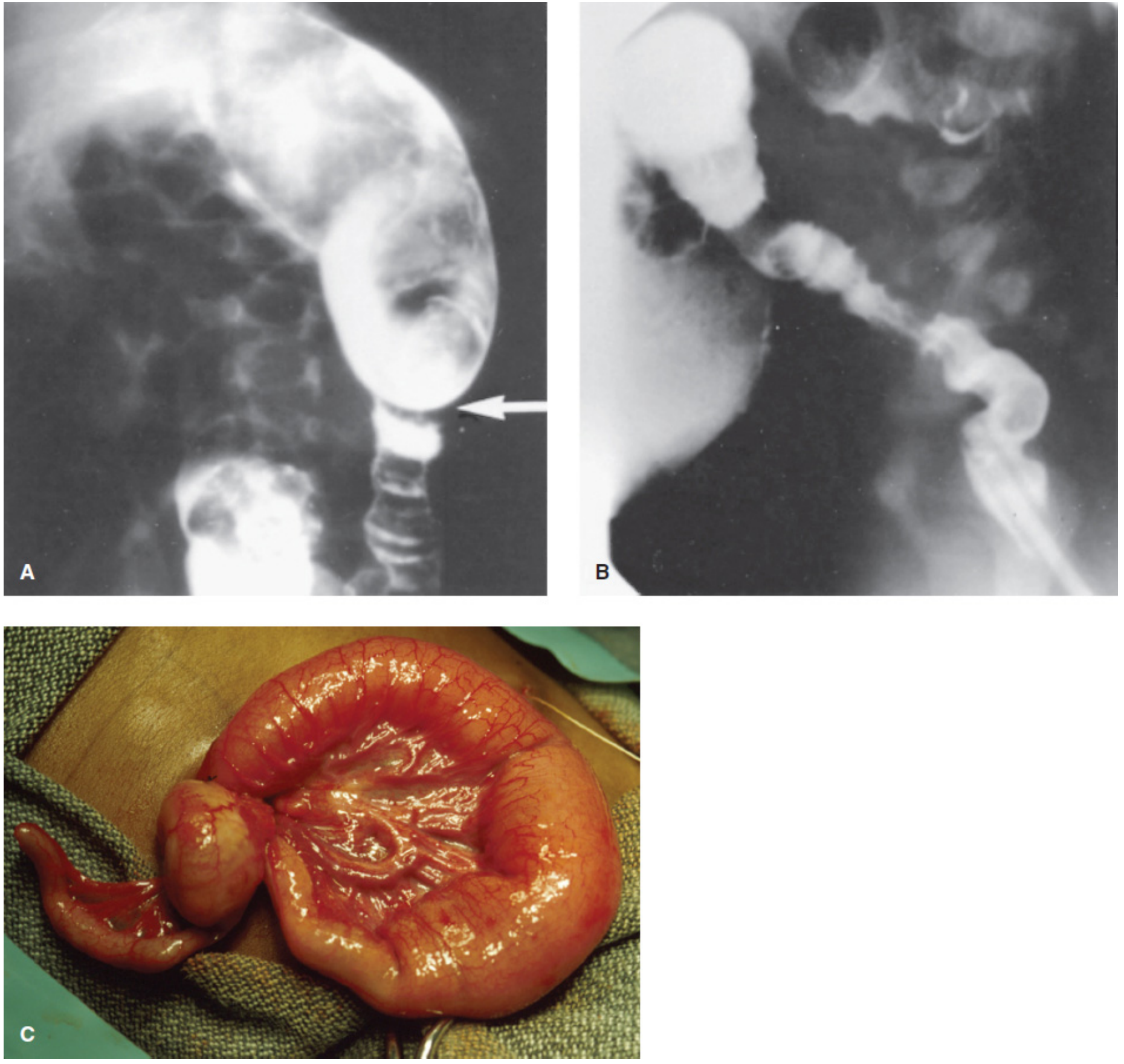
GROSS PATHOLOGY
- Distal aganglionic segment: Normal caliber or slightly contracted, externally looks near-normal
- Proximal ganglionic segment: Massively dilated (megacolon), hypertrophied walls
- Transition zone: Cone/funnel-shaped segment between the two; becomes evident on contrast enema in the first few weeks as obstruction progresses
MICROSCOPIC / HISTOLOGICAL FEATURES
On H&E Stain
- Absence of ganglion cells in both Meissner's and Auerbach's plexuses - the cardinal feature
- Hypertrophied (thickened), non-myelinated nerve trunks in:
- Lamina propria
- Muscularis mucosae
- Submucosa
- Myenteric plexus
- Both adrenergic and cholinergic nerve fibers are prominent and increased
Special Stains
| Stain | Hirschsprung's Finding |
|---|---|
| H&E | Absent ganglion cells + hypertrophied nerve trunks |
| Acetylcholinesterase (AChE) | Dense, dark black-staining thickened submucosal nerve trunks |
| Calretinin (IHC) | Loss of calretinin-positive nerve fibers in the lamina propria |
| Nitric oxide synthase | Absent (NOS normally mediates smooth muscle relaxation) |
Note: Biopsy must be taken 1-1.5 cm above the dentate line to avoid the physiologically hypoganglionic anal canal, which would give a false positive.
DIAGNOSIS
1. Rectal Suction Biopsy (Gold Standard)
- Performed at bedside in neonates without anesthesia (bowel lacks somatic innervation)
- Samples taken at 1 cm, 2 cm, and 3 cm from dentate line
- Full-thickness biopsy required in older children (under general anesthesia)
- Histopathology confirms absent ganglia + hypertrophied nerve trunks + positive AChE staining
2. Contrast Enema (Barium Enema)
- Shows the transition zone - narrow distal aganglionic segment with dilated proximal colon
- Failure to evacuate contrast after 24 hours strongly suggests HD
- Also useful to exclude: meconium plug syndrome, colonic atresia, small left colon syndrome
3. Anorectal Manometry
- Tests the rectoanal inhibitory reflex (RAIR)
- In HD: failure of internal sphincter to relax on rectal balloon distension (paradoxical increase in tone)
- Useful in older children; 85-90% accurate when performed carefully
- Not widely used in USA for primary diagnosis in infancy
4. Plain Abdominal X-Ray
- Non-specific: dilated air-filled loops of bowel consistent with distal intestinal obstruction
- In enterocolitis: thickened loops + pneumatosis intestinalis
DIFFERENTIAL DIAGNOSIS
| Condition | Distinguishing Feature |
|---|---|
| Functional constipation | No structural/neurologic defect; responds to laxatives; normal biopsy |
| Meconium plug syndrome | Resolves with contrast enema; no aganglionosis |
| Small left colon syndrome | Associated with infants of diabetic mothers; resolves spontaneously |
| Colonic atresia | Distinct on imaging; structural discontinuity |
| Hypothyroidism | Acquired megacolon; thyroid function tests abnormal |
| Chagas disease | Acquired megacolon due to Trypanosoma cruzi; destroys ganglion cells |
TREATMENT
Surgery is required in all cases.
Pre-operative Management
- Rectal irrigations (warm saline via soft catheter) daily - decompresses the bowel
- Antibiotics and IV fluids if enterocolitis present
- Leveling colostomy if: enterocolitis not responding, long-segment disease, or poor family compliance - placed in confirmed ganglionated bowel using frozen section biopsies
Definitive Surgery: Pull-Through Procedures
The principle of all procedures is the same:
- Confirm the level of ganglion cells (transition zone) using intraoperative frozen sections
- Resect the aganglionic segment
- Anastomose ganglionated bowel to anus/rectal cuff
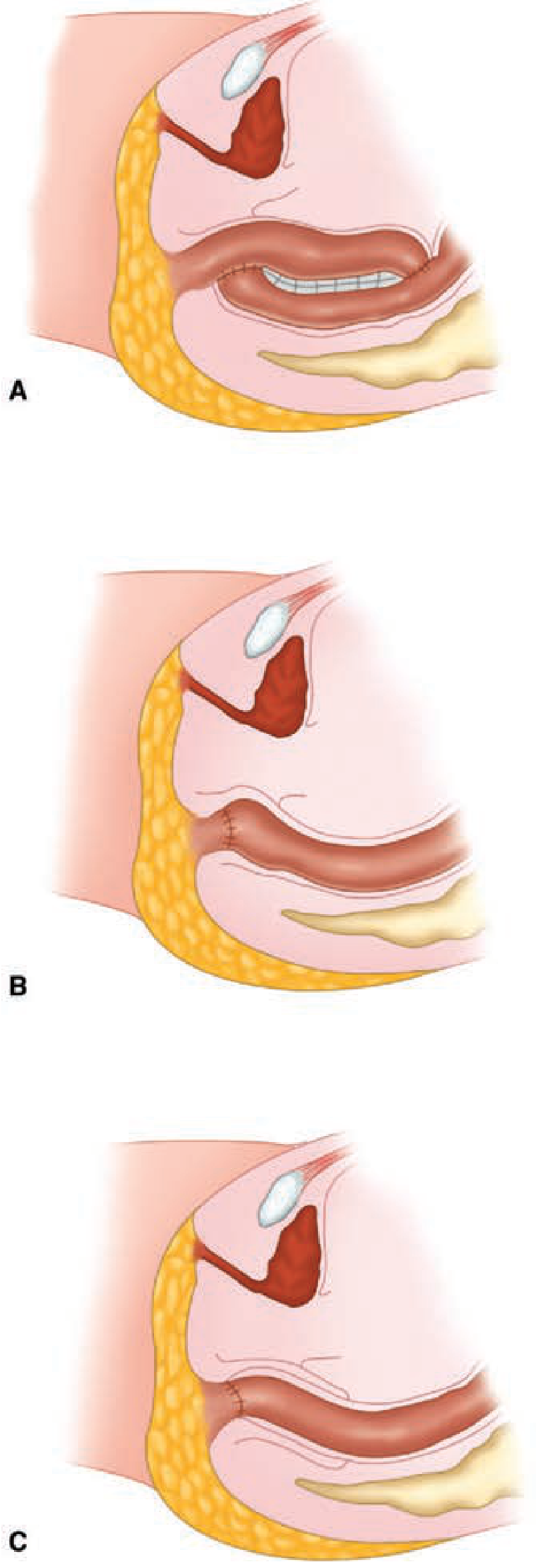
| Procedure | Technique | Notes |
|---|---|---|
| Swenson (original, 1949) | Full-thickness pelvic dissection; aganglionic rectum removed; end-to-end coloanal anastomosis via perineal approach | Risk of parasympathetic nerve injury |
| Duhamel | Retrorectal dissection; ganglionic colon pulled behind aganglionic rectal cuff; side-to-side stapled anastomosis forming a neorectum | Leaves anterior aganglionic rectal wall |
| Soave (most commonly used today) | Endorectal mucosal stripping within aganglionic rectum; ganglionic colon pulled through muscular sleeve; coloanal anastomosis | Can be done entirely transanally; lower parasympathetic nerve injury risk |
All three procedures can be performed laparoscopically - now the current standard of care for most infants.
Primary (single-stage) pull-through is now preferred for most patients - avoids the morbidity of a colostomy.
COMPLICATIONS
Post-operative Complications
| Complication | Notes |
|---|---|
| Post-operative enterocolitis | Most common serious complication; occurs in ~25% before and after surgery |
| Constipation | Persistent in many patients; managed with stool softeners and laxatives |
| Anastomotic stricture | Requires dilation |
| Soiling / Fecal incontinence | May take years to resolve |
| Recurrent HD | Due to residual aganglionic bowel or transition zone pull-through; ~1/3 of transition zone pull-throughs require reoperation |
| Urinary dysfunction | If parasympathetic nerves damaged (especially with Swenson) |
PROGNOSIS
- Long-term results are generally excellent in experienced hands
- All three pull-through procedures have comparable outcomes
- Normal bowel function and continence may take years to develop
- Close postoperative follow-up is mandatory
- If symptoms persist, histologic re-evaluation at anastomosis site is required
- Patients with total colonic aganglionosis have a more challenging course
SUMMARY BOX
| Feature | Key Point |
|---|---|
| Cause | Failed caudal migration of neural crest cells during embryogenesis |
| Defect | Absence of ganglion cells in Meissner's + Auerbach's plexus |
| Result | Tonic contraction of distal bowel → functional obstruction → proximal megacolon |
| Most common segment | Rectosigmoid (80%) |
| Sex | Male > Female (4:1) |
| Key association | Down syndrome (trisomy 21) |
| Key gene | RET (chromosome 10) |
| Hallmark symptom | Failure to pass meconium within 48 hours |
| Leading cause of death | Hirschsprung-associated enterocolitis |
| Gold standard diagnosis | Rectal suction biopsy (absent ganglion cells + hypertrophied nerve trunks) |
| Confirmatory stain | Acetylcholinesterase (AChE) - dense black trunks; Calretinin loss |
| Treatment | Pull-through surgery (Swenson / Duhamel / Soave) |
| Best imaging | Contrast (barium) enema - shows transition zone |
Sources: Robbins & Kumar Basic Pathology; Robbins, Cotran & Kumar Pathologic Basis of Disease; Schwartz's Principles of Surgery 11e; Sabiston Textbook of Surgery; Mulholland & Greenfield's Surgery 7e
This is a shared conversation. Sign in to Orris to start your own chat.