Biomechanics of shoulder - 15 marks MPT level answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Loading Image
Loading Image
I now have comprehensive, authoritative content from three major textbooks. Let me compose the full MPT-level answer.
BIOMECHANICS OF THE SHOULDER
MPT-Level Answer (15 Marks)
I. INTRODUCTION
The shoulder complex is the most mobile joint in the human body, achieving this range of motion through the coordinated interaction of four distinct articulations: the sternoclavicular (SC), acromioclavicular (AC), glenohumeral (GH), and scapulothoracic (ST) joints. The fundamental biomechanical challenge is balancing extraordinary mobility with adequate stability - achieved through a carefully orchestrated interplay of bony geometry, labrum, capsule-ligament complex, and musculotendinous structures.
- Campbell's Operative Orthopaedics 15th Ed 2026
- Miller's Review of Orthopaedics 9th Edition
II. STRUCTURAL FOUNDATIONS: BONY GEOMETRY
The glenohumeral joint is characterized by a disproportionate bony architecture - classically described as a "golf ball on a tee" or "ball on a seal's nose." The humeral head surface area is significantly larger than the glenoid, providing minimal inherent bony constraint.
Key bony parameters:
- Humeral head inclination: ~125 degrees
- Humeral head retroversion: ~25 degrees
- Glenoid retroversion: slight posterior tilt (provides posterior stability)
- Native glenoid depth: ~9 mm superoinferior, ~5 mm anteroposterior
- The glenoid labrum increases socket depth by 50%, augmenting contact surface to 75% of the humeral head vertically and 57% horizontally
The "large ball - small socket" configuration maximizes arc of motion but requires the surrounding soft tissues to compensate for the reduced bony constraint.
- Campbell's Operative Orthopaedics 15th Ed 2026
- Miller's Review of Orthopaedics 9th Edition
III. KINEMATICS
A. Scapular Plane
The scapula lies 30 degrees anterior to the coronal plane. This is the preferred reference plane for all shoulder ROM measurement because:
- The glenohumeral ligaments are lax in this plane
- Minimal impingement of supraspinatus against the acromion
- Abduction in this plane requires less external rotation to clear the greater tuberosity
B. Scapulohumeral Rhythm (2:1 Ratio)
Full shoulder abduction to 180° involves:
| Component | Contribution |
|---|---|
| Glenohumeral motion | 120 degrees |
| Scapulothoracic motion | 60 degrees |
| Ratio | 2:1 (GH:ST) |
This 2:1 ratio is not fixed throughout the arc - it varies significantly in the first 30 degrees of elevation. During early abduction (0-30°), most motion occurs at the GH joint as the scapula "sets." Beyond 30°, scapular upward rotation becomes increasingly prominent.
Clinical importance: Disturbance of normal scapulohumeral rhythm - termed dyskinesia - shifts biomechanical load, narrows the subacromial space, and predisposes to secondary impingement.
- Rheumatology 2-Volume Set, Elsevier 2022
C. Surface Joint Motion at the GH Joint
GH joint surface motion is a combination of rotation, rolling, and translation rather than pure rolling or sliding. The femoral head analogy does not apply here - the humeral head undergoes:
- Rolling (translating center of rotation)
- Sliding/gliding (compensatory counter-translation)
- Spinning (axial rotation)
This complex triplanar kinematics is why even small labral or capsular defects can substantially alter joint mechanics.
D. Zero Position
- Defined as 165 degrees of abduction in the scapular plane
- Minimal deforming forces about the shoulder at this position
- Ideal position for reducing shoulder dislocations and fractures with traction
E. Abduction - External Rotation Requirement
During arm elevation in the coronal plane, the humerus must externally rotate to allow the greater tuberosity to clear beneath the coracoacromial arch. With internal rotation contractures, abduction is limited to approximately 120 degrees because the greater tuberosity impinges on the acromion.
IV. STATIC STABILIZERS
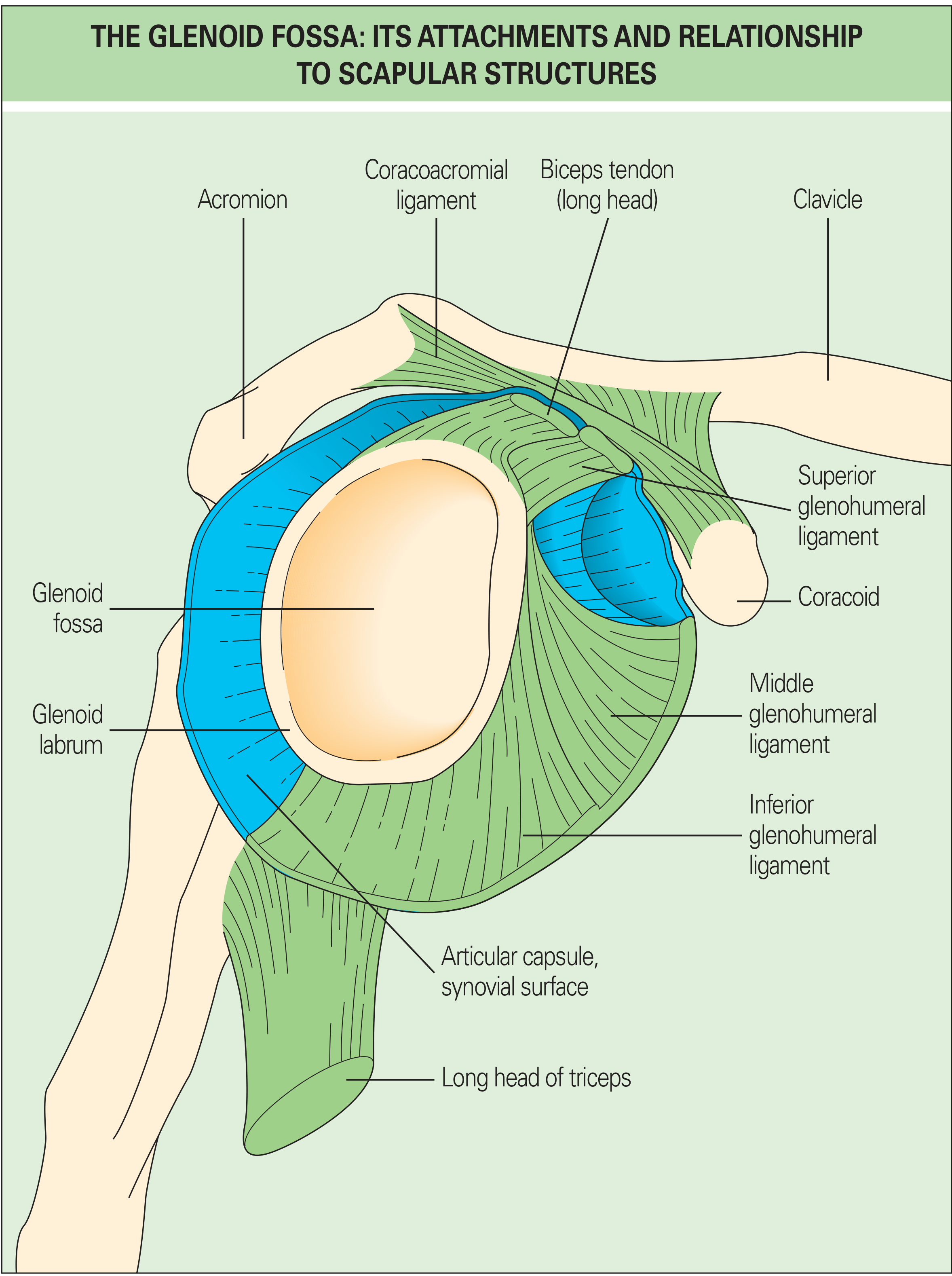
A. Glenoid Labrum
- Fibrocartilaginous ring encircling the glenoid
- Increases bony socket depth by 50%
- Distributes compressive contact stresses, particularly at 90° abduction
- Superior labrum serves as biceps anchor (SLAP region)
B. Glenohumeral Capsule and Ligaments
The glenohumeral ligaments (SGHL, MGHL, IGHL) are thickenings within the anterior capsule. Their function is position-dependent:
| Ligament | Primary Role | Position of Maximum Tension |
|---|---|---|
| SGHL | Inferior subluxation prevention; anterior-posterior restraint | 0° abduction (arm at side) |
| MGHL | Limits external rotation | Mid-range abduction (45-60°) |
| IGHL (anterior band) | Main stabilizer to anterior & posterior stress | ≥45° abduction - most important overall |
| IGHL (posterior band) | Posterior restraint in abduction + ER | Arm abducted and internally rotated |
The IGHL forms a "hammock-type sling" with an anterior band, posterior band, and axillary pouch:
- With external rotation - hammock slides anteriorly, anterior band tightens, posterior band fans out
- With internal rotation - the opposite occurs
Rotator interval (triangular area between supraspinatus and subscapularis): tightening this interval reduces both posterior and inferior translation. Contains the SGHL and coracohumeral ligament.
C. Negative Intraarticular Pressure
Inferior subluxation in the neutral position is resisted in part by negative intraarticular pressure (suction effect), which acts as a passive stabilizer when the ligaments are lax.
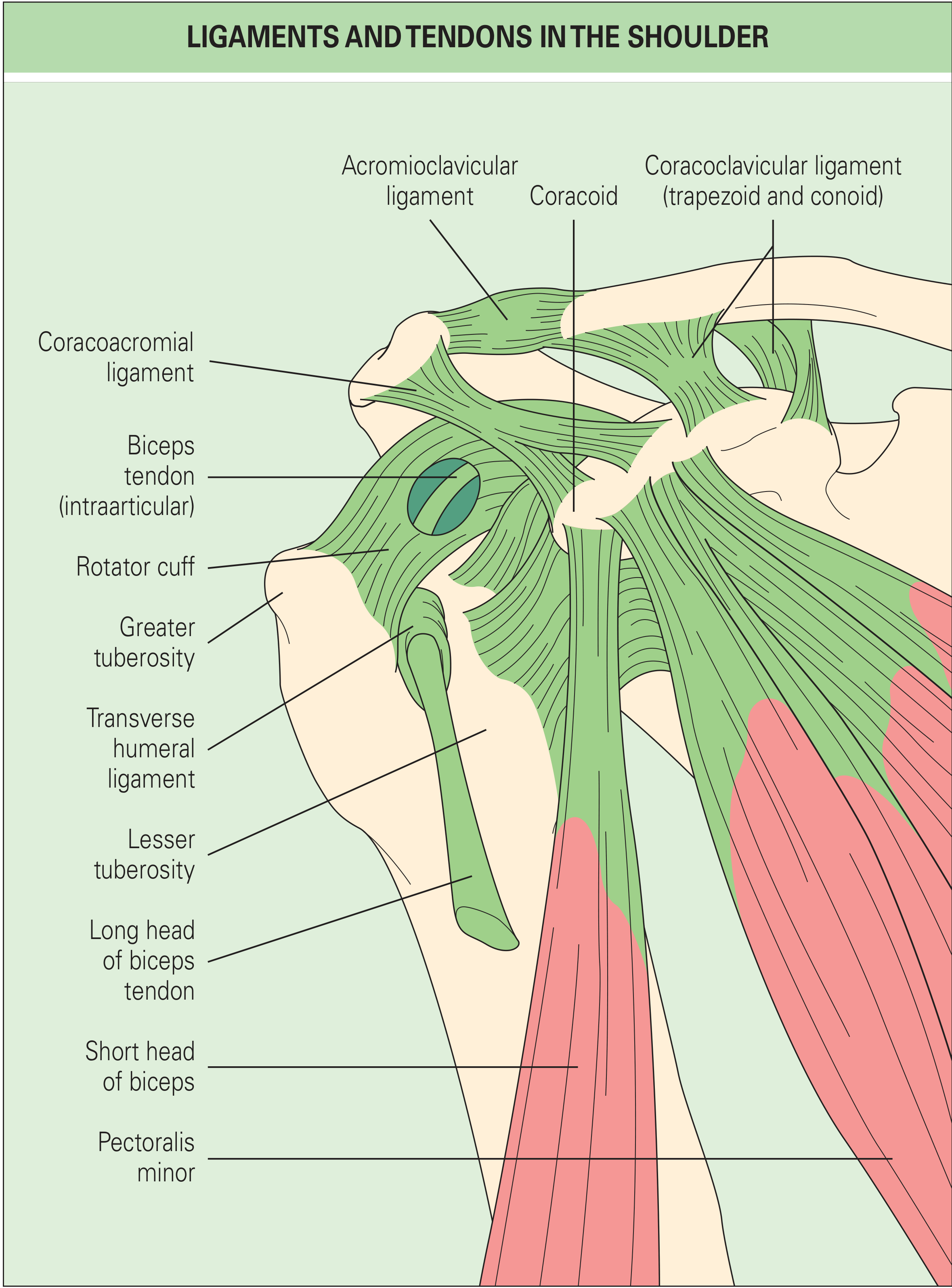
D. Acromioclavicular and Coracoclavicular Ligaments
-
AC ligament - maintains horizontal stability of AC joint
-
Coracoclavicular ligament (trapezoid + conoid) - transmits vertical loads; scapular rotation occurs through this ligament
-
Coracoacromial ligament - forms the roof of subacromial space; prevents superior escape of the humeral head
-
Campbell's Operative Orthopaedics 15th Ed 2026
-
Miller's Review of Orthopaedics 9th Edition
V. DYNAMIC STABILIZERS
A. Rotator Cuff - The Central Dynamic Stabilizer
The rotator cuff (subscapularis, supraspinatus, infraspinatus, teres minor) contributes to stability through three mechanisms:
1. Compression: Rotator cuff muscles generate a compressive force vector that centers the humeral head in the glenoid ("concavity compression mechanism"). This is why patients with massive superior cuff tears can paradoxically retain some overhead function if the subscapularis and posterior cuff remain intact.
2. Barrier effect: The physical bulk of the cuff tendons provides a restraint against translation.
3. Capsular stiffening: Rotator cuff contraction increases the stiffness and torsional rigidity of the glenohumeral capsule, reducing translation. Biceps tendon activity similarly stiffens the capsule.
B. Rotator Cuff Force Couples
The most important biomechanical concept of rotator cuff function is the force couple:
Coronal plane force couple (abduction):
- Deltoid generates a superiorly directed shear force
- Rotator cuff (primarily supraspinatus, infraspinatus, teres minor, subscapularis) generates an inferiorly directed compressive/depressive force
- Together they create net abduction torque while keeping the humeral head centered in the glenoid
Transverse plane force couple (rotation):
- Subscapularis (anterior) vs infraspinatus + teres minor (posterior)
- These muscles work in opposition to provide rotational control and maintain centration
- This is why isolated massive posterior cuff tears create anterosuperior escape and why subscapularis integrity is critical for glenohumeral stability
C. Muscle Action Table (Kinetics)
| Motion | Primary Muscles |
|---|---|
| GH Abduction | Deltoid + supraspinatus (cuff depresses head) |
| GH Adduction | Latissimus dorsi, pectoralis major, teres major |
| Forward Flexion | Pectoralis major, anterior deltoid, biceps |
| Extension | Latissimus dorsi |
| Internal Rotation | Subscapularis, teres major |
| External Rotation | Infraspinatus, teres minor, posterior deltoid |
| Scapular Upward Rotation | Upper trapezius + lower trapezius + serratus anterior (force couple) |
| Scapular Adduction | Trapezius, rhomboids, latissimus dorsi |
| Scapular Abduction | Serratus anterior, pectoralis minor |
- Miller's Review of Orthopaedics 9th Edition (Table 1.44)
D. Periscapular Muscles and Scapular Stabilizers
The extrinsic muscles (rhomboids, levator scapulae, trapezius, serratus anterior) dynamically position the scapula to place the glenoid "opposite the humeral head" as the shoulder moves. This scapular repositioning is a prerequisite for normal GH mechanics. Loss of serratus anterior function (long thoracic nerve palsy) causes winging and profoundly disrupts this repositioning, leading to secondary GH impingement.
Scapular upward rotation force couple:
- Upper trapezius (superior force on clavicle/scapula) + lower trapezius (inferior force on scapular spine) + serratus anterior (inferior angle traction) = pure upward rotation torque with minimal translational component.
E. Biceps Tendon
The long head of the biceps (LHB) acts as a humeral head depressor and anterior stabilizer. Mechanically, it stiffens the capsule and reduces superior translation, particularly in abduction and external rotation. Its intraarticular course through the rotator interval explains why LHB pathology is frequently associated with subscapularis tears.
VI. ROTATOR CABLE AND CRESCENT
A clinically important concept: the rotator cuff is not mechanically homogeneous. The rotator cable is a thick bundle of fibers running perpendicular to the direction of the cuff tendons, acting as a suspensory arch that transfers loads around the rotator crescent (the thinner, avascular zone near insertion). This explains why small crescent tears may be relatively well tolerated, while cable tears correlate more directly with pain and weakness.
- Campbell's Operative Orthopaedics 15th Ed 2026
VII. KINETICS: JOINT REACTION FORCES
- During abduction, the GH joint reaction force is directed inferiorly and medially into the glenoid fossa
- Peak GH joint reaction forces during activities of daily living can reach 0.89 × body weight during abduction
- The subacromial space is narrowed by superior deltoid shear forces; the intact rotator cuff must generate sufficient inferior compressive force to maintain joint centration and prevent impingement
- With rotator cuff deficiency, superior humeral head migration occurs, eventually leading to cuff tear arthropathy
VIII. STERNOCLAVICULAR AND ACROMIOCLAVICULAR JOINT MECHANICS
Sternoclavicular joint:
- Diarthrodial saddle joint with intra-articular disk
- Allows clavicular: elevation/depression (frontal plane), protraction/retraction (transverse plane), and axial rotation (long axis)
- Axillary motion in the scapulothoracic joint is partly achieved through SC joint rotation
- Strong posterior ligaments = primary AP stabilizer; costoclavicular ligament = secondary
Acromioclavicular joint:
- Scapular rotation is transmitted through the conoid and trapezoid ligaments
- AC joint movement occurs during the early part of overhead elevation
- Disruption (AC separation) directly alters scapulothoracic rhythm and subacromial mechanics
IX. SUBACROMIAL SPACE BIOMECHANICS
The coracoacromial arch (acromion + coracoacromial ligament + coracoid) forms a rigid roof over the subacromial space, which normally contains the supraspinatus tendon and subacromial bursa. Key factors affecting this space:
- Acromial morphology (Type I flat, Type II curved, Type III hooked - Bigliani classification)
- Humeral head position (superior migration in cuff deficiency)
- Scapular tilt and rotation
- Arm elevation plane and rotation
During full elevation, the subacromial space reaches its minimum, making dynamic narrowing the basis of outlet impingement (Neer's concept).
X. CLINICAL APPLICATIONS
| Biomechanical Concept | Clinical Relevance |
|---|---|
| 2:1 scapulohumeral rhythm | Scapular dyskinesia screening; shoulder impingement |
| Force couple disruption | Rotator cuff tear patterns; reverse shoulder arthroplasty design |
| IGHL hammock mechanism | Bankart lesion; shoulder dislocation repair |
| Negative intraarticular pressure | Sulcus sign; multidirectional instability |
| Rotator cuff concavity compression | Rationale for cuff strengthening in instability rehab |
| Scapulothoracic rhythm disruption | Secondary impingement; periscapular strengthening protocols |
| Zero position | Traction reduction technique; post-op positioning |
| Rotator cable biomechanics | Partial vs full cuff tear prognosis; surgical repair strategy |
SUMMARY
The shoulder achieves its unparalleled range of motion through:
- Minimal bony constraint compensated by labrum, capsule, and ligaments
- Position-dependent ligament tension ensuring appropriate restraint at end-ranges
- Rotator cuff force couples maintaining dynamic centration during movement
- Scapulothoracic rhythm expanding the effective arc of elevation
- Negative intraarticular pressure and capsular stiffening as passive mechanisms
Understanding these principles is the foundation for analyzing shoulder dysfunction, interpreting shoulder pathology, and designing evidence-based rehabilitation and surgical strategies.
Sources:
- Campbell's Operative Orthopaedics, 15th Ed 2026 - Anatomy and Biomechanics, Shoulder Injuries chapter
- Miller's Review of Orthopaedics, 9th Edition - Biomechanics (Table 1.44)
- Rheumatology, 2-Volume Set (Elsevier 2022) - Scapulothoracic Joint; Glenohumeral Biomechanics
- Firestein & Kelley's Textbook of Rheumatology - Joint Constraint and Stability
explain me in simple language
Biomechanics of the Shoulder - Simple Explanation
Let me break this down like a story, piece by piece.
🏗️ First, What is the Shoulder?
Think of the shoulder as 4 joints working as a team:
- Glenohumeral (GH) - the main ball-and-socket joint (arm bone + shoulder blade)
- Scapulothoracic (ST) - shoulder blade gliding on the rib cage
- Acromioclavicular (AC) - top of shoulder blade + collar bone
- Sternoclavicular (SC) - collar bone + breastbone
All 4 move together every time you lift your arm. If any one fails, the others suffer.
⚽ The "Golf Ball on a Tee" Problem
The shoulder is built like a golf ball sitting on a tee - the ball (humeral head) is much bigger than the socket (glenoid). This gives you amazing movement in all directions, but very little natural stability.
Compare this to the hip - which is like a ball deep inside a cup - very stable but limited movement.
So how does the shoulder not fall apart? That's what the whole biomechanics is about!
🔒 What Keeps the Shoulder Stable?
Think of stability in two layers:
Layer 1 - Passive (Static) Stabilizers
These work even when your muscles are relaxed.
| Structure | What it does | Simple analogy |
|---|---|---|
| Glenoid Labrum | Deepens the socket by 50% | Like a rubber rim on a cup |
| Glenohumeral Ligaments (3 bands) | Tighten like ropes at end range of motion | Seatbelts - loose normally, tight in a crash |
| Joint Capsule | Surrounds the whole joint | A tight zip-lock bag |
| Negative pressure inside joint | Suction holds the ball in | Like a suction cup on glass |
The most important ligament is the Inferior Glenohumeral Ligament (IGHL) - it acts like a hammock under the humeral head when your arm is raised. When you rotate your arm outward, the front of the hammock tightens. When you rotate inward, the back tightens. This is why shoulder dislocations usually happen in the "arm raised + rotated outward" position - the hammock is at maximum stretch.
Layer 2 - Active (Dynamic) Stabilizers
These work when your muscles contract.
The Rotator Cuff - 4 muscles (SITS):
- Supraspinatus
- Infraspinatus
- Teres minor
- Subscapularis
Their main job is NOT to move the arm - it's to press the ball into the socket and keep it centered. Think of them as the guy-wires on a tent pole - they don't hold the pole up directly, they keep it from swaying side to side.
🔄 Scapulohumeral Rhythm - The 2:1 Rule
When you lift your arm fully overhead (180°), two things happen simultaneously:
- 120° comes from the GH joint (ball rotating in socket)
- 60° comes from the scapula rotating on the rib cage
Ratio = 2:1 (for every 2° of GH motion, the scapula rotates 1°)
Simple analogy: Imagine screwing a bolt. The bolt spins (GH joint), but your whole wrist also rotates (scapula). Both movements together let you reach much further than the bolt alone could.
Why this matters: If your scapula stops rotating properly (weak serratus anterior or trapezius), your shoulder blade lags behind. The supraspinatus tendon then gets pinched between the humeral head and the acromion - this is impingement syndrome.
💪 Force Couples - The Teamwork Concept
This is the most important kinetics concept. A force couple means two muscles pulling in opposite directions to create rotation without translating (shifting) the joint.
Force Couple 1 - Lifting the Arm (Coronal Plane)
Deltoid pulls UP ↑
Rotator Cuff pulls DOWN ↓
= Net result: ARM LIFTS, head stays centered
Without the rotator cuff's downward pull, the deltoid would simply pull the humeral head upward into the acromion. This is exactly what happens in a massive rotator cuff tear - superior migration of humeral head.
Force Couple 2 - Rotating the Arm (Transverse Plane)
Subscapularis pulls FORWARD (front) →
Infraspinatus + Teres Minor pull BACKWARD (rear) ←
= Net result: Balanced rotation, head stays in socket
This is why a balanced rotator cuff is more important than a strong one.
🎯 The Scapular Plane - Why Physios Use It
The scapula faces 30° forward from the side of the body (not directly sideways). This position is called the scapular plane.
Lifting your arm in this plane is the most natural and comfortable arc because:
- The joint capsule is least stressed
- The rotator cuff works most efficiently
- No impingement of the greater tuberosity
This is why physiotherapists prescribe "scaption" (scapular plane elevation) exercises rather than pure sideways raises.
🏋️ What Happens When You Lift Your Arm - Step by Step
- 0-30°: Mostly GH joint moves. Scapula is just "setting" its position.
- 30-90°: Both GH and scapula move together (2:1 ratio kicks in). Humerus must externally rotate to clear the greater tuberosity under the acromion.
- 90-180°: Scapula rotation becomes more dominant. SC joint rotates the clavicle, lifting the whole shoulder girdle.
🔑 Key Numbers to Remember
| Parameter | Value |
|---|---|
| GH abduction range | 120° |
| Scapulothoracic range | 60° |
| Scapulohumeral rhythm ratio | 2:1 |
| Humeral head inclination | 125° |
| Humeral retroversion | 25° |
| Labrum increases socket depth by | 50% |
| Scapular plane angle | 30° anterior to coronal |
🩺 Connecting It to Clinical Practice
| If this biomechanics is disrupted... | This happens clinically |
|---|---|
| Rotator cuff force couple fails | Shoulder impingement, superior head migration |
| Scapulohumeral rhythm disrupted | Secondary impingement, shoulder pain on lifting |
| IGHL stretched/torn | Bankart lesion, recurrent anterior dislocation |
| Serratus anterior weak | Winging of scapula, loss of overhead reach |
| Subacromial space narrows | Supraspinatus tendinopathy, bursitis |
| Negative intraarticular pressure lost | Inferior subluxation (sulcus sign) |
One-Line Summary
The shoulder sacrifices stability for mobility - and compensates through a perfectly balanced team of ligaments, labrum, and rotator cuff muscles working together. When any one member of this team fails, the whole system breaks down.
That is the entire biomechanics of the shoulder in a nutshell.
This is a shared conversation. Sign in to Orris to start your own chat.