Sulfuric acid poisoning in fmt
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the comprehensive information. Here is the complete, exam-ready coverage of sulfuric acid poisoning from the FMT textbook:
Sulfuric Acid Poisoning (H₂SO₄)
The Essentials of Forensic Medicine and Toxicology, 36th edition (2026)
Characteristics
- Pure sulfuric acid = oil of vitriol (H₂SO₄)
- Heavy, odorless, colorless, nonfuming, hygroscopic, oily liquid
- Strong tendency to carbonize organic substances
- Commercial form is brown or dark in color
- Causes superficial burns after 1 second and full-thickness burns after 30 seconds of contact
Signs and Symptoms
| Feature | Description |
|---|---|
| Lips | Swollen, excoriated; brown/black streaks from mouth angles to chin/neck |
| Mouth/throat | Corrosion of mucous membranes; immediate burning pain |
| Teeth | Chalky-white |
| Tongue | Swollen, sodden, black |
| Voice | Hoarse and husky |
| Airways | Stridor, drooling; edema of glottis may cause asphyxia |
| Swallowing | Odynophagia, dysphagia; pharyngeal pain is the most common presenting symptom |
| GI | Epigastric pain spreading to abdomen and thorax; eructation, nausea, vomiting |
| Vomit | Brown or black, mucoid, strongly acid, may contain charred shreds of stomach wall |
| Thirst | Intense; any attempt to drink causes vomiting |
| Abdomen | Distended, very tender; severe constipation; tenesmus |
| Eyes | Sunken; pupils usually dilated |
| Sensorium | Mind remains clear until death |
| Late sequelae | Esophageal, gastric, and pyloric strictures/stenoses; permanent scars in skin and oropharynx |
Fatal Dose and Period
- Fatal Dose: 10-5 mL
- Fatal Period: 12-24 hours
Causes of Death
- Circulatory collapse
- Spasm or edema of glottis
- Collapse due to perforation of stomach
- Toxemia
- Delayed death - hypostatic pneumonia, secondary infection, renal failure, or starvation from esophageal stricture
Complications
Acute:
- Upper airway obstruction and injury
- GI hemorrhage
- Esophageal and gastric perforation
- Sepsis
- Tracheobronchial necrosis, atelectasis, obstructive lung injury
Chronic:
- Esophageal obstruction
- Pyloric stenosis
- Vocal cord paralysis with airway obstruction
Treatment
- NO gastric lavage or emetics (contraindicated - risk of re-exposure and perforation)
- Dilute and neutralize in situ - give 1/4 litre of water, milk, milk of magnesia, lime water, soap suds, or aluminium hydroxide gel within 30 minutes
- Do NOT use alkaline carbonates/bicarbonates (liberate CO₂ → gastric distension → rupture)
- Demulcents - olive oil, milk, egg whites, starch water, mineral oil, melted butter
- Prednisolone 60 mg/day in divided doses to prevent esophageal stricture and for shock (generally not recommended due to increased perforation risk)
- 4 cm diameter mercury-filled bougie passed daily if stricture develops
- Flexible fiber optic endoscopy within first 24-48 hours to assess damage; if circumferential 2nd/3rd-degree burns → exploratory laparotomy; if gastric necrosis → esophagogastrostomy
- Tracheostomy if there is edema of glottis
- NPO - IV nutrition for ~1 week, then liquids → soft food → regular diet
- Skin burns - wash with large amounts of water; apply paste of magnesium oxide or sodium bicarbonate
- Eye burns - irrigate with water or sodium bicarbonate solution for 10-15 minutes (suspended IV bag for low-pressure irrigation is ideal)
- Symptomatic treatment
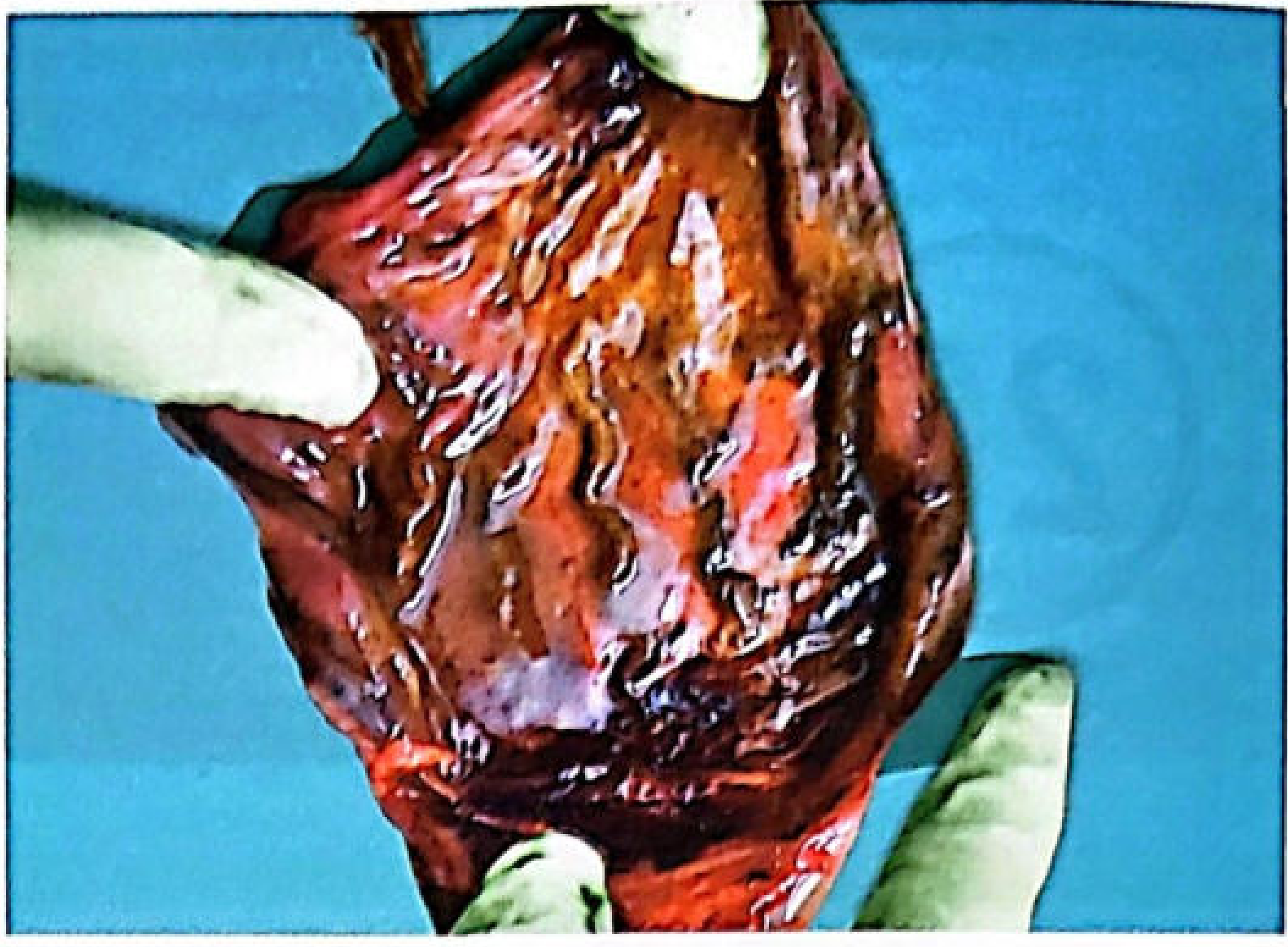
Postmortem Appearances
External
- Corrosion of mucous membranes of lips, mouth, throat
- Corrosion of skin over chin, angles of mouth, and hands
- Necrotic areas initially grayish-white, then become brown or black and leathery
- Examine clothing for burns and stains
Internal
- Upper digestive tract inflamed and swollen with edema and severe interstitial hemorrhage
- Acids mainly affect columnar epithelium of the stomach (squamous esophageal epithelium is relatively resistant) - superficial erosion, coagulation, eschar formation
- Perforation of esophagus is rare
- Greater part of stomach may be converted into a soft, spongy, black mass that readily disintegrates on touch
- Sometimes only the pyloric region is involved (fluid pathway along lesser curvature to pylorus; initial acid exposure causes pyloric spasm, promoting injury there)
- Mucosal ridges more damaged than intervening furrows
- Stomach contains altered blood, dark brown/black from acid hematin; wall studded with acute erosions
- Calcium oxalate crystals may be seen in stomach contents or mucosal scrapings
- Perforation → chemical peritonitis and corrosion of adjacent organs
- Perforation of diaphragm may occur
- Duodenum: similar but less intense changes; small intestine: signs of irritation
- Little to no free acid may be found if victim survived 2+ days (acid converted to normal body substances)
- Larynx and trachea: corrosion or severe inflammation
- Liver and kidney: secondary toxic swelling if survival is prolonged
- Renal tubules: necrosis, primarily in proximal convoluted tubules
Time Course of Injury
| Stage | Time | Features |
|---|---|---|
| Acute inflammatory | Days 1-7 | Perforation and acidosis may occur |
| Granulation | Days 4-7 | |
| Perforation most likely | Days 7-21 | Tissue is weakest at this stage |
| Cicatrization | From ~3rd week | May persist for years; excessive scar → stricture |
Tests / Chemical Analysis
- Only the stomach contents are suitable for analysis (mineral acids decompose rapidly)
- Strong acid chars organic matter
- Barium nitrate or chloride solution produces a white precipitate of barium sulphate (confirmatory for sulfate)
Circumstances of Poisoning
- Accidental - mistaking it for glycerin or castor oil; inhalation of vapors in chemical factories
- Suicidal - most common mode
- Homicide - rare/not used (acid taste, immediate local action, visible physical changes in food make it impractical)
- Also used as an abortifacient (injected into vagina) or out of vengeance
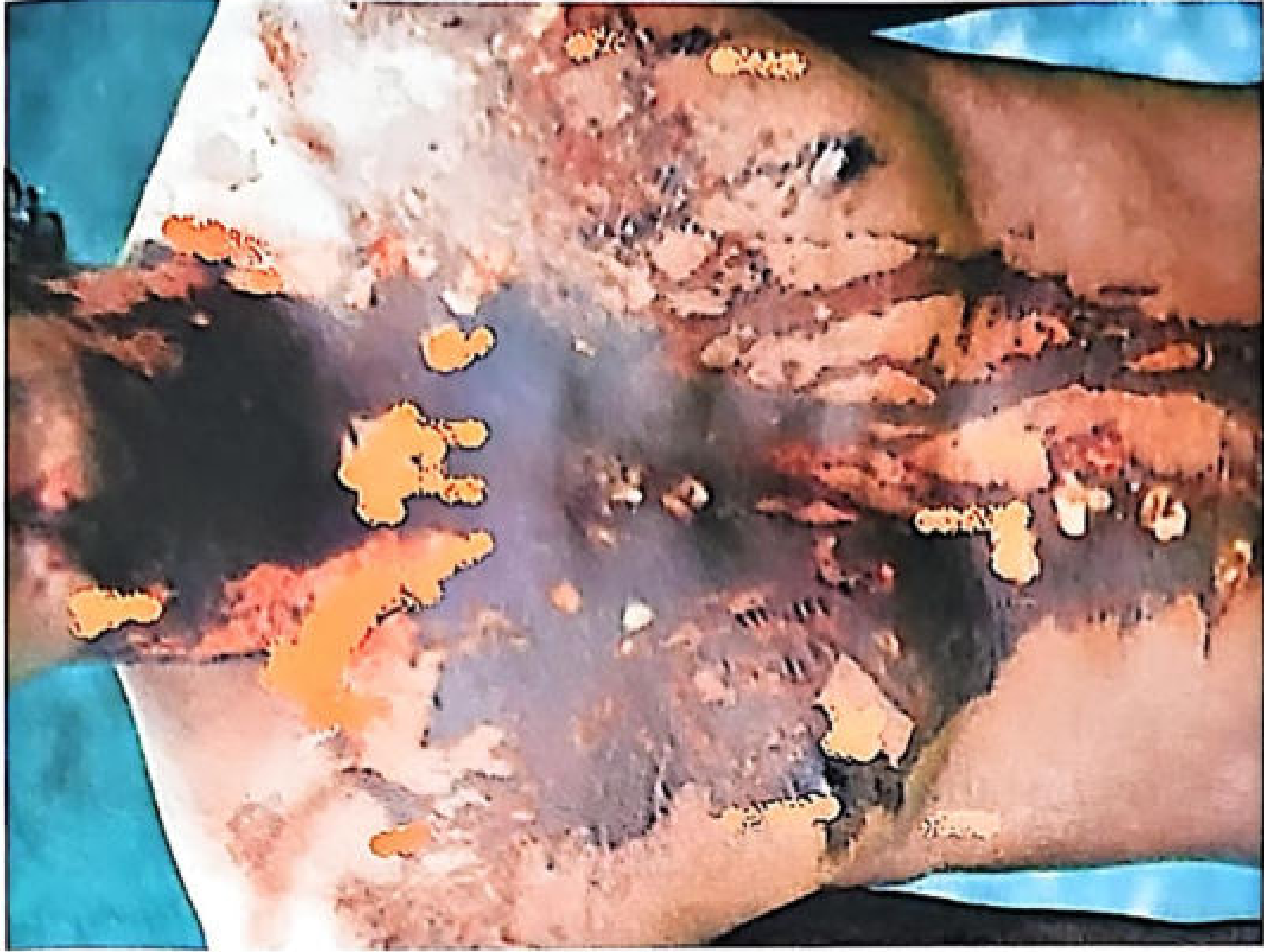
Vitriolage (Vitriol Throwing)
- Throwing of sulfuric acid on another individual
- Done by jealous or disgruntled persons to disfigure and harm enemies
- Burns are penetrating, devitalize tissues, predispose to infection
- Burns initially described as painless
- Repair is slow; scar tissue causes contracture
- Blindness if eyes are involved
- Death from shock or toxemia if extensive area involved
- Other agents also used for vitriolage: nitric acid, carbolic acid, corrosive alkali, juice of marking nut or calotropis
Source: The Essentials of Forensic Medicine and Toxicology, 36th edition (2026), Chapter 26
This is a shared conversation. Sign in to Orris to start your own chat.