Cpr
Reading File
Finding Sources
Searching the Web
CPR guidelines 2025 AHA cardiopulmonary resuscitation steps
Finding Sources
Reading Web Page
https://cpr.heart.org/-/media/CPR-Files/2025-documents-for-c…
Reading File
Reading File
Loading Image
Reading File
Here is a thorough overview of CPR (Cardiopulmonary Resuscitation), drawing from Miller's Anesthesia, Roberts and Hedges' Clinical Procedures in Emergency Medicine, and the 2025 AHA Guidelines.
Cardiopulmonary Resuscitation (CPR)
CPR is an emergency procedure performed when the heart stops beating (cardiac arrest). Each minute without treatment is associated with a 10-15% decrease in survival probability. Prompt, high-quality CPR can up to double a patient's chance of survival.
Adult BLS Algorithm (Healthcare Providers)
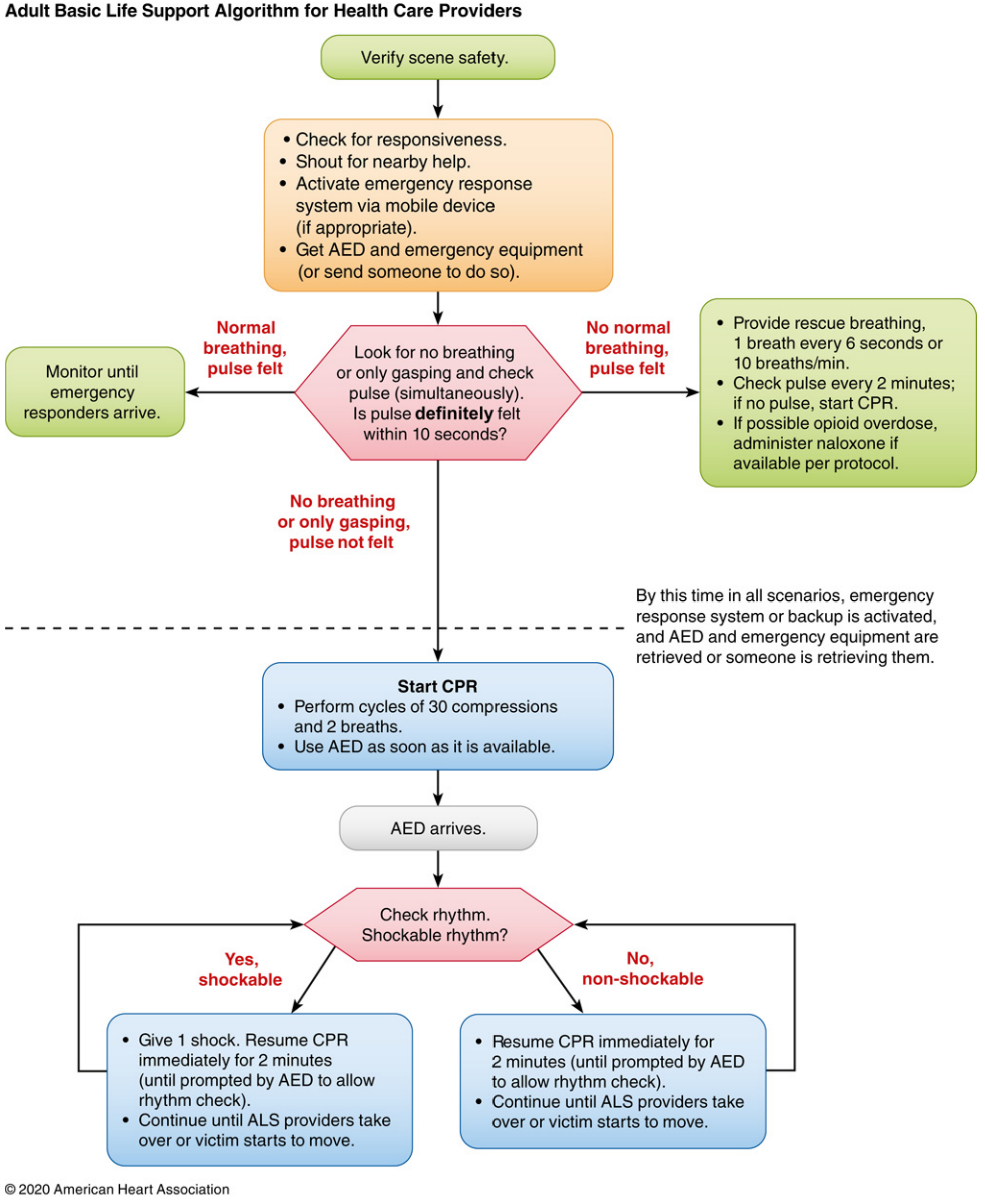
Step-by-Step: Adult CPR
1. Verify Scene Safety
Ensure the environment is safe before approaching.
2. Check Responsiveness
Tap and shout. If unresponsive, shout for nearby help and activate the emergency response system (call 911 or send someone).
3. Assess Simultaneously (≤10 seconds)
- Look for no breathing or only gasping
- Check for a definite pulse
| Finding | Action |
|---|---|
| Normal breathing + pulse felt | Monitor until responders arrive |
| No normal breathing + pulse felt | Rescue breathing: 1 breath every 6 seconds (10/min); check pulse every 2 min |
| No breathing, no pulse | Start CPR |
4. High-Quality CPR
Compressions:
- Place heel of one hand on center of chest (lower half of sternum), other hand on top, fingers interlaced
- Compress to a depth of at least 2 inches (5 cm), no more than 2.4 inches (6 cm)
- Rate: 100-120 compressions/min (do not exceed 140/min -- excessively rapid rate reduces depth)
- Allow complete chest recoil after each compression (do not lean on chest)
- Minimize interruptions; pauses should be <10 seconds
Ventilation (before advanced airway):
- 30 compressions : 2 breaths (30:2 ratio)
- Avoid hyperventilation -- it reduces venous return and worsens outcomes
After advanced airway (ETT or supraglottic):
- 8-10 breaths/min asynchronously
- Continuous chest compressions without pausing for breaths
5. AED Use
- Attach and use an AED as soon as it arrives
- If shockable rhythm (VF/pulseless VT): give 1 shock, then immediately resume CPR for 2 minutes
- If non-shockable: resume CPR immediately for 2 minutes
- Continue until ALS providers take over or victim starts to move
Key Quality Metrics Summary
| Parameter | Target |
|---|---|
| Compression depth (adult) | 2.0 - 2.4 inches (5 - 6 cm) |
| Compression rate | 100 - 120/min |
| Compression:ventilation ratio | 30:2 (before advanced airway) |
| Ventilation rate (advanced airway) | 8-10/min |
| Pause duration | <10 seconds |
| Compression fraction | >60% of resuscitation time |
2025 AHA Guideline Updates (Key Changes)
The 2025 AHA CPR Guidelines (published October 2025 in Circulation) made several notable changes:
- Ventilation is now recommended for both lay rescuers and healthcare professionals when willing and capable -- breaths with compressions improve outcomes (previously compression-only was more broadly acceptable)
- 30:2 remains the compression-to-ventilation ratio before advanced airway
- Choking (adults/children): Alternate 5 back blows + 5 abdominal thrusts until object expelled or victim becomes unresponsive
- Choking (infants): Alternate 5 back blows + 5 chest thrusts (heel of one hand)
- Pediatric CPR: Pause duration should be <10 seconds; for children with arterial line, target diastolic BP ≥30 mmHg (≥25 mmHg in infants)
- Compressor switching for neonates: switch every 2-5 minutes as compression quality deteriorates
Compression-Only CPR
Acceptable for untrained bystanders or those unwilling to give rescue breaths, and can be dispatcher-guided by phone. Survival rates from cardiac arrest of cardiac etiology are similar to conventional CPR when given before EMS arrives. However, for:
- Asphyxiation-related arrest
- Pediatric arrest
- Prolonged CPR
...rescue breaths are strongly recommended alongside compressions.
Common Pitfalls (Known from Clinical Data)
- Compressions too shallow (more common than too deep)
- Rate too slow or too fast (>140/min reduces effective depth)
- Leaning on the chest between compressions (reduces recoil)
- Hyperventilation (raises intrathoracic pressure, decreases venous return)
- Excessive pauses for airway management or rhythm checks
Sources: Miller's Anesthesia 10e, p. 12190-12191 | Roberts and Hedges' Clinical Procedures in Emergency Medicine | 2025 AHA Guidelines for CPR and ECC
This is a shared conversation. Sign in to Orris to start your own chat.