Tongue
Reading File
Asking for Preferences
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Here is a comprehensive overview of the anatomy and structure of the tongue, compiled from authoritative ENT and anatomy textbooks.
Anatomy of the Tongue
Overview
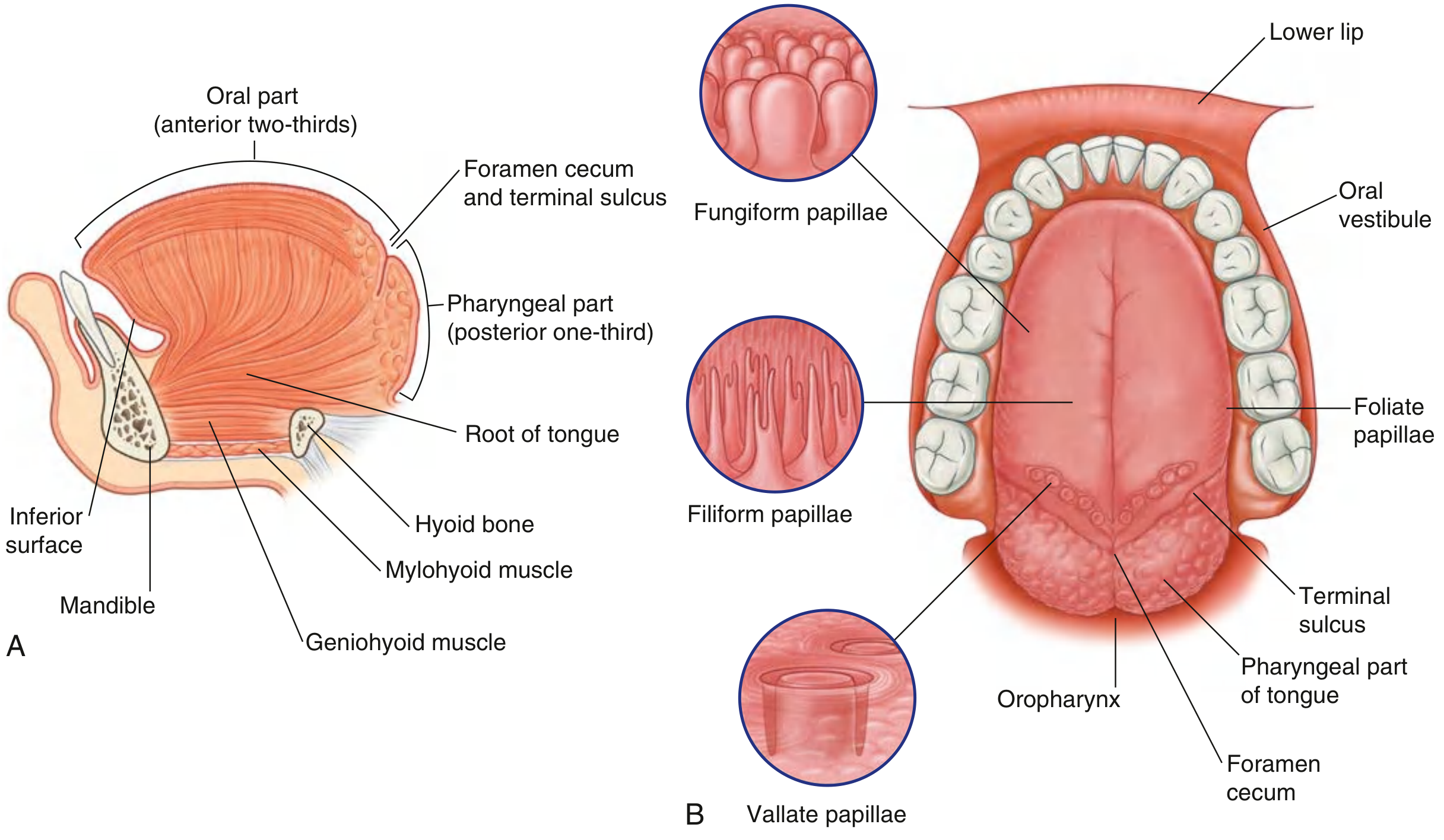
The tongue is a muscular organ occupying the floor of the mouth and the oropharynx. It is divided into:
- Anterior two-thirds (oral tongue) - mobile portion in the oral cavity
- Posterior one-third (tongue base / base of tongue) - fixed portion in the oropharynx
These two parts are separated by the sulcus terminalis, a V-shaped groove, at the apex of which lies the foramen cecum (caecum linguae) - the embryologic origin of thyroid descent, which is the source of lingual thyroids and thyroglossal duct cysts.
Surface Anatomy
Papillae (anterior two-thirds)
| Type | Location | Features |
|---|---|---|
| Filiform | Bulk of anterior tongue | Most numerous; transmit temperature, texture, and pain via trigeminal nerve endings; no taste function |
| Fungiform | Diffuse, majority at anterior 2 cm | Mushroom-shaped; taste buds on superior surface |
| Foliate | Lateral tongue | Taste buds on lateral surface |
| Circumvallate (vallate) | V-shaped row at junction of anterior/posterior tongue | Largest; taste buds on lateral wall of surrounding groove |
Other Surface Features
- Frenulum - anterior fold of mucous membrane tethering the inferior tongue to the floor of the mouth; Wharton's ducts (submandibular gland) open on either side; may be congenitally short (ankyloglossia / "tongue-tie")
- Lingual tonsil - lymphoid tissue at the base of tongue (oropharynx)
- Valleculae - depressions on either side of the midline glossoepiglottic fold, extending to the pharyngoepiglottic fold laterally
Muscles
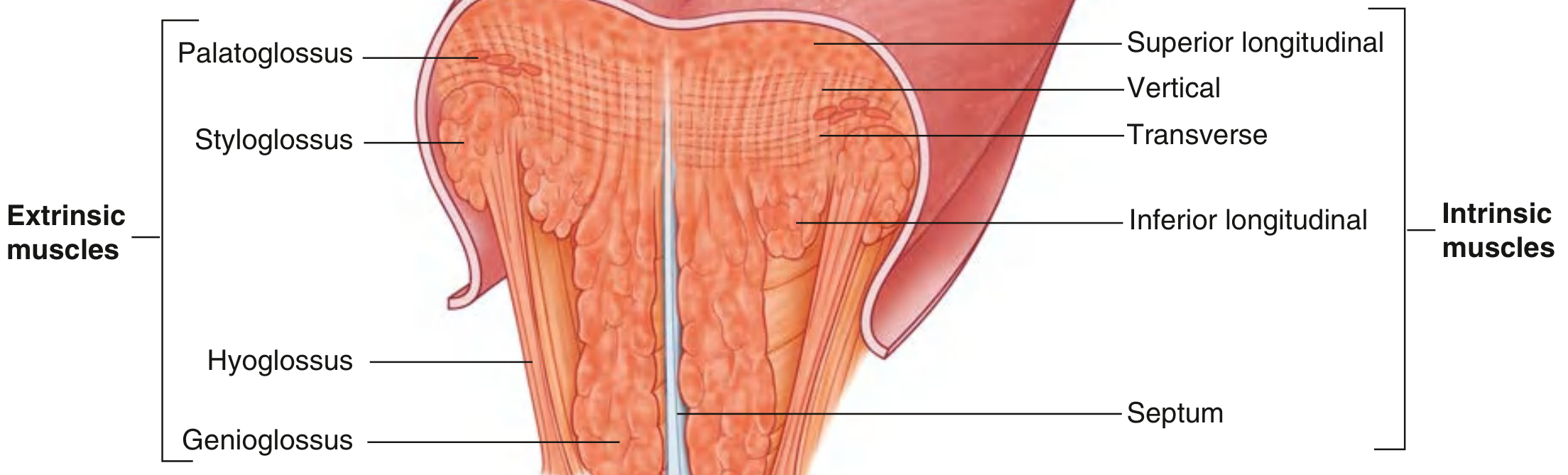
Extrinsic Muscles (move the tongue as a whole)
All extrinsic muscles are innervated by the hypoglossal nerve (CN XII), except palatoglossus.
| Muscle | Origin | Insertion | Function | Nerve |
|---|---|---|---|---|
| Genioglossus | Mental spine of mandible | Hyoid bone + underside of tongue | Protrudes and depresses tongue; provides bulk; bilateral action creates a midline concavity | CN XII |
| Hyoglossus | Body and greater cornu of hyoid | Side of tongue (between inferior longitudinal and styloglossus) | Depresses and retracts tongue | CN XII |
| Styloglossus | Styloid process of temporal bone (anterolateral aspect) and stylomandibular ligament | Tip and side of tongue (decussates with hyoglossus) | Retracts and elevates tongue | CN XII |
| Palatoglossus | Palatine aponeurosis of soft palate | Side and dorsum of tongue | Elevates posterior tongue; closes the oropharyngeal isthmus; initiates swallowing; prevents salivary spillage | CN X (vagus, pharyngeal plexus) |
Key point: Palatoglossus is the only tongue muscle NOT innervated by CN XII - it is innervated by the vagus nerve via the pharyngeal plexus.
Intrinsic Muscles (change shape of the tongue)
All innervated by CN XII; blood supply from the lingual artery.
| Muscle | Action |
|---|---|
| Superior longitudinal | Shortens tongue; pulls apex and sides up - makes dorsum concave |
| Inferior longitudinal | Shortens tongue; pulls apex down - makes dorsum convex |
| Transverse | Narrows and elongates tongue |
| Vertical | Flattens and widens tongue |
Together, the intrinsic muscles provide the tongue with precise, highly varied mobility for speech, swallowing, and mastication.
Fibrous Septum (Septum Linguae)
A midline fibrous structure defining the left/right halves; contains a triangular fat pad visible on axial CT.
Vascular Supply
- Arterial: Lingual artery - the 2nd branch of the external carotid artery (some sources cite it as the 3rd)
- Branches: dorsal lingual, sublingual, and deep lingual arteries
- Venous drainage: Lingual vein and vena comitans of the hypoglossal nerve (Ranine vein)
Lymphatic Drainage
| Region | Drainage |
|---|---|
| Tongue tip | Submental nodes |
| Central anterior tongue | Ipsilateral AND contralateral nodes |
| Lateral anterior tongue | Ipsilateral nodes (levels I-III); possible skip drainage to level IV |
| Posterior tongue (base) | Bilateral deep cervical nodes (jugulodigastric) |
The bilateral drainage of the posterior tongue is clinically significant - cancers of the tongue base can metastasize to the contralateral neck.
Sensory Innervation
| Region | Modality | Nerve |
|---|---|---|
| Anterior 2/3 | Touch, pain, temperature (general sensation) | Lingual nerve (CN V3) |
| Posterior 1/3 | Touch, gag reflex (visceral afferent) | Glossopharyngeal nerve (CN IX) |
Taste (Special Sensory)
Five basic tastes: sweet, sour, bitter, salty, umami.
| Region | Papillae | Pathway |
|---|---|---|
| Anterior 2/3 | Fungiform and foliate | Lingual nerve → chorda tympani (CN VII) → geniculate ganglion → nucleus solitarius |
| Posterior 1/3 | Foliate, circumvallate, posterior oropharynx | Glossopharyngeal (CN IX) → inferior petrosal ganglion → nucleus solitarius |
Flavor perception is a combination of taste + olfactory + trigeminal inputs, modulated by emotion, metabolic state, and learning.
Motor Innervation Summary (CN XII - Hypoglossal)
- All intrinsic muscles
- Genioglossus, hyoglossus, styloglossus
- Genioglossus is the most important clinically - loss of its tone (e.g., in unconsciousness or CN XII palsy) causes the tongue to fall backwards and obstruct the airway
- In CN XII palsy, the tongue deviates toward the side of the lesion on protrusion (unopposed genioglossus on the intact side pushes the tongue to the affected side)
Sources: K.J. Lee's Essential Otolaryngology, p. 665; Scott-Brown's Otorhinolaryngology Head & Neck Surgery, Ch. 41
Point to be said during viva regarding tongue
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Here are the key high-yield viva points on the tongue, organized by topic:
Tongue - High-Yield Viva Points
1. Parts & Basic Description
- Muscular organ of deglutition, taste, and speech
- Partly oral, partly pharyngeal in position
- Divided into anterior 2/3 (oral tongue) and posterior 1/3 (tongue base/root)
- Separated by the sulcus terminalis - a V-shaped groove
- At the apex of the sulcus terminalis lies the foramen cecum - the embryologic origin of thyroid descent
2. Papillae (Classic Viva Question)
| Type | Location | Taste Buds? | Nerve |
|---|---|---|---|
| Filiform | Bulk of anterior 2/3 | No | CN V3 (temperature, pain, touch) |
| Fungiform | Scattered on dorsum, majority at anterior 2 cm | Yes | Chorda tympani (CN VII) |
| Foliate | Lateral tongue | Yes | Chorda tympani (anterior), CN IX (posterior) |
| Circumvallate | V-row just anterior to sulcus terminalis; 8-12 in number | Yes | CN IX |
Viva point: Filiform papillae are the ONLY papillae with NO taste buds. They have a mechanical/masticatory function - increase friction between tongue and food.
3. Muscles
Rule to remember:
All tongue muscles = CN XII, EXCEPT palatoglossus = CN X (vagus)
Extrinsic Muscles
| Muscle | Origin | Function |
|---|---|---|
| Genioglossus | Mental spine of mandible | Protrudes + depresses tongue; provides bulk |
| Hyoglossus | Greater cornu + body of hyoid | Depresses + retracts tongue |
| Styloglossus | Styloid process | Retracts + elevates tongue |
| Palatoglossus | Palatine aponeurosis | Elevates posterior tongue; closes oropharyngeal isthmus |
Intrinsic Muscles (all CN XII)
| Muscle | Action |
|---|---|
| Superior longitudinal | Shortens; curls apex up - concave dorsum |
| Inferior longitudinal | Shortens; pulls apex down - convex dorsum |
| Transverse | Narrows + elongates |
| Vertical | Flattens + widens |
Viva point: Genioglossus is the most clinically important tongue muscle - loss of tone (e.g., unconsciousness, CN XII palsy) causes tongue to fall back and obstruct the airway.
4. Nerve Supply (Most Asked!)
Motor
- CN XII (Hypoglossal) - all intrinsic + extrinsic muscles except palatoglossus
- CN X (Vagus) - palatoglossus only
Sensory (General)
- Anterior 2/3 - Lingual nerve (CN V3)
- Posterior 1/3 - Glossopharyngeal nerve (CN IX)
Taste (Special Sensory)
- Anterior 2/3 - Chorda tympani (branch of CN VII) via lingual nerve
- Posterior 1/3 - CN IX
- Extreme posterior + epiglottis - Superior laryngeal nerve (CN X)
Viva trick: Sensory and taste are supplied by DIFFERENT nerves on the anterior 2/3 - touch by CN V3, taste by CN VII (chorda tympani).
5. Blood Supply
- Arterial: Lingual artery (branch of external carotid artery)
- Venous: Lingual vein + Ranine vein (vena comitans of hypoglossal nerve)
6. Lymphatic Drainage
| Region | Drainage |
|---|---|
| Tongue tip | Submental nodes |
| Central anterior tongue | Bilateral (ipsilateral + contralateral) |
| Lateral anterior tongue | Ipsilateral (levels I-III), may skip to level IV |
| Posterior tongue (base) | Bilateral deep cervical (jugulodigastric) |
Viva point: Posterior tongue drains bilaterally - this is WHY carcinoma of tongue base can metastasize to the contralateral neck, requiring bilateral neck dissection.
7. Embryology
- Tongue appears at 4 weeks
- Anterior 2/3 - from 2 lateral lingual swellings + 1 tuberculum impar (all from 1st pharyngeal arch) → sensory by CN V3
- Posterior 1/3 - from copula (2nd, 3rd, 4th arch); 3rd arch tissue overgrows 2nd → sensory by CN IX
- Tongue muscles - derived from occipital somite myoblasts migrating into the tongue → hence innervated by CN XII (hypoglossal)
- Foramen cecum = site where thyroid diverticulum invaginates → thyroid descends from here; persistence gives thyroglossal duct cyst or lingual thyroid
8. Clinical Viva Points
| Finding | Cause |
|---|---|
| Deviation on protrusion | CN XII palsy - tongue deviates toward the SIDE OF LESION (unopposed contralateral genioglossus pushes it across) |
| Macroglossia | Acromegaly, cretinism, myxoedema, lymphangioma, amyloidosis |
| Tremor on protrusion | Thyrotoxicosis (classic); also delirium tremens, Parkinsonism |
| Smooth/bald tongue (atrophic papillae) | Vitamin B12 deficiency, iron-deficiency anaemia |
| Dry, brown tongue | Dehydration, acute intestinal obstruction, uraemia |
| Black hairy tongue | Fungal infection (Candida/Aspergillus), often in heavy smokers |
| Leukoplakia | Chronic superficial glossitis - whitish thickened epithelium; premalignant |
| Median rhomboid glossitis | Lozenge-shaped loss of papillae anterior to foramen cecum; distinguish from lingual thyroid and carcinoma |
| Ankyloglossia (tongue-tie) | Congenitally short frenulum; causes inability to protrude tongue |
| Inability to protrude (adults) | Carcinoma of tongue involving floor of mouth |
9. One-Liner Facts Examiners Love
- Undersurface of tongue - no papillae; has frenulum, lingual vein, and fimbriated fold
- Lingual tonsil - lymphoid tissue on posterior 1/3 (pharyngeal surface); no papillae on this surface
- Valleculae - depressions on either side of the midline glossoepiglottic fold; part of oropharynx
- Fibrous septum (septum linguae) - divides tongue into two halves; contains a triangular fat pad visible on axial CT
- Wharton's duct (submandibular gland) opens on either side of the frenulum
- Only 8-12 circumvallate papillae despite being the largest and most prominent
Sources: S. Das - Manual of Clinical Surgery; Scott-Brown's Otorhinolaryngology; Gray's Anatomy for Students; Langman's Medical Embryology; K.J. Lee's Essential Otolaryngology
Can u please use the source from bd chaurasiya
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Unfortunately, BD Chaurasia's Human Anatomy is not available in the textbook library. The anatomy books we have are:
- Gray's Anatomy for Students
- Color Atlas of Human Anatomy (Vols 1, 2, 3)
- Netter's Atlas of Human Anatomy
- THIEME Atlas of General Anatomy
- Color Atlas of Ultrasound Anatomy
Would you like me to compile the tongue viva points using Gray's Anatomy for Students instead? That is the closest equivalent to BD Chaurasia in terms of depth and style for anatomy viva preparation - it covers all the same topics (muscles, nerve supply, blood supply, lymphatics, embryology) in a structured format.
Alternatively, I can use Netter's Atlas for visual reference alongside Gray's. Just let me know!
Compile tongue viva points using Gray's Anatomy
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Here are the complete tongue viva points compiled directly from Gray's Anatomy for Students:
Tongue - Viva Points
Source: Gray's Anatomy for Students
Fig. 8.257 - Tongue Overview (Gray's)
1. Definition & Basic Description
- The tongue is a muscular structure forming part of the floor of the oral cavity and part of the anterior wall of the oropharynx
- Anterior part is in the oral cavity - somewhat triangular in shape with a blunt apex directed anteriorly, sitting immediately behind the incisor teeth
- The root of the tongue is attached to the mandible and the hyoid bone
2. Parts of the Tongue
| Part | Surface orientation | Location |
|---|---|---|
| Anterior 2/3 (oral part) | Horizontal plane, faces upward | Oral cavity |
| Posterior 1/3 (pharyngeal part) | Curves inferiorly, more vertical plane | Oropharynx |
- Separated by a V-shaped terminal sulcus
- The terminal sulcus forms the inferior margin of the oropharyngeal isthmus between oral and pharyngeal cavities
- At the apex of the V = foramen cecum - the site where epithelium invaginated in the embryo to form the thyroid gland
- In some individuals a thyroglossal duct persists, connecting the foramen cecum to the thyroid gland in the neck
3. Surfaces
Dorsal (Superior) Surface
- Anterior 2/3 covered by hundreds of papillae
- Posterior 1/3 (pharyngeal surface) has no papillae - mucosa is irregular due to many small nodules of lymphoid tissue = lingual tonsil
Inferior Surface
- No papillae
- Has a single median fold - frenulum of the tongue - continuous with the floor of oral cavity mucosa
- Underlies the lower margin of the midline sagittal septum (which internally separates left and right halves of the tongue)
- On each side of the frenulum = lingual vein
- Lateral to each lingual vein = fimbriated fold
4. Papillae (Classic Viva)
"All papillae increase the area of contact between the tongue surface and contents of the oral cavity. All EXCEPT filiform papillae have taste buds." - Gray's
| Type | Shape | Location | Taste Buds? |
|---|---|---|---|
| Filiform | Small cone-shaped, end in one or more points | Bulk of dorsum, diagonal rows | NO |
| Fungiform | Rounder, larger than filiform | Concentrated along margins of tongue | Yes |
| Vallate (Circumvallate) | Blunt-ended cylindrical invaginations - LARGEST | Single V-shaped line just anterior to terminal sulcus | Yes |
| Foliate | Linear folds of mucosa | Sides of tongue near terminal sulcus | Yes |
Viva key: Only 8 to 12 vallate papillae exist, in a single V-shaped row.
5. Muscles of the Tongue
- The tongue is completely divided into left and right halves by a median sagittal septum of connective tissue
- Therefore all muscles of the tongue are paired
- Two groups: intrinsic and extrinsic
The Golden Rule (Gray's): "Except for the palatoglossus, which is innervated by the vagus nerve [X], all muscles of the tongue are innervated by the hypoglossal nerve [XII]."
Intrinsic Muscles (origin and insertion within tongue)
| Muscle | Action |
|---|---|
| Superior longitudinal | Shortens tongue; curls apex and sides upward |
| Inferior longitudinal | Shortens tongue; uncurls apex, turns it downward |
| Transverse | Narrows and elongates tongue |
| Vertical | Flattens and widens tongue |
- Working in pairs or one side at a time, intrinsic muscles contribute to precision movements for speech, eating, and swallowing
Extrinsic Muscles (origin outside tongue, insert into tongue)
| Muscle | Origin | Insertion | Function | Nerve |
|---|---|---|---|---|
| Genioglossus | Superior mental spines of mandible (posterior surface) | Body of hyoid + entire length of tongue | Protrudes tongue; depresses center | CN XII |
| Hyoglossus | Entire length of greater horn + adjacent body of hyoid | Lateral surface of tongue (between genioglossus medially and styloglossus laterally) | Depresses tongue | CN XII |
| Styloglossus | Anterior surface of styloid process | Lateral surface of tongue (blends with superior margin of hyoglossus) | Retracts tongue; pulls back superiorly | CN XII |
| Palatoglossus | Undersurface of palatine aponeurosis | Lateral margin of tongue | Elevates back of tongue; depresses palate; moves palatoglossal fold toward midline | CN X (vagus, via pharyngeal plexus) |
Genioglossus is the most important clinically - Gray's states: "If the nerve on one side is not fully functional, the tip of the tongue will point to that side" on protrusion.
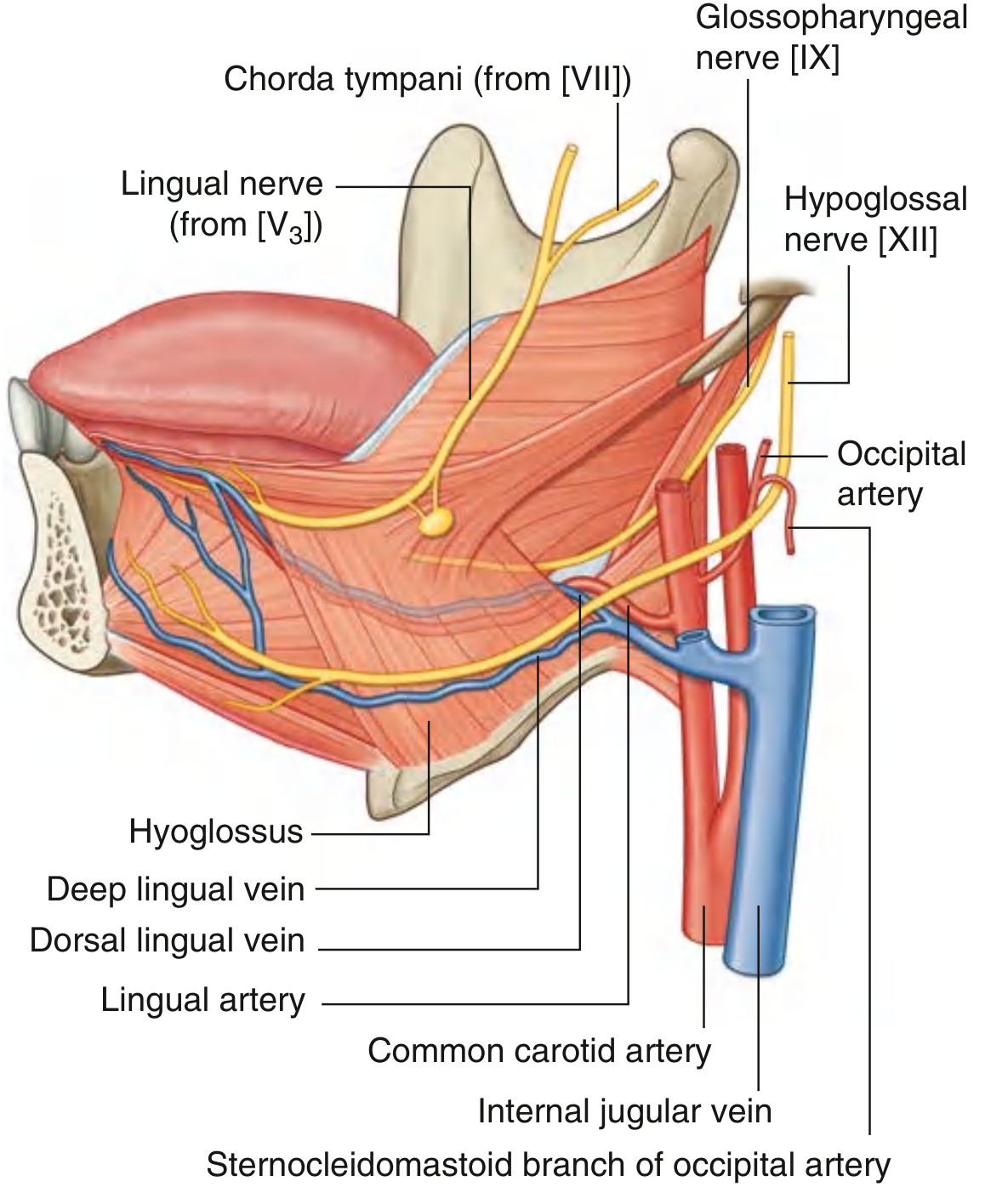
Hyoglossus - The Key Landmark Muscle
Gray's specifically highlights hyoglossus as an important anatomical landmark in the floor of the oral cavity:
- Deep to hyoglossus (between hyoglossus and genioglossus): Lingual artery
- External (superficial) surface of hyoglossus: Hypoglossal nerve [XII] and Lingual nerve (V3)
This is a classic viva question - what passes deep vs. superficial to hyoglossus.
6. Vessels
Arterial Supply
- Lingual artery - branch of the external carotid artery, arising at the level of the tip of the greater horn of the hyoid bone
- It forms an upward bend, loops downward and forward, passes deep to hyoglossus
- Travels forward in the plane between hyoglossus and genioglossus to the apex
- Also supplies: sublingual gland, gingiva, oral mucosa of the floor
Venous Drainage
- Deep lingual veins - visible through mucosa on undersurface; travel with hypoglossal nerve on external surface of hyoglossus → drain into internal jugular vein
- Dorsal lingual veins - follow the lingual artery between hyoglossus and genioglossus → drain into internal jugular vein
7. Innervation
"Innervation of the tongue is complex and involves a number of nerves." - Gray's
General Sensation
| Region | Nerve |
|---|---|
| Anterior 2/3 (oral part) | Lingual nerve (branch of mandibular [V3]) |
| Posterior 1/3 (pharyngeal part) | Glossopharyngeal nerve [IX] |
Taste (Special Sensory)
| Region | Nerve |
|---|---|
| Anterior 2/3 | Chorda tympani (branch of CN VII) - fibers travel within the lingual nerve, then enter the chorda tympani in the infratemporal fossa |
| Posterior 1/3 | Glossopharyngeal nerve [IX] |
Motor
- All tongue muscles → Hypoglossal nerve [XII]
- Palatoglossus only → Vagus nerve [X]
Course of Lingual Nerve (Gray's)
- Originates in infratemporal fossa as branch of V3
- Passes through gap (oropharyngeal triangle) between mylohyoid, superior constrictor, and middle constrictor
- Passes immediately inferior to the attachment of superior constrictor to the mandible
- Continues forward on medial surface of mandible adjacent to the last molar tooth (can be palpated here clinically)
- Loops under the submandibular duct
- Ascends into tongue on the external surface of hyoglossus
Course of Hypoglossal Nerve [XII] (Gray's)
- Leaves skull through hypoglossal canal
- Descends in the neck to just below angle of mandible
- Crosses the external carotid artery, crosses the loop of the lingual artery
- Reaches external surface of lower 1/3 of hyoglossus
- Enters tongue through the oropharyngeal triangle
- C1 fibers hitch a ride on CN XII and leave as:
- Superior root of ansa cervicalis
- Thyrohyoid branch (innervates thyrohyoid)
- Branch to geniohyoid
8. Lymphatic Drainage
"All lymphatic vessels from the tongue ultimately drain into the deep cervical chain of nodes along the internal jugular vein." - Gray's
| Region | Drainage pathway |
|---|---|
| Pharyngeal part (posterior 1/3) | Through pharyngeal wall → mainly jugulodigastric node of deep cervical chain |
| Oral part (anterior 2/3) | Directly into deep cervical nodes + indirectly through mylohyoid → submental and submandibular nodes |
| Tip of tongue | Through mylohyoid → submental nodes → mainly jugulo-omohyoid node of deep cervical chain |
- Submental nodes lie inferior to mylohyoid muscles, between the digastric muscles
- Submandibular nodes lie below the floor of the oral cavity along the inner aspect of the inferior margins of the mandible
9. One-Liner Viva Bombs from Gray's
| Question | Answer |
|---|---|
| What is the tongue? | Muscular structure forming part of the floor of oral cavity AND anterior wall of oropharynx |
| How many vallate papillae? | Only 8 to 12 |
| Which papillae have NO taste buds? | Filiform only |
| Which muscle is tested when you ask a patient to "stick tongue out"? | Genioglossus (tests CN XII) |
| Which is the exception to CN XII for tongue muscles? | Palatoglossus (CN X via pharyngeal plexus) |
| What passes deep to hyoglossus? | Lingual artery |
| What passes superficial to hyoglossus? | Lingual nerve (V3) and Hypoglossal nerve (XII) |
| What are the venous tributaries of tongue? | Deep lingual vein + Dorsal lingual vein (both drain to internal jugular vein) |
| What terminates at the foramen cecum? | The embryologic thyroid descent (origin of thyroglossal duct cysts and lingual thyroid) |
| Where does tip of tongue drain? | Submental nodes → jugulo-omohyoid node |
Source: Gray's Anatomy for Students, Chapter 8 - Head and Neck, pp. 1234-1241
This is a shared conversation. Sign in to Orris to start your own chat.