Epistaxsis causes, bleeding site( how to differentiate ), risk factors, investigations, management in emergency opd and age wise
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information from multiple authoritative sources. Let me compile the complete answer.
Epistaxis: Complete Clinical Guide
Sources: Cummings Otolaryngology; Rosen's Emergency Medicine; Bailey & Love's Surgery; Roberts & Hedges' Clinical Procedures
Vascular Anatomy - The Foundation
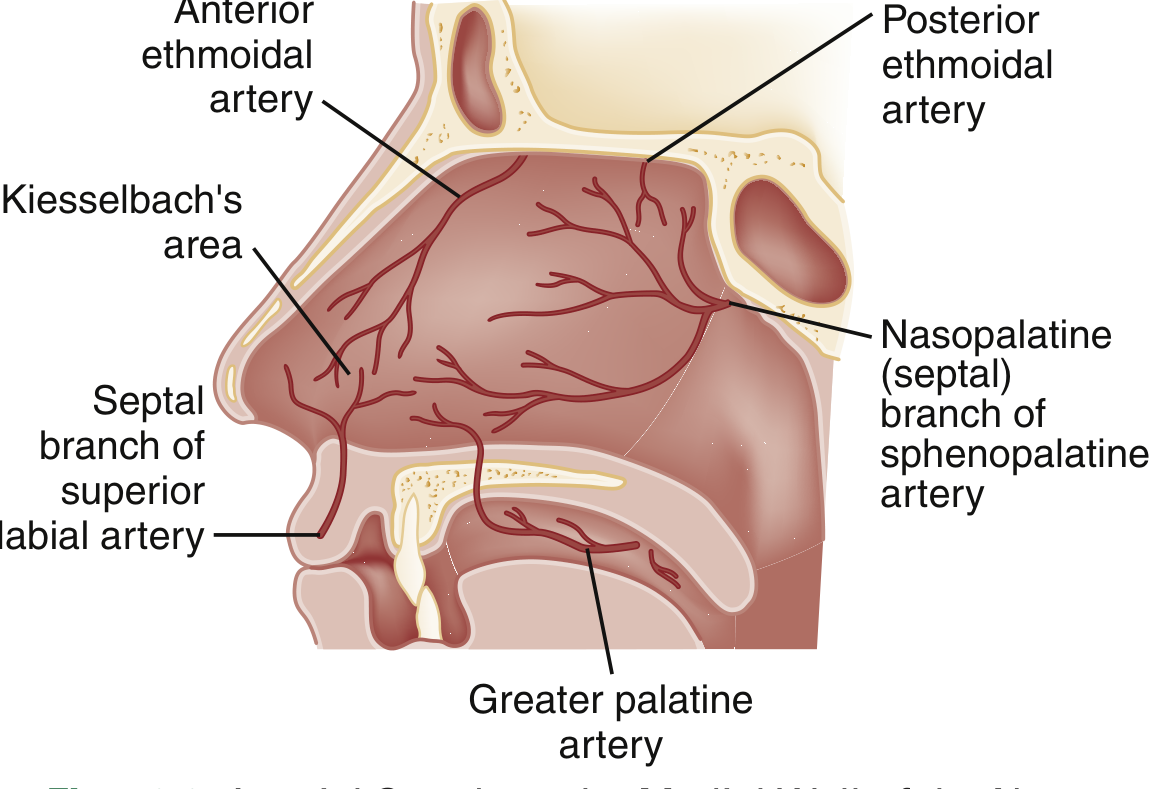
The nasal cavity receives a dual blood supply from both carotid systems:
External Carotid Artery:
- Internal maxillary artery → sphenopalatine artery (posterior septal + posterior lateral nasal branches), descending palatine → greater palatine artery
- Facial artery → superior labial artery
Internal Carotid Artery:
- Ophthalmic artery → anterior ethmoidal artery, posterior ethmoidal artery
1. Bleeding Site: Anterior vs. Posterior Differentiation
Kiesselbach's Plexus (Little's Area) - Anterior
A confluence of 4 arterial branches at the anteroinferior septum:
- Anterior ethmoidal artery
- Sphenopalatine artery
- Greater palatine artery
- Superior labial artery
Woodruff Plexus - Posterior
Located posterior to the inferior turbinate root and horizontal part of the middle turbinate; supplied by sphenopalatine and ascending pharyngeal arteries.
| Feature | Anterior Epistaxis | Posterior Epistaxis |
|---|---|---|
| Frequency | >90% of cases | ~10% |
| Source | Kiesselbach's plexus (Little's area) | Woodruff plexus / sphenopalatine branches |
| Age group | Children, young adults | Elderly (>50 years) |
| Laterality | Usually unilateral | Often bilateral or non-localizable |
| Severity | Mild to moderate, self-limiting | Severe, arterial, profuse |
| Visibility | Visible on anterior rhinoscopy | Not visible anteriorly |
| Blood flow direction | Predominantly out of nostril | Down posterior pharynx (patient swallows blood, nausea, haematemesis) |
| Response to pressure | Stops with external pressure | Does NOT stop with external pressure |
| Responds to anterior pack | Yes | No - needs posterior pack |
| Associated features | Dry mucosa, nose picking | Hypertension, arteriosclerosis, anticoagulants |
Practical clue: If bleeding continues despite a properly placed anterior nasal pack, suspect a posterior source.
2. Causes
Local Causes
| Category | Specific Causes |
|---|---|
| Traumatic | Nose picking (most common), vigorous nose blowing, nasal/facial fractures, foreign body, chemical injury, piercings, skull base fractures involving anterior ethmoidal arteries |
| Mucosal irritation | Cold/dry weather, low humidity, CPAP/nasal cannula, septal deviation, septal perforation |
| Infections | Viral/bacterial/fungal rhinosinusitis, granulomatous disorders |
| Neoplastic | Juvenile angiofibroma (adolescent boys, life-threatening), haemangioma, pyogenic granuloma, inverted papilloma, carcinoma, sarcoma, lymphoma |
| Vascular | HHT (Osler-Weber-Rendu disease) - autosomal dominant, recurrent multifocal bleeds from thin-walled telangiectasias |
| Iatrogenic | Post-nasal/sinus/septal surgery, NG tube placement |
Systemic Causes
| Category | Specific Causes |
|---|---|
| Cardiovascular | Hypertension, arteriosclerosis |
| Coagulation disorders | Haemophilia A/B, von Willebrand disease, thrombocytopenia (primary, drug-induced, leukaemia/lymphoma), DIC |
| Medications | Warfarin, NOACs (rivaroxaban, apixaban), heparin, aspirin, clopidogrel, topical nasal steroids, chronic nasal vasoconstrictors |
| Liver disease | Chronic liver disease / cirrhosis (impaired clotting factor synthesis) |
| Renal disease | CKD (platelet dysfunction) |
| Nutritional | Vitamin K deficiency, folic acid deficiency |
| Drug/toxin | Cocaine abuse (mucosal destruction), chronic alcohol use |
| Haematologic malignancy | Leukaemia, lymphoma |
| Chemotherapy | Thrombocytopenia |
3. Risk Factors
- Age: bimodal peaks - children <10 years and adults >35-50 years
- Male sex (estrogen appears to have a protective effect on nasal vasculature)
- Winter/dry climate (nasal mucosal desiccation)
- Anticoagulant or antiplatelet medications
- Hypertension (associated with persistent/severe bleeding, though causation unproven)
- Bleeding disorders (haemophilia, vWD, thrombocytopenia)
- Nasal septal deviation
- Recurrent URTIs
- HHT (family history)
- Chronic liver/renal disease
- Prior nasal surgery (altered anatomy)
- Cocaine use (mucosal damage)
4. Investigations
Clinical Assessment First
- Airway, breathing, circulation (assess hemodynamic stability)
- Anterior rhinoscopy with nasal speculum (vertical opening to visualize septum)
- Nasendoscopy (rigid or flexible) to identify posterior source
- Ask the patient to blow the nose to clear clots, then apply pressure + oxymetazoline 0.05% spray before examination
Laboratory Investigations
NOT routinely indicated for simple anterior epistaxis.
Indicated when:
- Severe hemorrhage with haemodynamic compromise
- Anticoagulant/antiplatelet therapy
- Suspected coagulopathy or bleeding disorder
- Advanced liver disease / haematologic malignancy
| Investigation | Indication |
|---|---|
| FBC (CBC) | Assess Hb (transfuse if <7 g/dL, or <8 g/dL with cardiovascular disease), platelet count |
| Coagulation screen (PT, aPTT, INR) | Anticoagulant use, liver disease, DIC |
| Blood group and crossmatch | Severe haemorrhage |
| Liver function tests | Suspected liver disease |
| Renal function | CKD |
| Blood film | Suspected leukaemia/haematologic malignancy |
| vWF antigen/activity | Recurrent epistaxis in young patient |
| Nasal endoscopy | Identify source, especially posterior bleeds |
| CT sinuses/nose | Suspected tumour, trauma, vascular malformation |
| Contrast CT/MRI | Juvenile angiofibroma (anterior bowing of posterior antral wall = Holman-Miller / antral sign) |
| Angiography | Pre-embolisation workup for refractory cases |
5. Emergency OPD Management - Step-by-Step
STEP 1: Initial Assessment and Stabilisation
- Assess airway, breathing, circulation - address haemodynamic instability first
- Sit patient upright, leaning slightly forward (prevents swallowing blood, reduces aspiration risk)
- Large-bore IV access + fluid resuscitation if haemodynamically compromised
- Pulse oximetry, BP monitoring
- Patient is often anxious and hypertensive - address both
STEP 2: First Aid Measures
- Instruct patient to blow nose to clear clots
- Apply 2 sprays of oxymetazoline 0.05% (or xylometazoline) into affected nostril - vasoconstriction facilitates examination and haemostasis
- Apply firm digital pressure on the cartilaginous (soft) part of the nose (not the bony bridge) for 10-15 minutes continuous; a nose clip is superior to manual pressure alone
- Apply ice pack over nose bridge
STEP 3: Local Anaesthesia and Examination
- Apply 2% aqueous lidocaine via mucosal atomisation or soaked pledget (with adrenaline for added vasoconstriction)
- Examine with nasal speculum (opened vertically, floor of nose parallel to floor)
- Identify bleeding source via anterior rhinoscopy or nasendoscopy
STEP 4: Chemical Cautery (if source identified)
- Silver nitrate cauterisation - first-line when bleeding point visible; highly effective with low re-bleeding rate
- Cauterise from periphery to centre, superiorly to inferiorly (blood makes sticks ineffective)
- Contact with mucosa no longer than 15 seconds to prevent septal necrosis
- NEVER cauterise both sides of the septum simultaneously - risk of septal perforation and necrosis
- If cautery fails, apply topical thrombogenic agents: Gelfoam (absorbable gelatin sponge) or Surgicel (oxidised cellulose)
STEP 5: Topical Tranexamic Acid
- 500 mg of IV tranexamic acid solution applied to a nasal pledget or atomised into the nose
- Evidence supports benefit in reducing bleeding at 10 minutes and re-bleeding at 7-10 days
- Superior to anterior nasal packing specifically in patients on antiplatelet drugs
- No significant increase in adverse events
STEP 6: Anterior Nasal Packing (if cautery fails)
Options:
- Merocel (polyvinyl alcohol) nasal tampon - inserted along floor of nose, expands with moisture; may control high-pressure arterial bleeds; remove after 3-5 days
- Rapid Rhino balloon catheter - coated in procoagulant material, inflated with air along floor of nose; self-lubricating
- Vaseline-impregnated ribbon gauze - traditional, effective but uncomfortable; layered from floor upwards in accordion fashion
- Absorbable packs (Nasopore, MeroGel) - dissolve within 1 week; better tolerated but less pressure
Key points for packing:
- Insert along the floor of the nose in an inferior vector (not superiorly against middle turbinate)
- Moisten before removal to prevent mucosal trauma
- For uncontrolled bleeding despite anterior pack in one naris, insert second anterior pack in opposite naris
Prophylactic antibiotics: NOT routinely recommended with anterior packing.
Admission not always required for unilateral anterior packing; bilateral packing or posterior packing requires inpatient monitoring.
STEP 7: Posterior Packing (if anterior packing fails - posterior epistaxis)
- Indicated when bleeding continues despite properly placed anterior nasal packing
- Options:
- Double balloon catheter (e.g., Brighton/Epistat balloon): posterior balloon inflated in nasopharynx, anterior balloon in nasal cavity
- Foley catheter + anterior gauze pack - classical method (14-16 Fr Foley, balloon inflated with 7-10 mL saline in nasopharynx)
- Gauze postnasal pack under GA in theatre
- Requires inpatient admission with monitoring (risk of hypoxia, eustachian tube dysfunction, pain)
- ENT consultation mandatory
STEP 8: Refractory/Surgical Management
| Procedure | Indication |
|---|---|
| Endoscopic sphenopalatine artery ligation (ESPAL) | Posterior epistaxis failing packing; safe, effective, avoids posterior packing morbidity |
| Anterior/posterior ethmoidal artery ligation | Superior/posterior bleeds; endoscopic or transorbital approach |
| Internal maxillary artery ligation | In pterygopalatine fossa (endoscopic approach) |
| External carotid artery ligation | Above origin of lingual artery; last resort |
| Interventional radiology (embolisation) | Refractory epistaxis, nasopharyngeal carcinoma, tumours, carotid injury, facial trauma; pre-operative vascular control for juvenile angiofibroma |
STEP 9: Treat Underlying Cause
- Reverse anticoagulation if clinically appropriate (Vitamin K for warfarin, reversal agents for NOACs)
- Manage hypertension (does not directly cause epistaxis but worsens persistent bleeding)
- Correct coagulopathy, transfuse if Hb <7 g/dL
- Address thrombocytopenia
- Platelet transfusion if count critically low
6. Age-Wise Approach
Children (< 10 years) - Most Common Age Group
- Predominant cause: Nose picking, trauma, URTIs, low humidity, allergies
- Site: Anterior (Kiesselbach's plexus) in almost all cases
- Severity: Usually mild, self-limiting
- Special considerations:
- In children <2 years, epistaxis is rare - always consider non-accidental trauma (NAT) and bleeding disorders
- Exclude nasal foreign body (unilateral, foul-smelling discharge)
- Exclude juvenile angiofibroma in adolescent boys (unilateral progressive epistaxis, nasal obstruction - do NOT biopsy, pre-op embolisation required)
- HHT may first manifest in childhood
- Screen for haematologic malignancy (leukaemia) if associated bruising/pallor
- Management: First-aid pressure, oxymetazoline, silver nitrate cautery under local anaesthesia if source visible; nasal moisturisers for recurrence prevention
- Do NOT routinely perform bilateral septal cautery in children
Young Adults (10-35 years)
- Predominant causes: Trauma, nose picking, septal deviation, substance abuse (cocaine - septal perforation), sports injuries, iatrogenic (post-septal/nasal surgery)
- Site: Usually anterior
- Considerations:
- Cocaine use causes progressive septal destruction
- Screen for bleeding disorders (vWD especially in young females with recurrent epistaxis)
- Pregnancy-associated epistaxis (hormonal mucosal engorgement)
- HHT presenting with recurrent episodes
- Management: Cautery usually sufficient; address underlying cause
Middle-Aged Adults (35-60 years)
- Predominant causes: Hypertension, antiplatelet medications, septal pathology, rhinitis, chronic alcohol use
- Transition period where posterior epistaxis starts becoming more prevalent
- Considerations:
- Onset of posterior epistaxis; assess need for posterior packing
- Screen for systemic comorbidities
- Exclude sinonasal malignancy in unilateral presentations with nasal obstruction/facial pain
- Management: Address underlying hypertension and coagulopathy; chemical cautery or anterior packing usually sufficient; escalate if posterior bleed suspected
Elderly (> 60-70 years)
- Predominant causes: Hypertension, arteriosclerosis (vessel fragility), anticoagulants (warfarin, NOACs), antiplatelet agents, chronic liver/renal disease
- Site: Frequently posterior; arterial bleeds from sphenopalatine branches
- Severity: More severe, harder to control, higher recurrence and mortality (13.9% recurrence, 3.4% mortality at 30 days in UK nationwide study)
- Special considerations:
- Multiple comorbidities complicate management (anticoagulation, cardiac disease)
- Higher risk of aspiration, hypoxia from posterior packing
- Mucosal atrophy worsens fragility
- Altered anatomy from prior surgeries
- Monitor for cardiovascular complications during packing
- Management: Posterior packing more often required; earlier ENT involvement; consider endoscopic SPA ligation over prolonged posterior packing (better tolerated in elderly); reverse anticoagulation carefully with haematology input
7. Prevention and Discharge Advice
- Saline nasal spray or nasal moisturiser (petroleum jelly to nasal vestibule) - prevents mucosal drying
- Avoid nose picking; cut fingernails
- Use humidifier at home in winter
- Lean forward (not backward) during a nosebleed
- Apply firm digital pressure for 10-15 minutes without interruption
- Avoid hot drinks, alcohol, and strenuous activity for 24-48 hours post-episode
- Review anticoagulant/antiplatelet medications with prescribing physician
- Return to ED if bleeding recurs and does not stop with 20 minutes of pressure
References:
- Cummings Otolaryngology Head and Neck Surgery, Chapter 47 (Epistaxis)
- Rosen's Emergency Medicine, Chapter 58 (Epistaxis)
- Bailey & Love's Short Practice of Surgery, 28th Ed., Chapter 51
- Roberts and Hedges' Clinical Procedures in Emergency Medicine, Chapter 15
This is a shared conversation. Sign in to Orris to start your own chat.