RA management
Reading File
Finding Sources
Searching PubMed
"rheumatoid arthritis"[MeSH Terms] AND "management"[MeSH Terms]
Finding Sources
Searching PubMed
"rheumatoid arthritis" AND treatment
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the content needed for a comprehensive RA management answer.
Rheumatoid Arthritis (RA) — Management
Principles of Treatment
RA has no known cure; the overriding goals are remission (achievable in >50% of patients treated early) or low disease activity in all patients. Key principles:
| Key | Detail |
|---|---|
| Early diagnosis + early DMARD | Erosions begin in the first 1–2 years — irreversible once established |
| Treat-to-target (T2T) | Reassess every 1–3 months; escalate until target is met |
| Multidisciplinary | Rheumatologist, nurse specialist, physio, OT, orthopedic surgeon |
| Comorbidities | CVD, infection risk, osteoporosis must be actively managed |
— Goldman-Cecil Medicine, p. 2794
Three Drug Categories
1. NSAIDs
- Provide symptomatic relief only — do not alter disease course
- Never use as sole therapy — always pair with a DMARD
- Prefer naproxen/ibuprofen over COX-2 inhibitors given CV risk in RA; if COX-2 used, keep at lowest dose
- Add PPI for all RA patients on NSAIDs
- Doses: Celecoxib 100 mg BD | Naproxen 500 mg BD | Ibuprofen 400 mg QID
2. Glucocorticoids
- Rapid onset — used as bridge while DMARDs take effect
- Prednisone ≤10 mg/day; taper to lowest effective dose
- Shown to reduce erosive damage and disability when added at start of MTX-based therapy
- Can use intra-articular or IM depot for flares
- Goal: wean off, or very low dose, once DMARDs are effective
- Risk: 25% ↑ serious infection even at 5 mg/day; doubling at 5–10 mg/day
3. DMARDs (cornerstone of therapy)
Conventional (csDMARDs)
| Drug | Dose | Notes |
|---|---|---|
| Methotrexate | 7.5–25 mg PO/SQ once weekly | First-line anchor drug |
| Hydroxychloroquine | 200–400 mg daily (5 mg/kg) | Mild disease; retinal monitoring |
| Leflunomide | 10–20 mg daily | Alternative to MTX |
| Sulfasalazine | 500 mg BD → 2 g/day | Often used in combination |
| Azathioprine | 1–2.5 mg/kg/day | Steroid-sparing |
| Minocycline | 100 mg BD | Mild, seropositive disease |
Triple therapy (MTX + hydroxychloroquine + sulfasalazine) has efficacy comparable to MTX + biologic in some trials.
Biologic DMARDs (bDMARDs)
| Class | Agents | Route |
|---|---|---|
| TNF inhibitors | Etanercept, Infliximab, Adalimumab, Certolizumab, Golimumab | SC / IV |
| IL-6 inhibitors | Tocilizumab, Sarilumab | SC / IV |
| T-cell costimulation blocker | Abatacept (500–1000 mg IV q4wk) | IV / SC |
| B-cell depletion | Rituximab (1000 mg IV × 2, 2 wks apart) | IV |
| IL-1 inhibitor | Anakinra | SC daily |
Note: Tocilizumab and JAK inhibitors raise serum cholesterol; TNF inhibitors and MTX reduce cardiovascular mortality.
Targeted Synthetic DMARDs (tsDMARDs) — JAK Inhibitors
| Drug | Dose |
|---|---|
| Tofacitinib | 5 mg PO BD or 11 mg XR daily |
| Baricitinib | 2 mg PO daily |
| Upadacitinib | 15 mg PO daily |
JAK inhibitors carry FDA black-box warnings for thrombosis, serious infections, and malignancy risk (particularly in patients >65, smokers, or with CVD). Use after failure of at least one csDMARD.
Treatment Algorithm (ACR Guidelines)
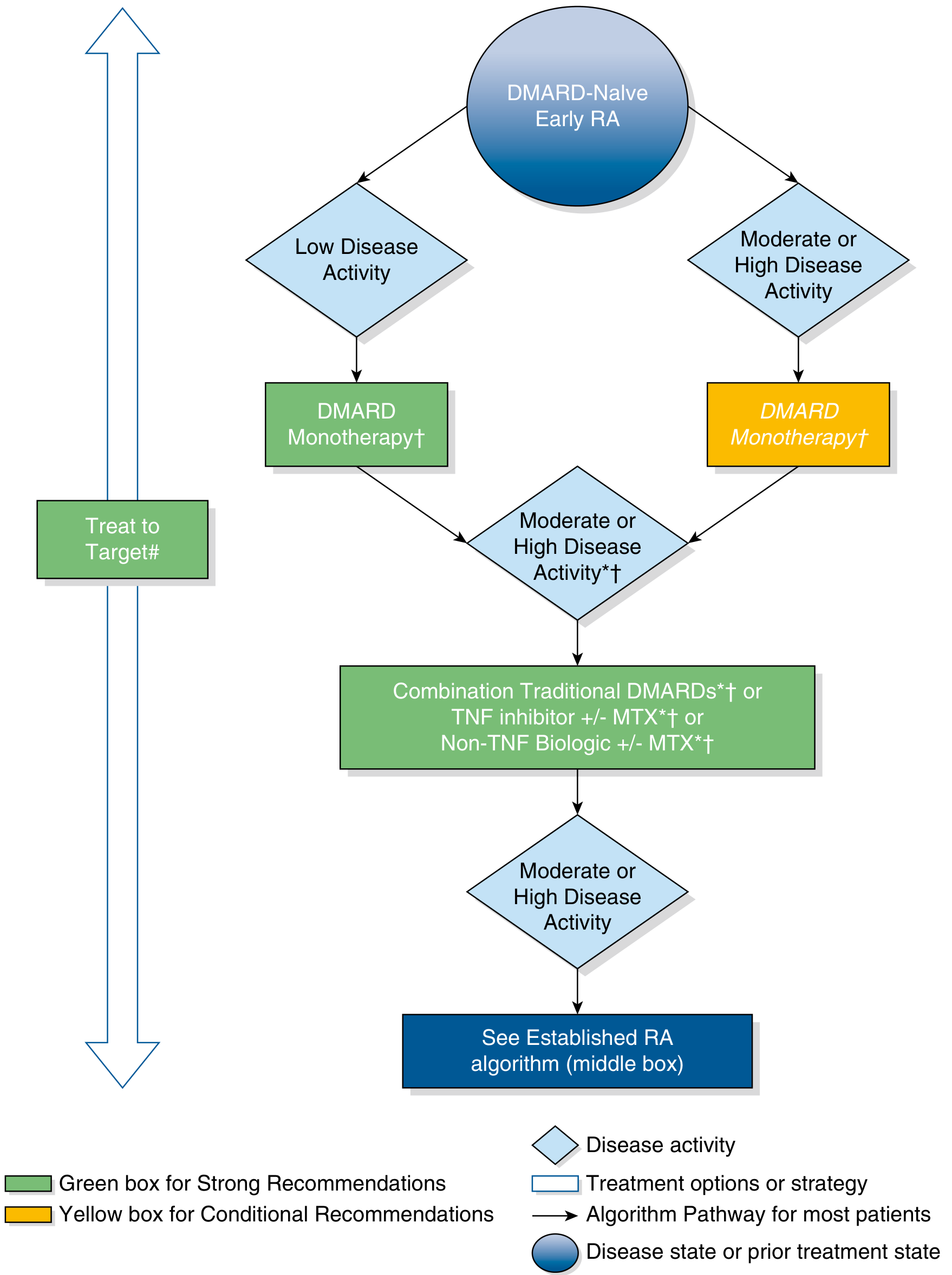
Early RA (DMARD-naïve):
- Low disease activity → DMARD monotherapy (MTX preferred)
- Moderate/high disease activity → DMARD monotherapy (conditional) → if still moderate/high → Combination csDMARDs or TNF inhibitor ± MTX or non-TNF biologic ± MTX
Established RA (inadequate response):
- Escalate to combination DMARDs, add biologic, or switch biologic class
- If TNF inhibitor fails → try non-TNF biologic (e.g., abatacept, tocilizumab, rituximab) or JAK inhibitor
— Swanson's Family Medicine Review, Fig. 49.2
Monitoring & Safety
| Drug | Key Monitoring |
|---|---|
| MTX | LFTs, CBC, renal function; folic acid 1 mg/day to reduce toxicity |
| Hydroxychloroquine | Annual ophthalmology (retinal toxicity) |
| Leflunomide | LFTs, blood pressure |
| Biologics/JAK inhibitors | TB screening (LTBI), hepatitis B serology before starting; annual influenza vaccine; pneumococcal vaccine; avoid live vaccines |
| Glucocorticoids | Bone density (DEXA); calcium + vitamin D; BP; glucose |
Comorbidity Management
- Cardiovascular: Aggressive risk factor treatment; MTX + TNF inhibitors reduce CV mortality
- Osteoporosis: Screen all RA patients; treat early
- Infections: Heightened risk (disease + therapy); vaccinate (pneumococcal, influenza, zoster); prompt treatment of infections
- Lymphoma: Increased risk — monitor; some B-cell lymphomas regress on reducing immunosuppression
- Cervical spine: C1–C2 instability in 30–40% of established RA; 5% develop myelopathy — screen before procedures
Surgical Management
- Considered when medical therapy fails to control joint damage
- Procedures: synovectomy, tendon repair, joint replacement (hip/knee most common)
- Pre-op cervical spine X-ray mandatory (atlanto-axial instability)
Prognosis
- RF+, anti-CCP+, and shared epitope (HLA-DRB1) → worse prognosis (more erosions, extra-articular disease)
- With modern aggressive DMARD/biologic therapy, all-cause mortality now approaches that of the general population
— Goldman-Cecil Medicine, p. 2795
Recent evidence note: A 2024 systematic review/meta-analysis supporting JAK inhibitors in RA-associated ILD (PMID: 39270812) and the 2024 Japan College of Rheumatology updated guidelines (PMID: 38814660) are available for reference. CAR-T cell therapy is under early investigation for refractory autoimmune disease (PMID: 39754644).
This is a shared conversation. Sign in to Orris to start your own chat.