An observational study to analyse Rasa , Meda and Asthi dhatu dushti in patients with Hypothyroidism
hypothyroidism AND "Ayurveda" AND dhatu
Rasa Meda Asthi dhatu dushti hypothyroidism Ayurveda observational study
https://jaims.in/jaims/article/download/1947/2230?inline=1
hypothyroidism AND Ayurveda AND "bone metabolism"
Asthi dhatu dushti hypothyroidism bone loss osteoporosis Ayurveda clinical study
hypothyroidism AND "bone mineral density" AND dyslipidemia
hypothyroidism AND dyslipidemia AND "bone mineral density"
Observational Study: Rasa, Meda and Asthi Dhatu Dushti in Hypothyroidism
Background and Conceptual Framework
- Rasa Dhatu (plasma/lymph/nutritional fluid)
- Meda Dhatu (adipose/fat tissue)
- Asthi Dhatu (bone tissue)
Ayurvedic Samprapti (Pathogenesis)
Nidana (Causative Factors)
| Type | Examples |
|---|---|
| Aharaja (dietary) | Abhishyandi (heavy, unctuous, cold foods), Guru Ahara, excessive Kapha-aggravating diet |
| Viharaja (lifestyle) | Sedentary lifestyle, Divasvapna (day sleep), Ati Sthaulya |
| Manasika | Chinta (stress), Shoka (grief), Bhaya (fear) - directly vitiate Rasavaha Srotas |
| Agantuja | Vegadharana (suppression of natural urges), Bharaharana |
Dosha Involvement
- Kapha Vriddhi - primary dosha (mirroring TSH-driven sluggishness, mucoid edema, weight gain)
- Vata Prakopa - secondary (causing dryness, constipation, bone depletion, neuromuscular symptoms)
- Pitta Kshaya - reduced metabolic fire (Agni mandya)
Agni Dushti
- Jataragni Mandya - reduced digestive fire at the gut level
- Dhatwagni Mandya - impaired tissue-level metabolism (particularly Rasa Dhatwagni, Meda Dhatwagni)
- This leads to Ama formation - the undigested metabolic byproduct that vitiates Srotas and Dhatus
1. Rasa Dhatu Dushti
Ayurvedic Concept
- Hrillasa (nausea/palpitations)
- Aruchi (loss of appetite/taste)
- Asya Vairasya
- Gaurava (heaviness)
- Tandra (drowsiness, fatigue)
- Alasya (lethargy)
- Pandu (pallor/anemia)
- Agnisada (digestive impairment)
- Sroto Avarodha (channel obstruction)
Correlation with Hypothyroidism
| Hypothyroid Feature | Rasa Dhatu Dushti Equivalent |
|---|---|
| Fatigue, lethargy | Alasya, Tandra |
| Facial/peripheral puffiness (myxedema) | Shotha (edema from Rasa Sroto dushti) |
| Pallor, anemia | Pandu (Rasa-Rakta Dushti) |
| Loss of appetite | Aruchi, Agnisada |
| Cold intolerance | Sheeta Lakshana from Kapha-dominant Rasa |
| Dry skin | Twak Parushyata (Heena Rasa nourishing Twak) |
| Bradycardia | Hrillasa/Hridaya-related Rasa Dushti |
2. Meda Dhatu Dushti
Ayurvedic Concept
- Sthaulya (obesity/overweight)
- Udara Vriddhi (abdominal enlargement)
- Shramena Shwasa (exertional dyspnea)
- Atisvedana (excessive sweating) OR Swedabhava (absent sweating)
- Snigdha Twak (oily skin)
- Durgandha (body odor from ama-laden Meda)
- Daurbalya (weakness despite apparent bulk)
- Medavaha Sroto Dushti
- Kshama (emaciation in severe cases)
- Pleeha/Granthi (swellings from Meda stagnation)
Correlation with Hypothyroidism
| Hypothyroid Feature | Meda Dhatu Dushti Equivalent |
|---|---|
| Weight gain / obesity | Sthaulya (Meda Vriddhi) |
| Dyslipidemia (elevated LDL, triglycerides) | Meda Dushti/ama in Medovaha Srotas |
| Pericardial effusion | Meda accumulation in Hridaya region |
| Fatty liver (NAFLD in hypothyroid) | Yaka-ashrita Meda Dushti |
| Metabolic syndrome | Sroto Avarodha from Ama+Meda |
| Non-pitting edema | Meda + Kapha accumulation in Twak |
3. Asthi Dhatu Dushti
Ayurvedic Concept
- Asthishula (bone pain)
- Asthisphotana (crackling of joints)
- Kesha-Nakha Bhanga (hair fall, brittle nails)
- Danta Bhanjana (dental decay/loosening)
- Sandhi Shaithilya (joint laxity)
- Asthi Daurbalya (bone fragility)
- Asthisaushirya (porosity/osteopenia)
- Adhidanta, Atidanta (dental abnormalities)
- Keshatimatra (excess hair growth as Asthi Vriddhi sign)
Correlation with Hypothyroidism
| Hypothyroid Feature | Asthi Dhatu Dushti Equivalent |
|---|---|
| Reduced bone turnover, osteopenia | Asthi Kshaya / Asthisaushirya |
| Joint stiffness, arthralgia | Asthishula, Sandhi Shotha |
| Brittle nails, hair fall | Asthi Mala Kshaya (Kesha-Nakha are Mala of Asthi) |
| Carpal tunnel syndrome | Majja Dushti secondary to Asthi Dushti |
| Delayed fracture healing | Asthi Daurbalya |
| Low BMD (especially prolonged hypothyroidism) | Asthisaushirya |
Meda Dhatwagni Mandya → impaired Meda → reduced substrate for Asthi formation → Asthi Dhatu Kshaya
Proposed Samprapti (Pathogenesis Flow)
Nidana (diet/lifestyle/stress)
↓
Jataragni Mandya + Kapha Vriddhi
↓
Ama formation → Rasavaha Srotas Dushti
↓
Rasa Dhatu Dushti (Sama Rasa - qualitatively poor)
↓
Rasa Dhatwagni Mandya → Rakta Dhatu Dushti (pallor)
↓
Mamsa Dhatu → Meda Dhatwagni Mandya
↓
Meda Vriddhi + Medovaha Sroto Dushti (Sanga type)
↓
Impaired substrate for Asthi formation
↓
Asthi Dhatu Kshaya / Dushti + Vata Prakopa
↓
Majja Dhatu affected (Sandhi symptoms, neurological features)
Study Design Recommendations
Inclusion Criteria
- Age 18-60 years, either sex
- Diagnosed hypothyroidism (TSH >5.0 mIU/L, low/normal T4)
- Primary hypothyroidism (autoimmune/idiopathic)
- Written informed consent
Exclusion Criteria
- Secondary/central hypothyroidism
- Graves' disease or hyperthyroidism
- Active malignancy, pregnancy
- Known metabolic bone disease, corticosteroid use
- Patients on thyroid hormone replacement for <6 months
Assessment Parameters
- Clinical: Fatigue (VAS), pallor, edema grading, cold intolerance
- Lab: Hemoglobin, serum albumin, serum protein
- Scoring: Rasa Dhatu Dushti Lakshana checklist (Charaka criteria)
- Clinical: BMI, waist circumference, skin fold thickness
- Lab: Fasting lipid profile (LDL, HDL, triglycerides, total cholesterol)
- USG: Fatty liver grading (Medovaha Sroto Dushti)
- Scoring: Meda Dushti Lakshana scale
- Clinical: Bone pain (NRS), hair fall (Sinclair scale), nail brittleness, joint crepitus
- Lab: Serum calcium, phosphorus, alkaline phosphatase, Vitamin D, PTH, serum osteocalcin
- Imaging: DEXA scan (BMD T-score and Z-score) for Asthisaushirya
- Scoring: Asthi Kshaya Lakshana checklist
Statistical Analysis
- Descriptive statistics (mean, SD, frequency, percentage)
- Pearson/Spearman correlation between TSH levels and Dhatu Dushti scores
- Chi-square test for categorical parameters
- ANOVA/Kruskal-Wallis for group comparisons
Published Evidence Summary
| Dhatu | Involvement |
|---|---|
| Meda | 78.2% (most frequent) |
| Rasa | 43.0% |
| Majja | 31.6% |
| Mamsa | 18.5% |
| Rakta | 5.5% |
- Kapha and Vata are the primary Doshas in Samprapti
- Dhatwagnimandya (especially Meda and Rasa Dhatwagni) is the core mechanism
- Sanga type of Srotodushti is the predominant form
- Udbhava Sthana: Amashaya; Vyakta Sthana: Sarva Shareera
Why Asthi Dhatu Must Be Included
- Sequential formation logic: Meda Dushti (most common in hypothyroidism) directly impairs Asthi formation via Medo Dhatwagni Mandya.
- Hypothyroid bone disease: Even subclinical hypothyroidism is associated with reduced bone turnover and increased fracture risk in long-term studies.
- Vata-Asthi relationship: Hypothyroidism causes secondary Vata Prakopa (via Kapha Avarana), and Vata aggravation depletes Asthi Dhatu.
- Asthi Mala markers: Hair fall and nail brittleness - common in hypothyroidism - are classical Asthi Dhatu Mala manifestations (Kesha and Nakha).
- Unmet research gap: Unlike Rasa and Meda, Asthi Dhatu Dushti in hypothyroidism has not been systematically quantified in published Ayurvedic observational studies.
for the above given topic of thesis give me literature review in terms of :functional anatomy of thyroid gland , Physiology of thyroid gland , causes , clinical features , investigations of Hypothyroidism and rasa dhatu ,medo dhatu and asthi dhatu vruddhi and kshaya lakshanas with interpretation
Rasa dhatu Meda dhatu Asthi dhatu vriddhi kshaya lakshanas classical Ayurveda Charaka Sushruta
https://www.ijfmr.com/papers/2023/5/7478.pdf
hypothyroidism AND "lipid metabolism" AND "bone mineral density"
Meda dhatu vriddhi kshaya lakshanas Charaka Samhita Sushruta classical text interpretation
LITERATURE REVIEW
Thesis Title: An Observational Study to Analyse Rasa, Meda and Asthi Dhatu Dushti in Patients with Hypothyroidism
PART A: MODERN REVIEW
I. FUNCTIONAL ANATOMY OF THE THYROID GLAND
1.1 Gross Anatomy
- Superior thyroid artery (from external carotid artery)
- Inferior thyroid artery (from thyrocervical trunk of subclavian artery)
- Venous drainage via superior, middle, and inferior thyroid veins into the internal jugular and brachiocephalic veins
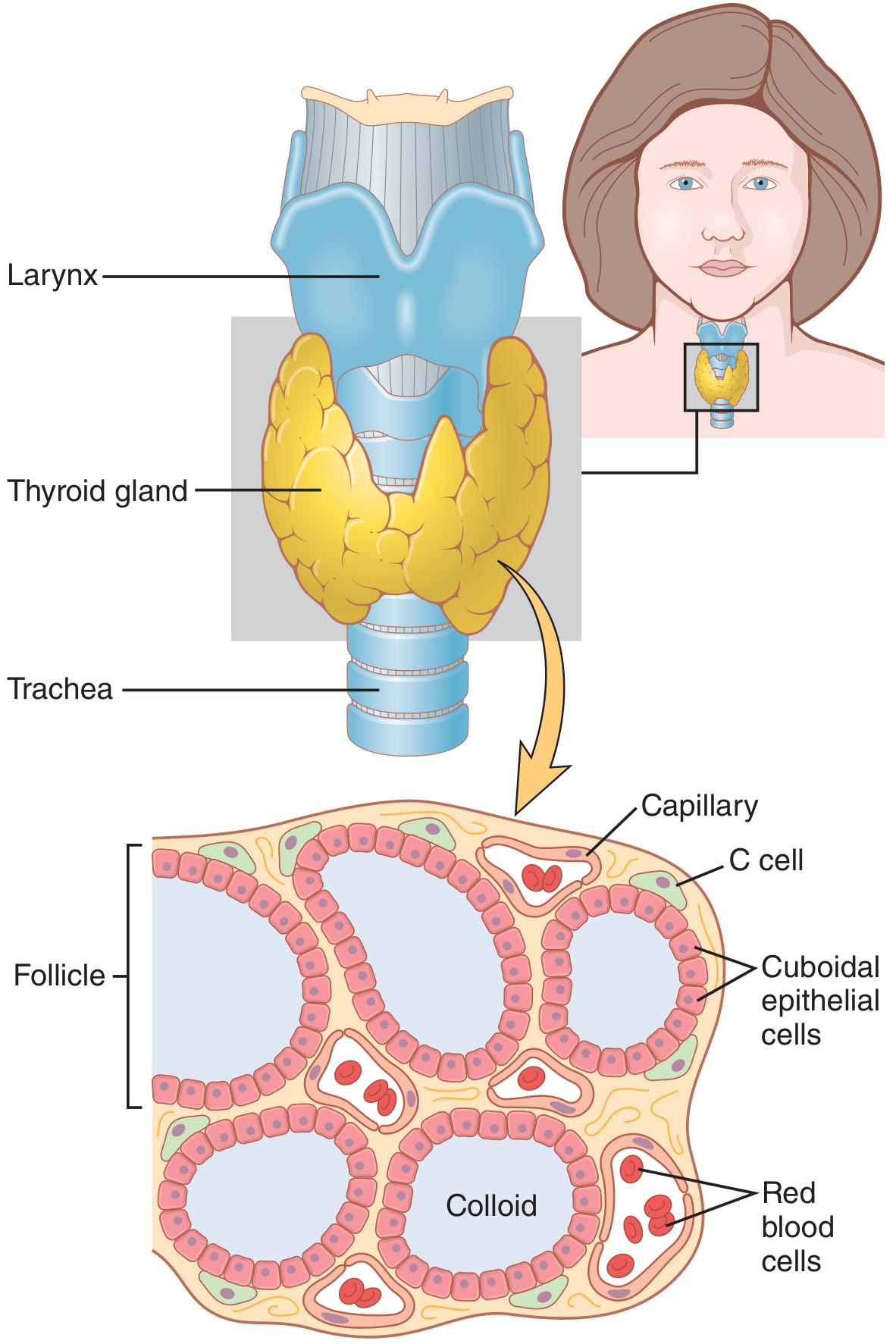
1.2 Microscopic Anatomy
| Cell Type | Location | Function |
|---|---|---|
| Follicular (thyrocyte) cells | Follicle lining | Synthesis and secretion of T3 and T4 |
| Parafollicular (C cells) | Between follicles | Secretion of calcitonin - regulates plasma calcium |
II. PHYSIOLOGY OF THE THYROID GLAND
2.1 Thyroid Hormone Synthesis
- MIT (Monoiodotyrosine) - one iodine
- DIT (Diiodotyrosine) - two iodines
2.2 Transport in Blood
- 99.97% of T4 and 99.7% of T3 in the plasma are protein-bound
- Binding proteins: Thyroxine-binding globulin (TBG) (major carrier), thyroxine-binding prealbumin (transthyretin), and albumin
- Only the free (unbound) fraction is biologically active
2.3 Mechanism of Action of Thyroid Hormones
- T4 is deiodinated to T3
- T3 binds to thyroid hormone receptors (THR) - nuclear transcription factors bound to thyroid hormone response elements (TRE) on DNA, usually as a heterodimer with retinoid X receptor (RXR)
- T3-THR complex activates gene transcription → formation of mRNA → new intracellular proteins → altered cellular function
- Metabolism: Increase basal metabolic rate, calorigenic effect, increase carbohydrate and fat catabolism
- Growth: Essential for normal bone and brain development
- Cardiovascular: Increase heart rate, cardiac contractility, and cardiac output
- CNS: Required for normal brain maturation in fetus; cognitive function in adults
- Lipid metabolism: Upregulate LDL receptors → reduce total cholesterol and LDL-C
- Muscle: Increase contractility, regulate sarcolemmal gene expression
- Bone: Regulate bone remodeling - both osteoblast and osteoclast activity
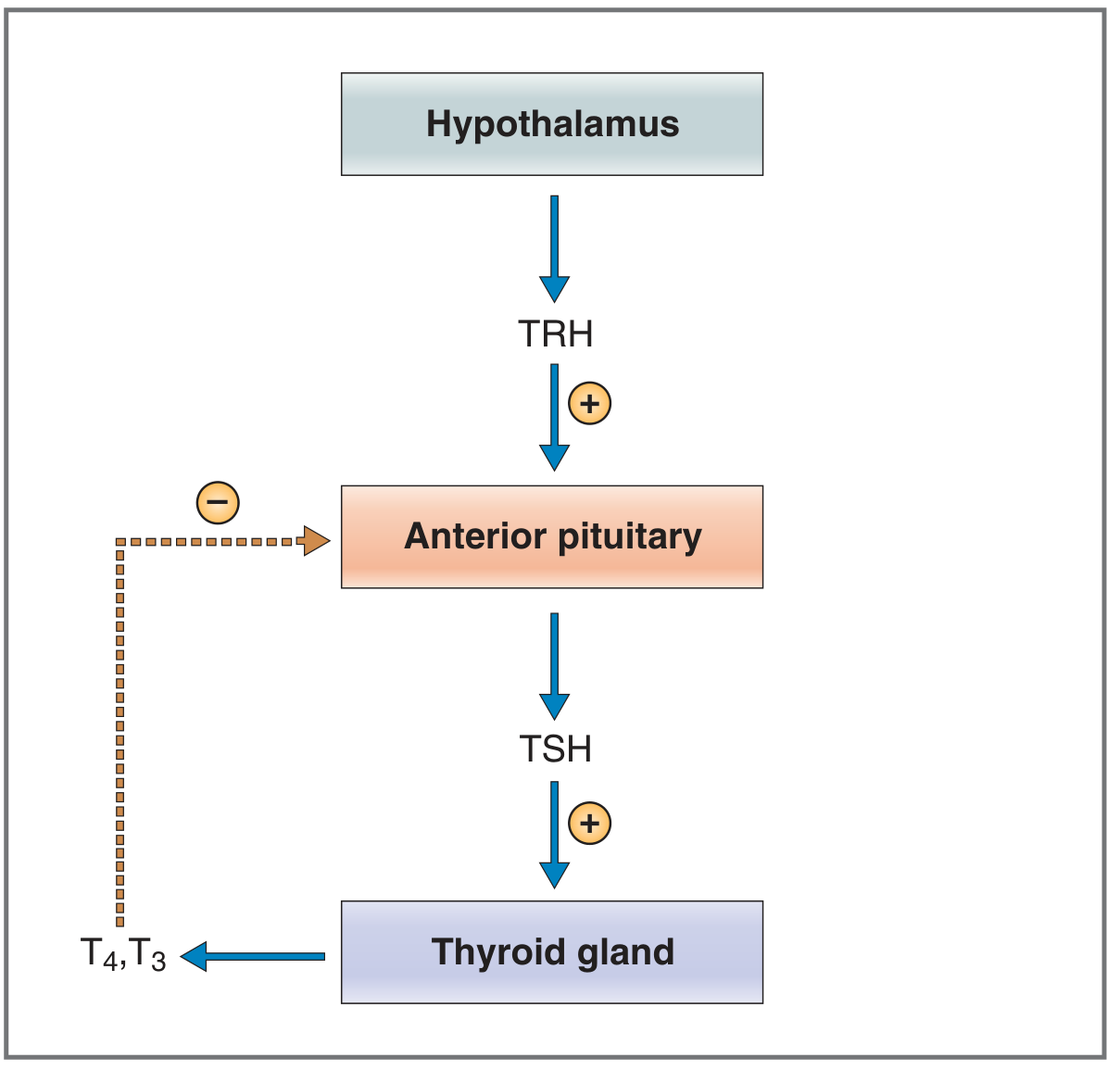
2.4 Regulation of Thyroid Hormone Secretion (HPT Axis)
-
TRH (Thyrotropin-Releasing Hormone): Secreted by paraventricular nuclei of hypothalamus. A tripeptide that acts on thyrotrophs of anterior pituitary to stimulate TSH gene transcription and TSH secretion.
-
TSH (Thyroid-Stimulating Hormone): Glycoprotein secreted by anterior pituitary thyrotrophs. Exerts a trophic effect (growth stimulus) on the thyroid and stimulates all steps of hormone synthesis and secretion - iodide trapping, thyroglobulin synthesis, TPO activity, endocytosis of colloid, and hormone release.
-
Negative Feedback: Free T3 (converted from T4 by pituitary deiodinase) down-regulates TRH receptors on thyrotrophs, reducing TSH secretion. This feedback loop maintains steady-state thyroid hormone levels.
- Iodine deficiency or excess (Wolff-Chaikoff effect)
- Propylthiouracil (inhibits TPO)
- Perchlorate/thiocyanate (inhibits NIS)
- Lithium, amiodarone
- Decreased TBG (liver disease)
III. HYPOTHYROIDISM
3.1 Definition
- Primary hypothyroidism: Failure of the thyroid gland itself (elevated TSH, low T4/T3) - most common (>95% of cases)
- Secondary hypothyroidism: Failure of TSH secretion from pituitary (low TSH, low T4)
- Tertiary hypothyroidism: Failure of TRH secretion from hypothalamus
- Overt hypothyroidism: TSH elevated (>20 mIU/L) with low free T4 and symptomatic disease
- Subclinical hypothyroidism: Elevated TSH (4.5-20 mIU/L) with normal free T4 - often asymptomatic
3.2 Causes of Hypothyroidism
| Category | Specific Causes |
|---|---|
| Autoimmune | Hashimoto's thyroiditis (most common in iodine-sufficient regions), Atrophic thyroiditis |
| Iatrogenic | Radioiodine (¹³¹I) therapy, thyroidectomy (subtotal/total), external neck irradiation |
| Drugs | Iodine excess (contrast media, amiodarone), lithium, antithyroid drugs (PTU, carbimazole), interferon-α, immune checkpoint inhibitors (ipilimumab, nivolumab, pembrolizumab), tyrosine kinase inhibitors (sunitinib) |
| Nutritional | Iodine deficiency (most common worldwide), selenium deficiency |
| Congenital | Thyroid agenesis/ectopia (65%), dyshormonogenesis (30%), TSH-R mutation (5%) |
| Infiltrative | Amyloidosis, sarcoidosis, hemochromatosis, scleroderma, Riedel's thyroiditis |
- Silent/postpartum thyroiditis
- Subacute (de Quervain's) thyroiditis
- After thyroidectomy/radioiodine for Graves' disease
- Pituitary disease (adenoma, surgery, Sheehan's syndrome)
- Hypothalamic tumors, trauma, infiltrative disorders, Prader-Willi syndrome
- Isolated TSH deficiency (rare)
- Drugs: bexarotene, mitotane
3.3 Clinical Features of Hypothyroidism
- Fatigue, lethargy, weakness
- Cold intolerance (due to reduced thermogenesis)
- Weight gain (despite poor appetite - mainly fluid retention)
- Hoarse, deep voice
- Dry, rough, cool, pale skin (decreased blood flow)
- Non-pitting edema / myxedema (glycosaminoglycan accumulation)
- Puffy face with periorbital edema
- Hair: Dry, brittle, thinning, diffuse alopecia; loss of outer-third eyebrows
- Nails: Retarded growth, brittle
- Yellow tinge (carotene accumulation)
- Bradycardia
- Reduced cardiac output, stroke volume
- Diastolic hypertension (increased peripheral resistance)
- Pericardial effusion (in up to 30% of patients)
- Dyslipidemia: Elevated total cholesterol, LDL-C, triglycerides - proatherogenic
- Mental slowness, cognitive impairment, depression
- Proximal muscle weakness
- Delayed deep tendon reflex relaxation (classic sign)
- Carpal tunnel syndrome, paresthesias
- Cerebellar ataxia (in severe cases)
- Constipation
- Decreased appetite
- Decreased libido
- Oligomenorrhea or amenorrhea (long-standing disease), or menorrhagia (early stage)
- Reduced fertility, increased miscarriage risk
- Hyperprolactinemia (galactorrhea)
- Hypercholesterolemia, hypertriglyceridemia (Meda Dushti analog)
- Hyponatremia (in severe cases)
- Reduced bone turnover (both osteoblast and osteoclast activity suppressed)
- Reduced BMD in severe or prolonged hypothyroidism
- Joint effusions, arthralgia
- Carpal tunnel compression
3.4 Investigations of Hypothyroidism
| Test | Interpretation |
|---|---|
| Serum TSH | Most sensitive test. Elevated (>4.5 mIU/L) in primary hypothyroidism. Normal or low in secondary hypothyroidism |
| Free T4 (FT4) | Decreased in overt hypothyroidism. Normal in subclinical hypothyroidism. Directly measures active hormone |
| Free T3 (FT3) | Usually decreased; helps assess severity |
- Overt hypothyroidism: TSH >20 mIU/L + low FT4 + symptoms
- Subclinical hypothyroidism: TSH 4.5-20 mIU/L + normal FT4
- Anti-TPO antibodies (anti-thyroid peroxidase): Elevated in 95% of Hashimoto's thyroiditis - confirms autoimmune etiology
- Anti-thyroglobulin antibodies: Elevated in ~60% of Hashimoto's
- TSH receptor antibodies (TRAb/TSI): To distinguish from Graves' disease and identify blocking antibodies
- Thyroid ultrasound: Assesses gland size, echogenicity (heterogeneous/hypoechoic in Hashimoto's), nodules
- Thyroid scan (¹²³I or ⁹⁹ᵐTc): Assesses functional status, ectopic tissue
| Parameter | What It Reflects |
|---|---|
| CBC with peripheral smear | Anemia (Rasa-Rakta Dushti) |
| Serum albumin, total protein | Rasa Dhatu quality |
| Fasting lipid profile (LDL, HDL, TG, TC) | Meda Dhatu Dushti |
| Blood glucose / insulin resistance | Meda-Medovaha Sroto Dushti |
| Serum calcium, phosphorus, ALP | Asthi Dhatu status |
| Vitamin D (25-OH D3), PTH | Asthi Dhatwagni function |
| Serum osteocalcin, bone-specific ALP | Bone formation markers |
| DEXA scan (T-score, Z-score) | Quantitative Asthi Kshaya |
| Liver function tests | Hepatic Meda accumulation |
| ECG | Cardiovascular effects of Rasa Dushti |
| Serum CK, LDH | Muscle involvement (Mamsa Dushti) |
PART B: AYURVEDIC REVIEW
IV. RASA DHATU - VRIDDHI AND KSHAYA LAKSHANAS WITH INTERPRETATION
4.1 Introduction to Rasa Dhatu
- Preetih - provides satisfaction and contentment to the mind and body
- Tarpana - nourishes all other Dhatus sequentially
- Jivana - sustains life
4.2 Rasa Dhatu Kshaya (Depletion) - Lakshanas
| Sanskrit Term | English Meaning | Modern Correlation in Hypothyroidism |
|---|---|---|
| Hridrava | Palpitations, cardiac pain | Reflects impaired cardiac nourishment by Rasa |
| Sahate Shabdam Na | Intolerance to loud noises | Neurosensory depletion |
| Ghattate | Restlessness, anxiety | CNS under-nourishment |
| Hridayam Tamyati | Cardiac fatigue even with minimal exertion | Reduced cardiac output in hypothyroidism |
| Shrama (Alpacheshtasyapi) | Fatigue even with minimal activity | Classic hypothyroid fatigue |
| Ruksha Twak | Dry skin | Reduced plasma fluids nourishing skin |
| Pandu | Pallor, anemia | Reduced Rakta formation from deficient Rasa |
| Daurbalya | General weakness | Systemic nutritional deficiency |
4.3 Rasa Dhatu Vriddhi (Excess) - Lakshanas
| Sanskrit Term | English Meaning | Modern Correlation in Hypothyroidism |
|---|---|---|
| Agnisadana | Impaired digestion, poor appetite | Hypothyroid gut dysmotility |
| Praseka | Excessive salivation | Mucosal edema |
| Alasya | Sluggishness, lethargy | Classic hypothyroid feature |
| Gaurava | Heaviness of the body | Myxedema, weight gain |
| Shvaithya | Pallor, white discoloration of skin | Skin changes in hypothyroidism |
| Shaithya | Coldness (of body parts) | Cold intolerance in hypothyroidism |
| Shlathangatva | Looseness of body parts, flaccidity | Muscle weakness |
| Shwasa | Dyspnea, breathlessness | Pleural effusion, myopathy |
| Kasa | Cough | Myxedematous pharyngeal edema |
| Atinidrata | Excessive sleep, hypersomnia | Classic hypothyroid symptom |
V. MEDA DHATU - VRIDDHI AND KSHAYA LAKSHANAS WITH INTERPRETATION
5.1 Introduction to Meda Dhatu
- Sneha - provides unctuousness (oleation) to all body parts
- Svedana - governs perspiration
- Dridhatva - gives firmness and compactness to the body
- Balya - nourishes Asthi Dhatu (the next in sequence)
5.2 Meda Dhatu Kshaya (Depletion) - Lakshanas
| Sanskrit Term | English Meaning | Modern Correlation |
|---|---|---|
| Sphik, Udara, Stana Shushkata | Emaciation of buttocks, abdomen, breasts | Loss of subcutaneous fat |
| Parvakam Graha | Crackling/stiffness of small joints | Joint degeneration due to lack of synovial lubrication |
| Shrama | Fatigue, exhaustion | Metabolic depletion |
| Atishrama | Excessive fatigue even with light activity | Reduced energy reserves |
| Shosha | Emaciation | Severe wasting |
| Pleeha Vriddhi | Splenomegaly | Lymphoid hyperplasia |
5.3 Meda Dhatu Vriddhi (Excess) - Lakshanas
| Sanskrit Term | English Meaning | Modern Correlation in Hypothyroidism |
|---|---|---|
| Sthoulya | Obesity, overweight | Weight gain due to reduced lipolysis |
| Udara Vriddhi | Abdominal enlargement | Central adiposity |
| Shramena Shwasa | Exertional dyspnea | Obesity-related breathlessness |
| Kshudra Shwasa | Dyspnea on mild exertion | |
| Atisvedana | Excessive sweating | (Or conversely, reduced sweating in hypothyroid) |
| Daurgandhya | Foul body odor | Ama-mixed Meda |
| Daurbalya | Weakness | Despite apparent bulk |
| Medavaha Sroto Dushti | Obstruction in fat-carrying channels | Dyslipidemia (elevated LDL, TG) |
| Yaka-ashrita Meda | Fat accumulation in liver | Non-alcoholic fatty liver (NAFLD) |
| Kandu | Itching | Skin changes from Meda Dushti |
"Thyroid dysfunction is well established as a modifiable factor in dyslipidemia, with a direct, linear relationship observed between increasing TSH levels and total cholesterol, LDL-C, and triglycerides. Thyroid hormones, particularly T3, upregulate LDL receptors."
- Fitzpatrick's Dermatology, Vol. 1
VI. ASTHI DHATU - VRIDDHI AND KSHAYA LAKSHANAS WITH INTERPRETATION
6.1 Introduction to Asthi Dhatu
- Deha Dharana - provides structural support and framework to the body
- Mamsadhara - supports muscle tissue
- Protection of vital organs (brain, heart, lungs)
- Enables movement via Sandhi (joints)
6.2 Asthi Dhatu Kshaya (Depletion) - Lakshanas
| Sanskrit Term | English Meaning | Modern Correlation in Hypothyroidism |
|---|---|---|
| Kesha Patana | Hair fall, scalp hair loss | Hair loss is a cardinal symptom of hypothyroidism |
| Loma Patana | Loss of body hair | |
| Nakha Patana/Bhanga | Brittle nails, nail loss | Brittle, slow-growing nails in hypothyroidism |
| Shmashru Patana | Loss of beard/facial hair | |
| Dvija Patana (Danta Bhanjana) | Tooth loss, dental fragility | |
| Asthishula | Bone pain, aching | Arthralgia and musculoskeletal pain |
| Asthisphotana | Crackling of bones/joints | Crepitus in hypothyroid arthropathy |
| Sandhi Shaithilya | Joint laxity, looseness | Ligamentous laxity in hypothyroid myxedema |
| Shrama | Fatigue | Systemic |
| Asthi Daurbalya | Bone fragility | Osteopenia/osteoporosis in prolonged hypothyroidism |
- Hair follicle cycling is regulated by thyroid hormones; hypothyroidism causes telogen effluvium and diffuse alopecia
- Nail growth depends on matrix cell proliferation driven by thyroid hormones; hypothyroidism produces brittle, ridged, slow-growing nails
- Both are widely recognized clinical features of hypothyroidism
- Bone turnover is reduced (both formation and resorption are slowed)
- In prolonged hypothyroidism, net bone mass decreases
- In subclinical hypothyroidism, BMD may be subtly reduced, especially in trabecular bone
- Hypothyroid myxedema can cause joint effusions resembling Sandhi Shotha
- Carpal tunnel syndrome (a recognized hypothyroid complication) corresponds to Asthi-Majja Dushti affecting the wrist canal
6.3 Asthi Dhatu Vriddhi (Excess) - Lakshanas
| Sanskrit Term | English Meaning | Modern Correlation |
|---|---|---|
| Adhyasthi | Extra bone development/calcification (exostosis) | Periosteal new bone, heterotopic ossification |
| Adhidanta | Extra teeth (hyperdontia), calcified dental structures | Dental calcification |
| Keshatimatra | Excessive hair growth | Hirsutism (not typically hypothyroid) |
VII. INTERCONNECTION: DHATU POSHANA KRAMA AND HYPOTHYROIDISM
Hypothyroidism → Jataragni/Dhatwagni Mandya
↓
Impaired Ahara Paka → Ama formation
↓
RASA DHATU DUSHTI (Sama Rasa - poor quality)
[Lakshanas: Gaurava, Alasya, Shaithya, Atinidrata, Shwasa]
↓
Impaired nourishment of Mamsa Dhatu
↓
MEDA DHATWAGNI MANDYA → MEDA VRIDDHI + MEDA DUSHTI
[Lakshanas: Sthoulya, Medovaha Sroto Dushti, Daurgandhya]
↓
Impaired Meda → Reduced substrate for Asthi formation
↓
ASTHI DHATU KSHAYA
[Lakshanas: Kesha/Nakha Patana, Asthishula, Sandhi Shaithilya, BMD ↓]
- Meda Dhatu Dushti: 78.2% (most frequent)
- Rasa Dhatu Dushti: 43%
- Majja Dhatu: 31.6%
- Mamsa Dhatu: 18.5%
SUMMARY TABLE: Dhatu Lakshanas in Hypothyroidism
| Dhatu | Lakshana (Ayurvedic) | Clinical Feature (Modern) | Lab/Investigation |
|---|---|---|---|
| Rasa Kshaya/Dushti | Hridrava, Pandu, Alasya, Gaurava, Shaithya | Fatigue, pallor, cold intolerance, edema | Low Hb, low albumin |
| Rasa Vriddhi | Atinidrata, Shvaithya, Shlathangatva, Shwasa | Excessive sleep, pallor, flaccidity | TSH elevated, bradycardia |
| Meda Vriddhi/Dushti | Sthoulya, Shrama, Medovaha Sroto Dushti | Weight gain, dyslipidemia, NAFLD | Elevated LDL, TG, TC; USG liver |
| Meda Kshaya | Sphik-Udara Shushkata, Atishrama | Emaciation (severe cases) | Low BMI (rare) |
| Asthi Kshaya | Kesha/Nakha Patana, Asthishula, Sandhi Shaithilya | Hair fall, brittle nails, bone pain, joint laxity | Low DEXA T-score, low Vit D, high PTH |
| Asthi Vriddhi | Adhyasthi, Adhidanta | Calcification (not typical in hypothyroid) | X-ray |
- Guyton and Hall Textbook of Medical Physiology (14th Ed.)
- Costanzo Physiology (7th Ed.)
- Harrison's Principles of Internal Medicine (22nd Ed., 2025)
- Robbins, Cotran & Kumar Pathologic Basis of Disease (10th Ed.)
- Charaka Samhita - Sutra Sthana 17 (Dhatu Kshaya-Vriddhi), Vimana Sthana 5 & 8
- Sushruta Samhita - Sutra Sthana 14
- Ashtanga Hridayam - Sutra Sthana 11
- JAIMS Observational study on Samprapti Ghatakas in hypothyroidism (n=100)
- Fitzpatrick's Dermatology (Vol. 1) - on thyroid and dyslipidemia
- IJFMR - A Physiological Review on Dhatu Kshaya Vriddhi in Ayurveda (2023)
Generate a presentation summarizing the literature review framework
ls /home/daytona/workspace/ 2>/dev/null || echo "workspace empty or not found"
mkdir -p /home/daytona/workspace/hypothyroid-pptx
~/hypothyroid-pptx/build.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "Rasa, Meda & Asthi Dhatu Dushti in Hypothyroidism";
pres.author = "Literature Review Presentation";
// ─── COLOUR PALETTE ───────────────────────────────────────────────────────
const C = {
darkBg: "0D1B2A", // deep navy – title / section dividers
midBg: "1B3A4B", // teal-navy – accent bg
accent1: "E8A838", // warm amber – primary accent / highlights
accent2: "5BB8D4", // sky teal – secondary accent
ayur: "2E7D32", // deep green – Ayurvedic slides
ayurLight: "E8F5E9", // pale green – Ayurvedic card bg
white: "FFFFFF",
offWhite: "F4F6F8",
lightGray: "E0E6EC",
textDark: "0D1B2A",
textGray: "4A5568",
rasaCol: "1565C0", // blue – Rasa
medaCol: "6A1B9A", // purple – Meda
asthiCol: "BF360C", // burnt orange – Asthi
};
// ─── HELPER: section divider ──────────────────────────────────────────────
function sectionDivider(pres, label, sub, colorBg) {
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: colorBg }, line: { type: "none" } });
// accent bar
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 2.5, w: 0.12, h: 0.8, fill: { color: C.accent1 }, line: { type: "none" } });
s.addText(label, { x: 0.35, y: 2.35, w: 9, h: 0.7, fontSize: 30, bold: true, color: C.white, fontFace: "Calibri", margin: 0 });
if (sub) s.addText(sub, { x: 0.35, y: 3.1, w: 9, h: 0.5, fontSize: 14, color: C.accent1, fontFace: "Calibri", margin: 0 });
}
// ─── HELPER: card box ─────────────────────────────────────────────────────
function card(slide, pres, x, y, w, h, title, body, accentColor) {
slide.addShape(pres.shapes.RECTANGLE, { x, y, w, h, fill: { color: C.white }, line: { color: C.lightGray, pt: 1 }, shadow: { type: "outer", color: "000000", blur: 8, offset: 3, angle: 135, opacity: 0.1 } });
slide.addShape(pres.shapes.RECTANGLE, { x, y, w, h: 0.08, fill: { color: accentColor }, line: { type: "none" } });
slide.addText(title, { x: x + 0.15, y: y + 0.12, w: w - 0.3, h: 0.38, fontSize: 11, bold: true, color: accentColor, fontFace: "Calibri", margin: 0 });
slide.addText(body, { x: x + 0.15, y: y + 0.52, w: w - 0.3, h: h - 0.65, fontSize: 9.5, color: C.textDark, fontFace: "Calibri", valign: "top", margin: 0 });
}
// ─────────────────────────────────────────────────────────────────────────
// SLIDE 1 – TITLE
// ─────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
// full dark bg
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.darkBg }, line: { type: "none" } });
// amber band top
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.18, fill: { color: C.accent1 }, line: { type: "none" } });
// amber band bottom
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 5.45, w: 10, h: 0.18, fill: { color: C.accent1 }, line: { type: "none" } });
// teal side accent
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0.18, w: 0.45, h: 5.27, fill: { color: C.midBg }, line: { type: "none" } });
s.addText("LITERATURE REVIEW", { x: 0.7, y: 0.7, w: 9, h: 0.45, fontSize: 13, bold: true, color: C.accent1, charSpacing: 5, fontFace: "Calibri", margin: 0 });
s.addText("Rasa, Meda & Asthi Dhatu Dushti\nin Hypothyroidism", {
x: 0.7, y: 1.25, w: 8.8, h: 1.7, fontSize: 30, bold: true, color: C.white, fontFace: "Calibri", margin: 0
});
s.addShape(pres.shapes.RECTANGLE, { x: 0.7, y: 3.05, w: 2.8, h: 0.05, fill: { color: C.accent2 }, line: { type: "none" } });
s.addText("An Observational Study Framework", { x: 0.7, y: 3.2, w: 9, h: 0.4, fontSize: 13, color: C.accent2, fontFace: "Calibri", italic: true, margin: 0 });
s.addText("Dept. of Kayachikitsa / Kriya Shareera · Ayurveda College", { x: 0.7, y: 4.0, w: 9, h: 0.35, fontSize: 11, color: "8899AA", fontFace: "Calibri", margin: 0 });
s.addText("2026", { x: 0.7, y: 4.4, w: 2, h: 0.35, fontSize: 11, color: "8899AA", fontFace: "Calibri", margin: 0 });
}
// ─────────────────────────────────────────────────────────────────────────
// SLIDE 2 – OVERVIEW / OUTLINE
// ─────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offWhite }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.72, fill: { color: C.darkBg }, line: { type: "none" } });
s.addText("PRESENTATION OVERVIEW", { x: 0.4, y: 0.15, w: 9, h: 0.42, fontSize: 18, bold: true, color: C.white, fontFace: "Calibri", margin: 0 });
const sections = [
["01", "Functional Anatomy\nof Thyroid Gland", C.accent2],
["02", "Physiology of\nThyroid Gland", C.accent1],
["03", "Hypothyroidism –\nCauses, Features,\nInvestigations", "E53935"],
["04", "Rasa Dhatu –\nVriddhi & Kshaya\nLakshanas", C.rasaCol],
["05", "Medo Dhatu –\nVriddhi & Kshaya\nLakshanas", C.medaCol],
["06", "Asthi Dhatu –\nVriddhi & Kshaya\nLakshanas", C.asthiCol],
["07", "Dhatu Dushti &\nHypothyroidism –\nCorrelation", C.ayur],
];
const cols = [0.25, 1.7, 3.15, 4.6, 6.05, 7.5, 8.95];
sections.forEach(([num, title, col], i) => {
const x = cols[i];
s.addShape(pres.shapes.RECTANGLE, { x, y: 0.9, w: 1.35, h: 4.55, fill: { color: col }, line: { type: "none" } });
s.addText(num, { x, y: 0.95, w: 1.35, h: 0.5, fontSize: 22, bold: true, color: "FFFFFF", align: "center", fontFace: "Calibri", margin: 0 });
s.addText(title, { x: x + 0.07, y: 1.55, w: 1.21, h: 3.8, fontSize: 11, color: "FFFFFF", align: "center", fontFace: "Calibri", valign: "top", margin: 0 });
});
}
// ─────────────────────────────────────────────────────────────────────────
// SECTION DIVIDER – ANATOMY
// ─────────────────────────────────────────────────────────────────────────
sectionDivider(pres, "PART A: MODERN REVIEW", "Functional Anatomy · Physiology · Hypothyroidism", C.midBg);
// ─────────────────────────────────────────────────────────────────────────
// SLIDE 4 – FUNCTIONAL ANATOMY
// ─────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offWhite }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.72, fill: { color: C.midBg }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0.72, w: 10, h: 0.06, fill: { color: C.accent2 }, line: { type: "none" } });
s.addText("01 FUNCTIONAL ANATOMY OF THE THYROID GLAND", { x: 0.3, y: 0.15, w: 9.4, h: 0.42, fontSize: 14, bold: true, color: C.white, fontFace: "Calibri", margin: 0 });
// Gross anatomy card
s.addShape(pres.shapes.RECTANGLE, { x: 0.2, y: 0.95, w: 4.5, h: 2.35, fill: { color: C.white }, line: { color: C.lightGray, pt: 1 } });
s.addShape(pres.shapes.RECTANGLE, { x: 0.2, y: 0.95, w: 4.5, h: 0.07, fill: { color: C.accent2 }, line: { type: "none" } });
s.addText("GROSS ANATOMY", { x: 0.35, y: 1.05, w: 4.2, h: 0.35, fontSize: 11, bold: true, color: C.accent2, fontFace: "Calibri", margin: 0 });
s.addText([
{ text: "• ", options: { bold: true } }, { text: "Location:", options: { bold: true } }, { text: " Anterior neck; inferior to larynx, anterior to trachea\n", options: {} },
{ text: "• ", options: { bold: true } }, { text: "Structure:", options: { bold: true } }, { text: " Two lateral lobes + isthmus (± pyramidal lobe)\n", options: {} },
{ text: "• ", options: { bold: true } }, { text: "Weight:", options: { bold: true } }, { text: " 20–30 g in adults\n", options: {} },
{ text: "• ", options: { bold: true } }, { text: "Blood supply:", options: { bold: true } }, { text: " Superior thyroid a. (ext. carotid), Inferior thyroid a. (thyrocervical trunk)\n", options: {} },
{ text: "• ", options: { bold: true } }, { text: "Blood flow:", options: { bold: true } }, { text: " 5× gland weight/minute — one of the highest in the body", options: {} },
], { x: 0.35, y: 1.42, w: 4.2, h: 1.8, fontSize: 10, color: C.textDark, fontFace: "Calibri", valign: "top", margin: 0 });
// Microscopic anatomy card
s.addShape(pres.shapes.RECTANGLE, { x: 5.0, y: 0.95, w: 4.7, h: 2.35, fill: { color: C.white }, line: { color: C.lightGray, pt: 1 } });
s.addShape(pres.shapes.RECTANGLE, { x: 5.0, y: 0.95, w: 4.7, h: 0.07, fill: { color: C.accent1 }, line: { type: "none" } });
s.addText("MICROSCOPIC ANATOMY", { x: 5.15, y: 1.05, w: 4.4, h: 0.35, fontSize: 11, bold: true, color: C.accent1, fontFace: "Calibri", margin: 0 });
s.addText([
{ text: "Follicles", options: { bold: true } }, { text: " (100–300 µm): closed sacs lined by cuboidal thyrocytes\n", options: {} },
{ text: "Colloid", options: { bold: true } }, { text: ": interior filled with thyroglobulin (T3/T4 storage)\n", options: {} },
{ text: "Follicular cells", options: { bold: true } }, { text: ": cuboidal → columnar when active\n", options: {} },
{ text: "C cells", options: { bold: true } }, { text: " (parafollicular): secrete ", options: {} }, { text: "calcitonin", options: { bold: true } }, { text: " → regulates plasma Ca²⁺\n", options: {} },
{ text: "Active gland", options: { bold: true, italic: true } }, { text: ": tall columnar cells, pale fluid colloid", options: { italic: true } },
], { x: 5.15, y: 1.42, w: 4.4, h: 1.8, fontSize: 10, color: C.textDark, fontFace: "Calibri", valign: "top", margin: 0 });
// Lymph / nerve
s.addShape(pres.shapes.RECTANGLE, { x: 0.2, y: 3.45, w: 9.5, h: 1.95, fill: { color: C.white }, line: { color: C.lightGray, pt: 1 } });
s.addShape(pres.shapes.RECTANGLE, { x: 0.2, y: 3.45, w: 9.5, h: 0.07, fill: { color: "546E7A" }, line: { type: "none" } });
s.addText("NEUROVASCULAR & LYMPHATICS", { x: 0.35, y: 3.55, w: 9.2, h: 0.3, fontSize: 10, bold: true, color: "546E7A", fontFace: "Calibri", margin: 0 });
s.addText([
{ text: "Nerve supply: ", options: { bold: true } }, { text: "Sympathetic fibers from superior & middle cervical ganglia (regulate blood flow) ", options: {} },
{ text: "Venous drainage: ", options: { bold: true } }, { text: "Superior, middle & inferior thyroid veins → internal jugular & brachiocephalic veins\n", options: {} },
{ text: "Lymphatic drainage: ", options: { bold: true } }, { text: "Pretracheal, paratracheal & deep cervical lymph nodes", options: {} },
], { x: 0.35, y: 3.87, w: 9.2, h: 1.45, fontSize: 10, color: C.textDark, fontFace: "Calibri", valign: "top", margin: 0 });
s.addText("Source: Guyton & Hall Textbook of Medical Physiology", { x: 0.2, y: 5.45, w: 9, h: 0.17, fontSize: 7.5, color: "AAAAAA", italic: true, fontFace: "Calibri", margin: 0 });
}
// ─────────────────────────────────────────────────────────────────────────
// SLIDE 5 – THYROID HORMONE SYNTHESIS
// ─────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offWhite }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.72, fill: { color: C.midBg }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0.72, w: 10, h: 0.06, fill: { color: C.accent2 }, line: { type: "none" } });
s.addText("02 PHYSIOLOGY – THYROID HORMONE SYNTHESIS", { x: 0.3, y: 0.15, w: 9.4, h: 0.42, fontSize: 14, bold: true, color: C.white, fontFace: "Calibri", margin: 0 });
// Step boxes
const steps = [
["1", "Iodide Trapping", "NIS (Na⁺-I⁻ symporter) concentrates I⁻ 30× plasma; up to 250× when maximally stimulated", C.accent2],
["2", "Oxidation", "Thyroid peroxidase (TPO) oxidises I⁻ → I₂ using H₂O₂ from DUOX2", C.accent1],
["3", "Organification", "I₂ added to tyrosine residues on thyroglobulin → MIT & DIT", "E53935"],
["4", "Coupling", "DIT + DIT → T4 (thyroxine) | MIT + DIT → T3 (triiodothyronine)", "7B1FA2"],
["5", "Storage", "Iodinated thyroglobulin stored in follicular colloid (weeks supply)", "00695C"],
["6", "Secretion", "TSH stimulates endocytosis of colloid → lysosomal cleavage → T3 & T4 released", C.midBg],
["7", "Conversion", "Peripheral 5'-deiodinase converts T4 → T3; >90% of nuclear-bound hormone is T3", "6D4C41"],
];
steps.forEach(([num, title, body, col], i) => {
const row = Math.floor(i / 4);
const col_i = i % 4;
const x = 0.2 + col_i * 2.4;
const y = 0.95 + row * 2.3;
const w = 2.25;
const h = 2.0;
if (i === 6) { // last one centered
const cx = 0.2 + 1.5 * 2.4;
s.addShape(pres.shapes.RECTANGLE, { x: cx, y, w, h, fill: { color: C.white }, line: { color: C.lightGray, pt: 1 } });
s.addShape(pres.shapes.RECTANGLE, { x: cx, y, w, h: 0.07, fill: { color: col }, line: { type: "none" } });
s.addText(`STEP ${num}`, { x: cx + 0.1, y: y + 0.12, w: w - 0.2, h: 0.28, fontSize: 9, bold: true, color: col, fontFace: "Calibri", margin: 0 });
s.addText(title, { x: cx + 0.1, y: y + 0.42, w: w - 0.2, h: 0.38, fontSize: 11, bold: true, color: C.textDark, fontFace: "Calibri", margin: 0 });
s.addText(body, { x: cx + 0.1, y: y + 0.82, w: w - 0.2, h: 1.05, fontSize: 9.5, color: C.textGray, fontFace: "Calibri", valign: "top", margin: 0 });
} else {
s.addShape(pres.shapes.RECTANGLE, { x, y, w, h, fill: { color: C.white }, line: { color: C.lightGray, pt: 1 } });
s.addShape(pres.shapes.RECTANGLE, { x, y, w, h: 0.07, fill: { color: col }, line: { type: "none" } });
s.addText(`STEP ${num}`, { x: x + 0.1, y: y + 0.12, w: w - 0.2, h: 0.28, fontSize: 9, bold: true, color: col, fontFace: "Calibri", margin: 0 });
s.addText(title, { x: x + 0.1, y: y + 0.42, w: w - 0.2, h: 0.38, fontSize: 11, bold: true, color: C.textDark, fontFace: "Calibri", margin: 0 });
s.addText(body, { x: x + 0.1, y: y + 0.82, w: w - 0.2, h: 1.05, fontSize: 9.5, color: C.textGray, fontFace: "Calibri", valign: "top", margin: 0 });
}
});
s.addText("Source: Guyton & Hall Textbook of Medical Physiology; Costanzo Physiology 7th Ed.", { x: 0.2, y: 5.45, w: 9, h: 0.17, fontSize: 7.5, color: "AAAAAA", italic: true, fontFace: "Calibri", margin: 0 });
}
// ─────────────────────────────────────────────────────────────────────────
// SLIDE 6 – HPT AXIS REGULATION
// ─────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offWhite }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.72, fill: { color: C.midBg }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0.72, w: 10, h: 0.06, fill: { color: C.accent2 }, line: { type: "none" } });
s.addText("02 PHYSIOLOGY – HPT AXIS & REGULATION", { x: 0.3, y: 0.15, w: 9.4, h: 0.42, fontSize: 14, bold: true, color: C.white, fontFace: "Calibri", margin: 0 });
// HPT axis diagram (drawn with shapes)
const boxes = [
{ label: "HYPOTHALAMUS", sub: "Paraventricular nucleus\n→ Secretes TRH", x: 3.5, y: 0.9, col: C.midBg },
{ label: "ANTERIOR PITUITARY", sub: "Thyrotrophs\n→ Secretes TSH", x: 3.5, y: 2.3, col: "37474F" },
{ label: "THYROID GLAND", sub: "Follicular cells\n→ Secretes T3 & T4", x: 3.5, y: 3.7, col: "4CAF50" },
];
boxes.forEach(({ label, sub, x, y, col }) => {
s.addShape(pres.shapes.RECTANGLE, { x, y, w: 3, h: 1.1, fill: { color: col }, line: { type: "none" }, shadow: { type: "outer", color: "000000", blur: 6, offset: 2, angle: 135, opacity: 0.2 } });
s.addText(label, { x, y: y + 0.1, w: 3, h: 0.4, fontSize: 11, bold: true, color: C.white, align: "center", fontFace: "Calibri", margin: 0 });
s.addText(sub, { x, y: y + 0.52, w: 3, h: 0.5, fontSize: 9.5, color: "E0E0E0", align: "center", fontFace: "Calibri", margin: 0 });
});
// arrows between boxes
s.addShape(pres.shapes.RECTANGLE, { x: 4.95, y: 2.0, w: 0.1, h: 0.32, fill: { color: C.accent1 }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 4.95, y: 3.4, w: 0.1, h: 0.32, fill: { color: C.accent1 }, line: { type: "none" } });
s.addText("TRH", { x: 5.15, y: 2.0, w: 1, h: 0.3, fontSize: 11, bold: true, color: C.accent1, fontFace: "Calibri", margin: 0 });
s.addText("TSH", { x: 5.15, y: 3.4, w: 1, h: 0.3, fontSize: 11, bold: true, color: C.accent1, fontFace: "Calibri", margin: 0 });
// feedback label
s.addText("(-) Negative\nFeedback", { x: 1.8, y: 2.5, w: 1.5, h: 0.7, fontSize: 10, bold: true, color: "E53935", align: "center", fontFace: "Calibri", margin: 0 });
s.addShape(pres.shapes.RECTANGLE, { x: 3.3, y: 2.8, w: 0.2, h: 0.05, fill: { color: "E53935" }, line: { type: "none" } });
// Physiological effects right column
const effects = [
["METABOLIC", "↑ BMR, calorigenic effect\n↑ carbohydrate & fat catabolism", "E53935"],
["CARDIOVASCULAR", "↑ HR, contractility, cardiac output\n↓ peripheral resistance", C.accent2],
["LIPID", "Upregulates LDL receptors\n↓ Total cholesterol & LDL-C", C.medaCol],
["BONE", "Regulates osteoblast & osteoclast\nNormal bone remodeling", C.asthiCol],
];
effects.forEach(([title, body, col], i) => {
const ey = 0.9 + i * 1.18;
s.addShape(pres.shapes.RECTANGLE, { x: 7.0, y: ey, w: 2.75, h: 1.0, fill: { color: C.white }, line: { color: C.lightGray, pt: 1 } });
s.addShape(pres.shapes.RECTANGLE, { x: 7.0, y: ey, w: 0.08, h: 1.0, fill: { color: col }, line: { type: "none" } });
s.addText(title, { x: 7.18, y: ey + 0.08, w: 2.5, h: 0.3, fontSize: 9, bold: true, color: col, fontFace: "Calibri", margin: 0 });
s.addText(body, { x: 7.18, y: ey + 0.4, w: 2.5, h: 0.55, fontSize: 9.5, color: C.textDark, fontFace: "Calibri", valign: "top", margin: 0 });
});
s.addText("Source: Costanzo Physiology 7th Ed.; Guyton & Hall", { x: 0.2, y: 5.45, w: 9, h: 0.17, fontSize: 7.5, color: "AAAAAA", italic: true, fontFace: "Calibri", margin: 0 });
}
// ─────────────────────────────────────────────────────────────────────────
// SLIDE 7 – CAUSES OF HYPOTHYROIDISM
// ─────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offWhite }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.72, fill: { color: "B71C1C" }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0.72, w: 10, h: 0.06, fill: { color: C.accent1 }, line: { type: "none" } });
s.addText("03 HYPOTHYROIDISM – CAUSES & CLASSIFICATION", { x: 0.3, y: 0.15, w: 9.4, h: 0.42, fontSize: 14, bold: true, color: C.white, fontFace: "Calibri", margin: 0 });
const causes = [
{
title: "PRIMARY (>95%)", col: "B71C1C",
items: "• Autoimmune: Hashimoto's thyroiditis (most common in iodine-sufficient regions), Atrophic thyroiditis\n• Iatrogenic: ¹³¹I therapy, thyroidectomy, neck irradiation\n• Drugs: Amiodarone, lithium, PTU, carbimazole, immune checkpoint inhibitors\n• Nutritional: Iodine deficiency (most common worldwide), selenium deficiency\n• Infiltrative: Amyloidosis, sarcoidosis, hemochromatosis, Riedel's thyroiditis\n• Congenital: Thyroid agenesis (65%), dyshormonogenesis (30%), TSH-R mutation (5%)"
},
{
title: "TRANSIENT", col: C.accent1,
items: "• Silent/postpartum thyroiditis\n• Subacute (de Quervain's) thyroiditis\n• Withdrawal of supraphysiologic T4 therapy"
},
{
title: "SECONDARY (Central)", col: C.midBg,
items: "• Pituitary disease: adenoma, surgery, Sheehan's syndrome\n• Hypothalamic disorders: tumors, trauma, Prader-Willi syndrome\n• Drugs: bexarotene, mitotane\n• Isolated TSH deficiency (rare)"
},
];
const xs = [0.2, 0.2, 6.8];
const ys = [0.9, 3.4, 0.9];
const ws = [6.4, 6.4, 3.0];
const hs = [2.3, 2.1, 4.6];
causes.forEach(({ title, col, items }, i) => {
s.addShape(pres.shapes.RECTANGLE, { x: xs[i], y: ys[i], w: ws[i], h: hs[i], fill: { color: C.white }, line: { color: C.lightGray, pt: 1 } });
s.addShape(pres.shapes.RECTANGLE, { x: xs[i], y: ys[i], w: ws[i], h: 0.07, fill: { color: col }, line: { type: "none" } });
s.addText(title, { x: xs[i] + 0.15, y: ys[i] + 0.12, w: ws[i] - 0.3, h: 0.35, fontSize: 11, bold: true, color: col, fontFace: "Calibri", margin: 0 });
s.addText(items, { x: xs[i] + 0.15, y: ys[i] + 0.52, w: ws[i] - 0.3, h: hs[i] - 0.65, fontSize: 9.5, color: C.textDark, fontFace: "Calibri", valign: "top", margin: 0 });
});
// Hashimoto highlight box
s.addShape(pres.shapes.RECTANGLE, { x: 6.8, y: 4.85, w: 3.0, h: 0.6, fill: { color: "FFEBEE" }, line: { color: "B71C1C", pt: 1 } });
s.addText("★ Hashimoto's: CD8⁺ T-cell + anti-TPO Ab mediated progressive thyroid destruction | F:M = 8:1", { x: 6.9, y: 4.9, w: 2.8, h: 0.5, fontSize: 8.5, color: "B71C1C", fontFace: "Calibri", valign: "middle", margin: 0 });
s.addText("Source: Harrison's Principles of Internal Medicine 22E (2025); Robbins, Cotran & Kumar Pathologic Basis of Disease", { x: 0.2, y: 5.46, w: 9, h: 0.16, fontSize: 7.5, color: "AAAAAA", italic: true, fontFace: "Calibri", margin: 0 });
}
// ─────────────────────────────────────────────────────────────────────────
// SLIDE 8 – CLINICAL FEATURES
// ─────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offWhite }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.72, fill: { color: "B71C1C" }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0.72, w: 10, h: 0.06, fill: { color: C.accent1 }, line: { type: "none" } });
s.addText("03 HYPOTHYROIDISM – CLINICAL FEATURES", { x: 0.3, y: 0.15, w: 9.4, h: 0.42, fontSize: 14, bold: true, color: C.white, fontFace: "Calibri", margin: 0 });
const systems = [
{ sys: "Constitutional", col: "78909C", items: "Fatigue · lethargy · cold intolerance\nWeight gain · hoarse voice" },
{ sys: "Skin & Hair", col: "E53935", items: "Dry skin · non-pitting myxedema\nPuffy face · diffuse alopecia\nBrittle nails · outer eyebrow loss" },
{ sys: "Cardiovascular", col: C.accent2, items: "Bradycardia · reduced cardiac output\nDiastolic HTN · pericardial effusion\nDyslipidemia (↑ LDL, TG)" },
{ sys: "Neuromuscular", col: C.medaCol, items: "Cognitive slowing · depression\nProximal muscle weakness\nDelayed DTR relaxation · CTS" },
{ sys: "GI / Repro", col: "00796B", items: "Constipation · poor appetite\nOligomenorrhea / amenorrhea\nHyperprolactinemia · infertility" },
{ sys: "Skeletal (Asthi)", col: C.asthiCol, items: "Reduced bone turnover\nReduced BMD (prolonged hT)\nJoint effusions · arthralgia" },
];
const positions = [
[0.2, 0.88], [3.45, 0.88], [6.7, 0.88],
[0.2, 2.82], [3.45, 2.82], [6.7, 2.82],
];
systems.forEach(({ sys, col, items }, i) => {
const [x, y] = positions[i];
s.addShape(pres.shapes.RECTANGLE, { x, y, w: 3.1, h: 1.78, fill: { color: C.white }, line: { color: C.lightGray, pt: 1 } });
s.addShape(pres.shapes.RECTANGLE, { x, y, w: 3.1, h: 0.07, fill: { color: col }, line: { type: "none" } });
s.addText(sys.toUpperCase(), { x: x + 0.12, y: y + 0.12, w: 2.86, h: 0.3, fontSize: 10, bold: true, color: col, fontFace: "Calibri", margin: 0 });
s.addText(items, { x: x + 0.12, y: y + 0.48, w: 2.86, h: 1.22, fontSize: 10, color: C.textDark, fontFace: "Calibri", valign: "top", margin: 0 });
});
s.addText("Source: Harrison's Principles of Internal Medicine 22E; The Washington Manual of Medical Therapeutics; Frameworks for Internal Medicine", { x: 0.2, y: 5.46, w: 9, h: 0.16, fontSize: 7.5, color: "AAAAAA", italic: true, fontFace: "Calibri", margin: 0 });
}
// ─────────────────────────────────────────────────────────────────────────
// SLIDE 9 – INVESTIGATIONS
// ─────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offWhite }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.72, fill: { color: "B71C1C" }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0.72, w: 10, h: 0.06, fill: { color: C.accent1 }, line: { type: "none" } });
s.addText("03 HYPOTHYROIDISM – INVESTIGATIONS", { x: 0.3, y: 0.15, w: 9.4, h: 0.42, fontSize: 14, bold: true, color: C.white, fontFace: "Calibri", margin: 0 });
// First-line tests
s.addShape(pres.shapes.RECTANGLE, { x: 0.2, y: 0.9, w: 4.5, h: 2.0, fill: { color: C.white }, line: { color: C.lightGray, pt: 1 } });
s.addShape(pres.shapes.RECTANGLE, { x: 0.2, y: 0.9, w: 4.5, h: 0.07, fill: { color: "B71C1C" }, line: { type: "none" } });
s.addText("FIRST-LINE / THYROID FUNCTION", { x: 0.35, y: 1.0, w: 4.2, h: 0.32, fontSize: 10, bold: true, color: "B71C1C", fontFace: "Calibri", margin: 0 });
s.addText(
"Serum TSH — most sensitive screening test\n Primary hT: TSH >4.5 mIU/L | Overt: TSH >20 mIU/L\n Secondary hT: TSH low/normal\nFree T4 (FT4) — decreased in overt hT; normal in subclinical\nFree T3 (FT3) — severity assessment",
{ x: 0.35, y: 1.35, w: 4.2, h: 1.48, fontSize: 9.5, color: C.textDark, fontFace: "Calibri", valign: "top", margin: 0 }
);
// Autoimmune markers
s.addShape(pres.shapes.RECTANGLE, { x: 5.1, y: 0.9, w: 4.6, h: 2.0, fill: { color: C.white }, line: { color: C.lightGray, pt: 1 } });
s.addShape(pres.shapes.RECTANGLE, { x: 5.1, y: 0.9, w: 4.6, h: 0.07, fill: { color: C.accent2 }, line: { type: "none" } });
s.addText("AUTOIMMUNE & IMAGING", { x: 5.25, y: 1.0, w: 4.3, h: 0.32, fontSize: 10, bold: true, color: C.accent2, fontFace: "Calibri", margin: 0 });
s.addText(
"Anti-TPO antibodies — elevated in 95% of Hashimoto's\nAnti-thyroglobulin antibodies — elevated ~60%\nTSH receptor antibodies (TRAb) — distinguish Graves'\nThyroid USG — echogenicity, nodules, gland size\nThyroid scan (¹²³I / ⁹⁹ᵐTc) — functional assessment",
{ x: 5.25, y: 1.35, w: 4.3, h: 1.48, fontSize: 9.5, color: C.textDark, fontFace: "Calibri", valign: "top", margin: 0 }
);
// Dhatu assessment table
s.addShape(pres.shapes.RECTANGLE, { x: 0.2, y: 3.05, w: 9.5, h: 2.42, fill: { color: C.white }, line: { color: C.lightGray, pt: 1 } });
s.addShape(pres.shapes.RECTANGLE, { x: 0.2, y: 3.05, w: 9.5, h: 0.07, fill: { color: "546E7A" }, line: { type: "none" } });
s.addText("SECONDARY INVESTIGATIONS FOR DHATU DUSHTI ASSESSMENT", { x: 0.35, y: 3.15, w: 9.2, h: 0.3, fontSize: 10, bold: true, color: "546E7A", fontFace: "Calibri", margin: 0 });
const invRows = [
["RASA DHATU", "CBC, Hb, serum albumin, total protein, ECG (bradycardia), RFT", C.rasaCol],
["MEDA DHATU", "Fasting lipid profile (LDL, HDL, TG, TC), fasting glucose, USG liver, BMI, waist circumference", C.medaCol],
["ASTHI DHATU", "Serum Ca, PO₄, ALP, Vitamin D (25-OH D₃), PTH, osteocalcin, bone-specific ALP, DEXA scan (T-score & Z-score)", C.asthiCol],
];
invRows.forEach(([dhatu, tests, col], i) => {
const ry = 3.5 + i * 0.6;
s.addShape(pres.shapes.RECTANGLE, { x: 0.2, y: ry, w: 2.0, h: 0.52, fill: { color: col + "22" }, line: { type: "none" } });
s.addText(dhatu, { x: 0.28, y: ry + 0.08, w: 1.84, h: 0.36, fontSize: 9.5, bold: true, color: col, fontFace: "Calibri", margin: 0, valign: "middle" });
s.addText(tests, { x: 2.35, y: ry + 0.06, w: 7.2, h: 0.4, fontSize: 9.5, color: C.textDark, fontFace: "Calibri", margin: 0, valign: "middle" });
});
s.addText("Source: Harrison's Principles 22E; Robbins, Cotran & Kumar; The Washington Manual", { x: 0.2, y: 5.46, w: 9, h: 0.16, fontSize: 7.5, color: "AAAAAA", italic: true, fontFace: "Calibri", margin: 0 });
}
// ─────────────────────────────────────────────────────────────────────────
// SECTION DIVIDER – AYURVEDIC
// ─────────────────────────────────────────────────────────────────────────
sectionDivider(pres, "PART B: AYURVEDIC REVIEW", "Rasa · Meda · Asthi Dhatu – Vriddhi & Kshaya Lakshanas", C.ayur);
// ─────────────────────────────────────────────────────────────────────────
// SLIDE 11 – RASA DHATU
// ─────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offWhite }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.72, fill: { color: C.rasaCol }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0.72, w: 10, h: 0.06, fill: { color: C.accent1 }, line: { type: "none" } });
s.addText("04 RASA DHATU – VRIDDHI & KSHAYA LAKSHANAS", { x: 0.3, y: 0.15, w: 9.4, h: 0.42, fontSize: 14, bold: true, color: C.white, fontFace: "Calibri", margin: 0 });
// Intro
s.addShape(pres.shapes.RECTANGLE, { x: 0.2, y: 0.9, w: 9.5, h: 0.72, fill: { color: C.rasaCol + "18" }, line: { color: C.rasaCol + "44", pt: 1 } });
s.addText([
{ text: "Rasa Dhatu ", options: { bold: true, color: C.rasaCol } },
{ text: "= Plasma/lymph/nutritional fluid. Formed from Ahara Rasa by Rasa Dhatwagni. Circulates via ", options: { color: C.textDark } },
{ text: "Rasavaha Srotas.", options: { bold: true, color: C.textDark } },
{ text: " Upadhatu: Stanya, Aartava | Mala: Kapha | Ref: Charaka Su. 17", options: { color: C.textGray } },
], { x: 0.35, y: 0.97, w: 9.2, h: 0.58, fontSize: 10.5, fontFace: "Calibri", valign: "middle", margin: 0 });
// Kshaya
s.addShape(pres.shapes.RECTANGLE, { x: 0.2, y: 1.75, w: 4.65, h: 3.7, fill: { color: C.white }, line: { color: C.lightGray, pt: 1 } });
s.addShape(pres.shapes.RECTANGLE, { x: 0.2, y: 1.75, w: 4.65, h: 0.07, fill: { color: C.rasaCol }, line: { type: "none" } });
s.addText("RASA KSHAYA (Depletion) Lakshanas", { x: 0.35, y: 1.85, w: 4.35, h: 0.35, fontSize: 10.5, bold: true, color: C.rasaCol, fontFace: "Calibri", margin: 0 });
const kshayas = [
["Hridrava", "Palpitations, cardiac pain"],
["Hridayam Tamyati", "Cardiac fatigue, minimal exertion"],
["Shrama (Alpacheshtasyapi)", "Fatigue even on minimal activity"],
["Sahate Shabdam Na", "Noise intolerance"],
["Ruksha Twak", "Dry, rough skin"],
["Pandu", "Pallor, anemia"],
["Ghattate", "Restlessness, anxiety"],
["Daurbalya", "General weakness"],
];
kshayas.forEach(([sk, en], i) => {
const ky = 2.28 + i * 0.39;
s.addText(`• ${sk}`, { x: 0.35, y: ky, w: 2.0, h: 0.35, fontSize: 10, bold: true, color: C.rasaCol, fontFace: "Calibri", margin: 0 });
s.addText(en, { x: 2.4, y: ky, w: 2.3, h: 0.35, fontSize: 10, color: C.textDark, fontFace: "Calibri", margin: 0 });
});
// Vriddhi
s.addShape(pres.shapes.RECTANGLE, { x: 5.1, y: 1.75, w: 4.65, h: 3.7, fill: { color: C.white }, line: { color: C.lightGray, pt: 1 } });
s.addShape(pres.shapes.RECTANGLE, { x: 5.1, y: 1.75, w: 4.65, h: 0.07, fill: { color: C.accent2 }, line: { type: "none" } });
s.addText("RASA VRIDDHI (Excess) Lakshanas", { x: 5.25, y: 1.85, w: 4.35, h: 0.35, fontSize: 10.5, bold: true, color: C.accent2, fontFace: "Calibri", margin: 0 });
const vriddhi = [
["Agnisadana", "Impaired digestion, poor appetite"],
["Praseka", "Excessive salivation / mucosal edema"],
["Alasya", "Sluggishness, lethargy"],
["Gaurava", "Heaviness of the body (myxedema)"],
["Shaithya", "Coldness – cold intolerance"],
["Shvaithya", "Pallor, white discoloration"],
["Shlathangatva", "Flaccidity, loose body parts"],
["Atinidrata", "Excessive sleep / hypersomnia"],
["Shwasa / Kasa", "Dyspnea, cough"],
];
vriddhi.forEach(([sk, en], i) => {
const vy = 2.28 + i * 0.39;
s.addText(`• ${sk}`, { x: 5.25, y: vy, w: 2.0, h: 0.35, fontSize: 10, bold: true, color: C.accent2, fontFace: "Calibri", margin: 0 });
s.addText(en, { x: 7.3, y: vy, w: 2.3, h: 0.35, fontSize: 10, color: C.textDark, fontFace: "Calibri", margin: 0 });
});
s.addText("Ref: Charaka Samhita, Sutra Sthana 17; Ashtanga Hridayam, Sutra Sthana 11", { x: 0.2, y: 5.46, w: 9, h: 0.16, fontSize: 7.5, color: "AAAAAA", italic: true, fontFace: "Calibri", margin: 0 });
}
// ─────────────────────────────────────────────────────────────────────────
// SLIDE 12 – MEDA DHATU
// ─────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offWhite }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.72, fill: { color: C.medaCol }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0.72, w: 10, h: 0.06, fill: { color: C.accent1 }, line: { type: "none" } });
s.addText("05 MEDO DHATU – VRIDDHI & KSHAYA LAKSHANAS", { x: 0.3, y: 0.15, w: 9.4, h: 0.42, fontSize: 14, bold: true, color: C.white, fontFace: "Calibri", margin: 0 });
// Intro bar
s.addShape(pres.shapes.RECTANGLE, { x: 0.2, y: 0.9, w: 9.5, h: 0.72, fill: { color: C.medaCol + "15" }, line: { color: C.medaCol + "44", pt: 1 } });
s.addText([
{ text: "Meda Dhatu ", options: { bold: true, color: C.medaCol } },
{ text: "= Adipose/fat tissue. 4th Dhatu formed from Mamsa Dhatu by Meda Dhatwagni. ", options: { color: C.textDark } },
{ text: "Karma: Sneha (unctuousness), Svedana (perspiration), Balya (nourishes Asthi) | Upadhatu: Snayu | Mala: Sweda", options: { color: C.textGray } },
], { x: 0.35, y: 0.97, w: 9.2, h: 0.58, fontSize: 10.5, fontFace: "Calibri", valign: "middle", margin: 0 });
// Kshaya
s.addShape(pres.shapes.RECTANGLE, { x: 0.2, y: 1.75, w: 4.65, h: 3.7, fill: { color: C.white }, line: { color: C.lightGray, pt: 1 } });
s.addShape(pres.shapes.RECTANGLE, { x: 0.2, y: 1.75, w: 4.65, h: 0.07, fill: { color: C.medaCol }, line: { type: "none" } });
s.addText("MEDA KSHAYA Lakshanas", { x: 0.35, y: 1.85, w: 4.35, h: 0.35, fontSize: 10.5, bold: true, color: C.medaCol, fontFace: "Calibri", margin: 0 });
const medaK = [
["Sphik Shushkata", "Emaciation of buttocks"],
["Udara Shushkata", "Abdominal hollowness"],
["Stana Shushkata", "Loss of breast tissue bulk"],
["Parvakam Graha", "Stiffness of small joints"],
["Shrama / Atishrama", "Fatigue, exhaustion"],
["Shosha", "Emaciation, wasting"],
["Pleeha Vriddhi", "Splenomegaly"],
];
medaK.forEach(([sk, en], i) => {
const ky = 2.28 + i * 0.45;
s.addText(`• ${sk}`, { x: 0.35, y: ky, w: 2.2, h: 0.4, fontSize: 10, bold: true, color: C.medaCol, fontFace: "Calibri", margin: 0 });
s.addText(en, { x: 2.6, y: ky, w: 2.1, h: 0.4, fontSize: 10, color: C.textDark, fontFace: "Calibri", margin: 0 });
});
// Vriddhi
s.addShape(pres.shapes.RECTANGLE, { x: 5.1, y: 1.75, w: 4.65, h: 3.7, fill: { color: C.white }, line: { color: C.lightGray, pt: 1 } });
s.addShape(pres.shapes.RECTANGLE, { x: 5.1, y: 1.75, w: 4.65, h: 0.07, fill: { color: C.accent2 }, line: { type: "none" } });
s.addText("MEDA VRIDDHI Lakshanas ★ Most prevalent in hypothyroidism (78.2%)", { x: 5.25, y: 1.85, w: 4.35, h: 0.35, fontSize: 10, bold: true, color: C.accent2, fontFace: "Calibri", margin: 0 });
const medaV = [
["Sthoulya", "Obesity, weight gain"],
["Udara Vriddhi", "Abdominal enlargement"],
["Shramena Shwasa", "Exertional dyspnea"],
["Daurgandhya", "Foul body odour (Ama)"],
["Daurbalya", "Weakness despite bulk"],
["Kandu", "Itching, skin changes"],
["Medovaha Sroto Dushti", "Dyslipidemia (↑LDL, TG)"],
["Yaka-ashrita Meda", "Fatty liver (NAFLD)"],
];
medaV.forEach(([sk, en], i) => {
const vy = 2.28 + i * 0.45;
s.addText(`• ${sk}`, { x: 5.25, y: vy, w: 2.25, h: 0.4, fontSize: 10, bold: true, color: C.accent2, fontFace: "Calibri", margin: 0 });
s.addText(en, { x: 7.55, y: vy, w: 2.1, h: 0.4, fontSize: 10, color: C.textDark, fontFace: "Calibri", margin: 0 });
});
s.addText("Ref: Charaka Samhita, Su. 17; JAIMS Observational Study n=100; Fitzpatrick's Dermatology Vol.1", { x: 0.2, y: 5.46, w: 9, h: 0.16, fontSize: 7.5, color: "AAAAAA", italic: true, fontFace: "Calibri", margin: 0 });
}
// ─────────────────────────────────────────────────────────────────────────
// SLIDE 13 – ASTHI DHATU
// ─────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offWhite }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.72, fill: { color: C.asthiCol }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0.72, w: 10, h: 0.06, fill: { color: C.accent1 }, line: { type: "none" } });
s.addText("06 ASTHI DHATU – VRIDDHI & KSHAYA LAKSHANAS", { x: 0.3, y: 0.15, w: 9.4, h: 0.42, fontSize: 14, bold: true, color: C.white, fontFace: "Calibri", margin: 0 });
// Intro bar
s.addShape(pres.shapes.RECTANGLE, { x: 0.2, y: 0.9, w: 9.5, h: 0.72, fill: { color: C.asthiCol + "15" }, line: { color: C.asthiCol + "55", pt: 1 } });
s.addText([
{ text: "Asthi Dhatu ", options: { bold: true, color: C.asthiCol } },
{ text: "= Bone tissue (5th Dhatu). Formed from Meda Dhatu. ", options: { color: C.textDark } },
{ text: "Seat of Vata Dosha (Ashraya-Ashrayi). Mala: Kesha, Loma, Nakha, Shmashru | Ref: Ch. Sha. 7/15; Su. Su. 14/10", options: { color: C.textGray } },
], { x: 0.35, y: 0.97, w: 9.2, h: 0.58, fontSize: 10.5, fontFace: "Calibri", valign: "middle", margin: 0 });
// Kshaya
s.addShape(pres.shapes.RECTANGLE, { x: 0.2, y: 1.75, w: 4.65, h: 3.7, fill: { color: C.white }, line: { color: C.lightGray, pt: 1 } });
s.addShape(pres.shapes.RECTANGLE, { x: 0.2, y: 1.75, w: 4.65, h: 0.07, fill: { color: C.asthiCol }, line: { type: "none" } });
s.addText("ASTHI KSHAYA Lakshanas ★ Predominant pattern in hypothyroidism", { x: 0.35, y: 1.85, w: 4.35, h: 0.35, fontSize: 10, bold: true, color: C.asthiCol, fontFace: "Calibri", margin: 0 });
const asthiK = [
["Kesha Patana", "Hair fall (telogen effluvium)"],
["Loma Patana", "Loss of body hair"],
["Nakha Patana / Bhanga", "Brittle nails, nail loss"],
["Shmashru Patana", "Loss of beard / facial hair"],
["Asthishula", "Bone pain, arthralgia"],
["Asthisphotana", "Joint crackling, crepitus"],
["Sandhi Shaithilya", "Joint laxity"],
["Asthi Daurbalya", "Bone fragility (low BMD)"],
["Shrama", "Fatigue"],
];
asthiK.forEach(([sk, en], i) => {
const ky = 2.28 + i * 0.39;
s.addText(`• ${sk}`, { x: 0.35, y: ky, w: 2.3, h: 0.35, fontSize: 10, bold: true, color: C.asthiCol, fontFace: "Calibri", margin: 0 });
s.addText(en, { x: 2.7, y: ky, w: 2.0, h: 0.35, fontSize: 10, color: C.textDark, fontFace: "Calibri", margin: 0 });
});
// Vriddhi
s.addShape(pres.shapes.RECTANGLE, { x: 5.1, y: 1.75, w: 4.65, h: 1.65, fill: { color: C.white }, line: { color: C.lightGray, pt: 1 } });
s.addShape(pres.shapes.RECTANGLE, { x: 5.1, y: 1.75, w: 4.65, h: 0.07, fill: { color: C.accent2 }, line: { type: "none" } });
s.addText("ASTHI VRIDDHI Lakshanas (less common in hT)", { x: 5.25, y: 1.85, w: 4.35, h: 0.35, fontSize: 10, bold: true, color: C.accent2, fontFace: "Calibri", margin: 0 });
const asthiV = [
["Adhyasthi", "Extra bone / calcification / exostosis"],
["Adhidanta", "Hyperdontia, extra teeth"],
["Keshatimatra", "Excessive hair growth"],
];
asthiV.forEach(([sk, en], i) => {
const vy = 2.28 + i * 0.46;
s.addText(`• ${sk}`, { x: 5.25, y: vy, w: 2.0, h: 0.4, fontSize: 10, bold: true, color: C.accent2, fontFace: "Calibri", margin: 0 });
s.addText(en, { x: 7.3, y: vy, w: 2.35, h: 0.4, fontSize: 10, color: C.textDark, fontFace: "Calibri", margin: 0 });
});
// Asthi Mala interpretation box
s.addShape(pres.shapes.RECTANGLE, { x: 5.1, y: 3.55, w: 4.65, h: 1.85, fill: { color: "FFF3E0" }, line: { color: C.asthiCol, pt: 1 } });
s.addText("KEY INTERPRETATION: ASTHI MALA", { x: 5.25, y: 3.65, w: 4.35, h: 0.32, fontSize: 10, bold: true, color: C.asthiCol, fontFace: "Calibri", margin: 0 });
s.addText(
"Hair (Kesha) & Nails (Nakha) are Mala (waste products) of Asthi Dhatu. Their loss in hypothyroidism is the early clinical marker of Asthi Dhatu Kshaya — visible before bone density changes appear on DEXA.\n\nHypothyroid hair loss = telogen effluvium; brittle nails = reduced matrix cell proliferation.",
{ x: 5.25, y: 4.0, w: 4.35, h: 1.3, fontSize: 9.5, color: C.textDark, fontFace: "Calibri", valign: "top", margin: 0 }
);
s.addText("Ref: Charaka Samhita Su. 17; Sushruta Su. 14/10; IJRAP Pilot Study (BMD & Hair Fall)", { x: 0.2, y: 5.46, w: 9, h: 0.16, fontSize: 7.5, color: "AAAAAA", italic: true, fontFace: "Calibri", margin: 0 });
}
// ─────────────────────────────────────────────────────────────────────────
// SLIDE 14 – DHATU DUSHTI CORRELATION FLOWCHART
// ─────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offWhite }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.72, fill: { color: C.ayur }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0.72, w: 10, h: 0.06, fill: { color: C.accent1 }, line: { type: "none" } });
s.addText("07 DHATU DUSHTI IN HYPOTHYROIDISM – CORRELATION", { x: 0.3, y: 0.15, w: 9.4, h: 0.42, fontSize: 14, bold: true, color: C.white, fontFace: "Calibri", margin: 0 });
// Samprapti chain – boxes
const chain = [
{ label: "Hypothyroidism\n(↓ T3/T4)", sub: "Nidana activation", col: "B71C1C", x: 0.25, y: 0.9 },
{ label: "Jataragni Mandya\n+ Kapha Vriddhi", sub: "Agni impairment", col: C.midBg, x: 0.25, y: 1.9 },
{ label: "Ama formation\nRasa Dhatu Dushti", sub: "43% of hT cases", col: C.rasaCol, x: 0.25, y: 2.9 },
{ label: "Meda Dhatwagni\nMandya + Meda Vriddhi", sub: "78.2% of hT cases", col: C.medaCol, x: 0.25, y: 3.9 },
{ label: "Asthi Dhatu\nKshaya", sub: "Sequential depletion", col: C.asthiCol, x: 0.25, y: 4.77 },
];
chain.forEach(({ label, sub, col, x, y }, i) => {
s.addShape(pres.shapes.RECTANGLE, { x, y, w: 2.9, h: 0.82, fill: { color: col }, line: { type: "none" }, shadow: { type: "outer", color: "000000", blur: 6, offset: 2, angle: 135, opacity: 0.15 } });
s.addText(label, { x: x + 0.1, y: y + 0.04, w: 2.7, h: 0.5, fontSize: 10, bold: true, color: C.white, fontFace: "Calibri", margin: 0 });
s.addText(sub, { x: x + 0.1, y: y + 0.55, w: 2.7, h: 0.25, fontSize: 8.5, color: "FFD0A0", fontFace: "Calibri", margin: 0, italic: true });
if (i < 4) {
s.addShape(pres.shapes.RECTANGLE, { x: x + 1.4, y: y + 0.83, w: 0.1, h: 0.1, fill: { color: col }, line: { type: "none" } });
}
});
// Right column – interpretation cards
const interps = [
{ title: "RASA DUSHTI", body: "Sama Rasa → poor quality plasma\nFeatures: Gaurava, Alasya, Shaithya, Atinidrata\nModern: fatigue, cold intolerance, myxedema", col: C.rasaCol },
{ title: "MEDA DUSHTI", body: "Medovaha Sroto Dushti (Sanga type)\nFeatures: Sthoulya, dyslipidemia, NAFLD\nModern: ↑LDL, ↑TG, weight gain, fatty liver", col: C.medaCol },
{ title: "ASTHI KSHAYA", body: "Meda Dushti → impaired Asthi formation\nFeatures: Kesha/Nakha Patana, Asthishula\nModern: hair loss, brittle nails, ↓BMD", col: C.asthiCol },
];
interps.forEach(({ title, body, col }, i) => {
const iy = 0.9 + i * 1.55;
s.addShape(pres.shapes.RECTANGLE, { x: 3.5, y: iy, w: 6.3, h: 1.38, fill: { color: C.white }, line: { color: col, pt: 1.5 } });
s.addShape(pres.shapes.RECTANGLE, { x: 3.5, y: iy, w: 0.12, h: 1.38, fill: { color: col }, line: { type: "none" } });
s.addText(title, { x: 3.75, y: iy + 0.1, w: 5.9, h: 0.35, fontSize: 11, bold: true, color: col, fontFace: "Calibri", margin: 0 });
s.addText(body, { x: 3.75, y: iy + 0.5, w: 5.9, h: 0.82, fontSize: 10, color: C.textDark, fontFace: "Calibri", valign: "top", margin: 0 });
});
s.addText("Source: JAIMS observational study (n=100); Charaka Samhita; Harrison's Principles 22E", { x: 0.2, y: 5.46, w: 9, h: 0.16, fontSize: 7.5, color: "AAAAAA", italic: true, fontFace: "Calibri", margin: 0 });
}
// ─────────────────────────────────────────────────────────────────────────
// SLIDE 15 – SUMMARY TABLE
// ─────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.offWhite }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.72, fill: { color: C.darkBg }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0.72, w: 10, h: 0.06, fill: { color: C.accent1 }, line: { type: "none" } });
s.addText("SUMMARY – DHATU DUSHTI FRAMEWORK IN HYPOTHYROIDISM", { x: 0.3, y: 0.15, w: 9.4, h: 0.42, fontSize: 13, bold: true, color: C.white, fontFace: "Calibri", margin: 0 });
// Table header
const headers = ["Dhatu", "Key Lakshana (Ayurvedic)", "Clinical Feature (Modern)", "Investigation"];
const hws = [1.2, 3.0, 2.7, 2.8];
let hx = 0.2;
headers.forEach((h, i) => {
s.addShape(pres.shapes.RECTANGLE, { x: hx, y: 0.9, w: hws[i], h: 0.4, fill: { color: C.darkBg }, line: { type: "none" } });
s.addText(h, { x: hx + 0.07, y: 0.93, w: hws[i] - 0.14, h: 0.34, fontSize: 10, bold: true, color: C.white, fontFace: "Calibri", valign: "middle", margin: 0 });
hx += hws[i];
});
const rows = [
{ dhatu: "Rasa\nKshaya", col: C.rasaCol, lakshana: "Hridrava, Pandu, Alasya,\nGaurava, Shaithya, Atinidrata", modern: "Fatigue, pallor, cold\nintolerance, myxedema", inv: "Hb, serum albumin,\nECG, TSH" },
{ dhatu: "Rasa\nVriddhi", col: C.rasaCol + "88", lakshana: "Agnisadana, Praseka,\nShlathangatva, Shwasa", modern: "Poor digestion, mucosal\nedema, flaccidity", inv: "Serum protein, TSH" },
{ dhatu: "Meda\nVriddhi", col: C.medaCol, lakshana: "Sthoulya, Medovaha\nSroto Dushti, Daurgandhya", modern: "Weight gain, dyslipidemia\n(↑LDL, ↑TG), NAFLD", inv: "Lipid profile, USG\nliver, BMI" },
{ dhatu: "Meda\nKshaya", col: C.medaCol + "88", lakshana: "Sphik Shushkata, Atishrama,\nShosha", modern: "Emaciation (severe cases)", inv: "BMI, skinfold" },
{ dhatu: "Asthi\nKshaya", col: C.asthiCol, lakshana: "Kesha/Nakha Patana,\nAsthishula, Sandhi Shaithilya", modern: "Hair fall, brittle nails,\nbone pain, ↓BMD", inv: "DEXA, Vit D, PTH,\nCa, ALP, osteocalcin" },
{ dhatu: "Asthi\nVriddhi", col: C.asthiCol + "88", lakshana: "Adhyasthi, Adhidanta", modern: "Calcification (not typical\nin hypothyroidism)", inv: "X-ray" },
];
rows.forEach((row, i) => {
const ry = 1.35 + i * 0.7;
const bg = i % 2 === 0 ? C.white : "F0F4F8";
s.addShape(pres.shapes.RECTANGLE, { x: 0.2, y: ry, w: 9.6, h: 0.65, fill: { color: bg }, line: { color: C.lightGray, pt: 0.5 } });
// dhatu cell with color
s.addShape(pres.shapes.RECTANGLE, { x: 0.2, y: ry, w: 0.1, h: 0.65, fill: { color: row.col }, line: { type: "none" } });
s.addText(row.dhatu, { x: 0.35, y: ry + 0.04, w: 0.95, h: 0.57, fontSize: 9.5, bold: true, color: row.col.length > 7 ? C.textGray : row.col, fontFace: "Calibri", valign: "middle", margin: 0 });
let cx = 1.4;
[row.lakshana, row.modern, row.inv].forEach((cell, ci) => {
const cw = hws[ci + 1];
s.addText(cell, { x: cx + 0.07, y: ry + 0.04, w: cw - 0.14, h: 0.57, fontSize: 9, color: C.textDark, fontFace: "Calibri", valign: "middle", margin: 0 });
cx += cw;
});
});
s.addText("Sources: Charaka Samhita Su. 17; Harrison's 22E; Guyton & Hall; Costanzo Physiology; JAIMS Observational Study (n=100)", { x: 0.2, y: 5.46, w: 9.4, h: 0.16, fontSize: 7.5, color: "AAAAAA", italic: true, fontFace: "Calibri", margin: 0 });
}
// ─────────────────────────────────────────────────────────────────────────
// SLIDE 16 – CONCLUSION / THANK YOU
// ─────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 5.625, fill: { color: C.darkBg }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0, w: 10, h: 0.18, fill: { color: C.accent1 }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 5.45, w: 10, h: 0.18, fill: { color: C.accent1 }, line: { type: "none" } });
s.addShape(pres.shapes.RECTANGLE, { x: 0, y: 0.18, w: 0.45, h: 5.27, fill: { color: C.midBg }, line: { type: "none" } });
s.addText("KEY CONCLUSIONS", { x: 0.7, y: 0.4, w: 9, h: 0.4, fontSize: 13, bold: true, color: C.accent1, charSpacing: 4, fontFace: "Calibri", margin: 0 });
const conclusions = [
["Meda Dhatu Vriddhi", "is the most prevalent Dhatu Dushti in hypothyroidism (78.2%) — driven by Meda Dhatwagni Mandya and directly correlating with dyslipidemia (↑LDL, ↑TG).", C.medaCol],
["Rasa Dhatu Dushti", "is found in 43% of cases. Gaurava, Shaithya, Atinidrata, Shlathangatva map directly to cardinal hypothyroid symptoms via Ama formation and Rasavaha Sroto Dushti.", C.rasaCol],
["Asthi Dhatu Kshaya", "represents an underexplored but mechanistically essential finding — Meda Dushti impairs Asthi formation. Hair loss and brittle nails (Asthi Mala) are early clinical markers preceding DEXA changes.", C.asthiCol],
["Sequential Samprapti", "validates the Dhatu Poshana Krama: Hypothyroidism → Agni Mandya → Rasa Dushti → Meda Vriddhi → Asthi Kshaya — all three Dhatus are simultaneously involved via a chain mechanism.", C.accent1],
];
conclusions.forEach(([title, body, col], i) => {
const cy = 0.95 + i * 1.1;
s.addShape(pres.shapes.RECTANGLE, { x: 0.7, y: cy, w: 9.1, h: 0.95, fill: { color: col + "22" }, line: { color: col + "66", pt: 1 } });
s.addShape(pres.shapes.RECTANGLE, { x: 0.7, y: cy, w: 0.1, h: 0.95, fill: { color: col }, line: { type: "none" } });
s.addText([
{ text: title + " ", options: { bold: true, color: col } },
{ text: body, options: { color: C.white } },
], { x: 0.9, y: cy + 0.1, w: 8.8, h: 0.77, fontSize: 10.5, fontFace: "Calibri", valign: "middle", margin: 0 });
});
}
// ─── WRITE FILE ───────────────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/hypothyroid-pptx/Rasa_Meda_Asthi_Hypothyroidism_Literature_Review.pptx" })
.then(() => console.log("✅ Presentation saved successfully."))
.catch(err => { console.error("❌ Error:", err); process.exit(1); });
cd /home/daytona/workspace/hypothyroid-pptx && node build.js 2>&1
~/hypothyroid-pptx/build.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/hypothyroid-pptx/build.js'
cd /home/daytona/workspace/hypothyroid-pptx && sed -i \ "s/C\.rasaCol + '22'/'D0E4F7'/g; s/C\.medaCol + '22'/'EDE7F6'/g; s/C\.asthiCol + '22'/'FBE9E7'/g; \ s/C\.rasaCol + '18'/'D0E4F7'/g; s/C\.rasaCol + '44'/C.rasaCol/g; \ s/C\.medaCol + '15'/'EDE7F6'/g; s/C\.medaCol + '44'/C.medaCol/g; \ s/C\.asthiCol + '15'/'FBE9E7'/g; s/C\.asthiCol + '55'/C.asthiCol/g; \ s/C\.rasaCol + '88'/'5D89B8'/g; s/C\.medaCol + '88'/'9C6EB8'/g; s/C\.asthiCol + '88'/'D07A60'/g; \ s/C\.medaCol + '66'/C.medaCol/g; s/C\.medaCol + '33'/'D4B8E8'/g; \ s/C\.rasaCol + '66'/C.rasaCol/g; s/C\.asthiCol + '66'/C.asthiCol/g; \ s/C\.accent1 + '22'/'FBF0D5'/g; s/C\.accent1 + '66'/C.accent1/g" build.js && node build.js 2>&1
ls -lh /home/daytona/workspace/hypothyroid-pptx/Rasa_Meda_Asthi_Hypothyroidism_Literature_Review.pptx
Rasa Meda Asthi Hypothyroidism Literature Review
Presentation · PPTX
Presentation Overview - 16 Slides
| Slide | Content |
|---|---|
| 1 | Title slide - thesis name, department, year |
| 2 | Visual outline - 7 color-coded section columns |
| 3 | Section divider - Part A: Modern Review |
| 4 | Functional Anatomy - gross anatomy, microscopic anatomy, neurovascular |
| 5 | Physiology - 7-step hormone synthesis (Step 1-7 cards) |
| 6 | HPT Axis regulation diagram + key physiological effects (metabolic, CV, lipid, bone) |
| 7 | Causes of hypothyroidism - Primary / Transient / Secondary with Hashimoto highlight |
| 8 | Clinical features - 6 system cards (Constitutional, Skin, Cardiovascular, Neuromuscular, GI/Repro, Skeletal) |
| 9 | Investigations - thyroid function tests, autoimmune markers, + Dhatu Dushti assessment table |
| 10 | Section divider - Part B: Ayurvedic Review |
| 11 | Rasa Dhatu - Kshaya Lakshanas vs Vriddhi Lakshanas (side-by-side) |
| 12 | Meda Dhatu - Kshaya vs Vriddhi Lakshanas, with 78.2% statistic highlighted |
| 13 | Asthi Dhatu - Kshaya vs Vriddhi + interpretive box on Kesha/Nakha as Asthi Mala |
| 14 | Correlation flowchart - Samprapti chain + modern-Ayurvedic interpretation cards |
| 15 | Summary table - all 6 Dhatu states with Lakshana, Clinical Feature, and Investigation |
| 16 | Conclusions - 4 key takeaways with color-coded accent blocks |
download me above ppt
Rasa Meda Asthi Hypothyroidism Literature Review
Presentation · PPTX
/home/daytona/workspace/hypothyroid-pptx/. Click the link above and your browser will download it as a .pptx file that opens directly in Microsoft PowerPoint or Google Slides.