Explain ddh from maheswari
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to give a thorough answer. Note that Maheshwari's "Essential Orthopaedics" is not in the library, but the content below is drawn from the standard orthopaedic references (Miller's Review of Orthopaedics and Campbell's) which cover the same DDH material as Maheshwari. The content aligns closely with what Maheshwari teaches.
Developmental Dysplasia of the Hip (DDH)
(Based on standard orthopaedic references - Miller's Review of Orthopaedics, 9th Ed. and Campbell's Operative Orthopaedics, 15th Ed. Note: Maheshwari's "Essential Orthopaedics" is not available in the current textbook library, but the content below reflects the same standard teaching.)
Definition
DDH describes a spectrum of hip abnormalities ranging from acetabular dysplasia (shallow socket) through subluxation (partial dislocation) to complete dislocation of the femoral head from the true acetabulum. In a newborn, the femoral head can often be dislocated and reduced in and out of the acetabulum. In older children, the head remains dislocated and secondary structural changes develop.
Incidence
- ~1 in 1000 live births (clinically)
- Up to 25 per 1000 by ultrasound screening
- Left hip involved in 67% of cases; bilateral > right hip alone
- Girls affected 5x more commonly than boys (85% of cases are female)
Spectrum of Disease
| Type | Description |
|---|---|
| Dysplasia | Shallow acetabulum only; head still seated |
| Subluxation | Partial dislocation |
| Dislocation | Complete displacement |
| Teratologic | Dislocated in utero, irreducible at birth; associated with neuromuscular conditions (arthrogryposis, Larsen syndrome) |
| Late (adolescent/adult) | Residual undiagnosed dysplasia presenting later |
Risk Factors
In order of importance:
- Breech positioning (incidence 30-50% in breech; female + breech = 2.8% risk)
- Positive family history (risk ~10-20%)
- Female sex (85% of cases)
- Firstborn child (less intrauterine space)
- Oligohydramnios
- Swaddling with hips in extension (postnatal cultural practice)
- Increased maternal estrogens / hormone-induced ligamentous laxity (relaxin crosses placenta)
The most common intrauterine position (left occiput anterior) pushes the left hip into adduction against the maternal lumbosacral spine - explaining the left-sided predominance.
Associated Conditions
- Congenital muscular torticollis (~20% of DDH cases; boys 5x more likely to have both)
- Metatarsus adductus (~10%)
- Talipes calcaneovalgus
- No association with clubfoot (though screening is still recommended)
Pathological Anatomy / Blocks to Reduction
If untreated, secondary changes occur:
- Acetabulum becomes dysplastic and fills with fibrofatty tissue (pulvinar)
- Muscles around the hip contract
- A pseudoacetabulum forms in the teratologic form
The following structures become obstacles to achieving concentric reduction:
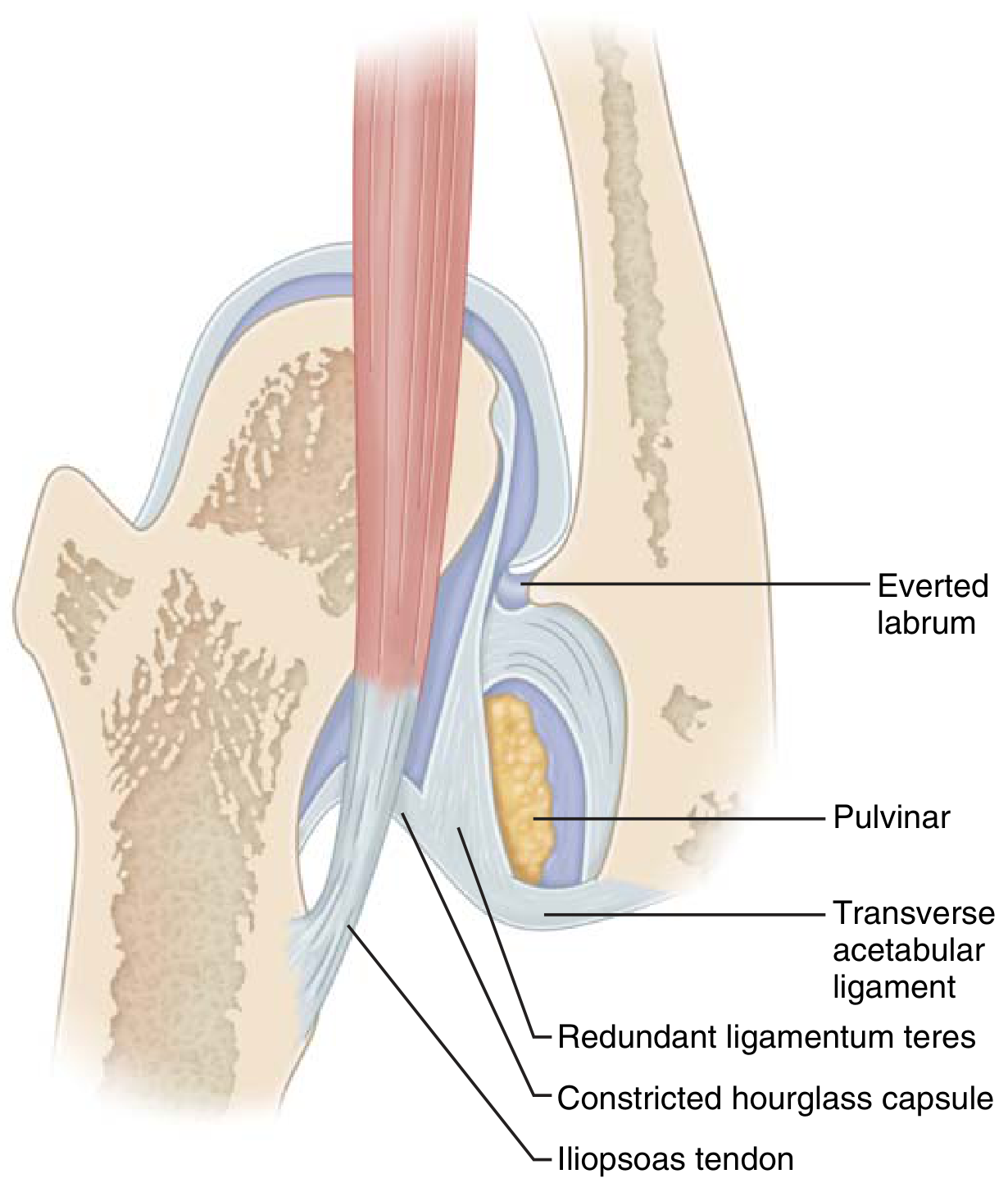
- Iliopsoas tendon (crosses anterior to hip, constricts capsule)
- Pulvinar (fibrofatty tissue fills acetabulum)
- Hypertrophied/redundant ligamentum teres
- Contracted inferomedial hip capsule (hourglass deformity)
- Transverse acetabular ligament
- Inverted/everted labrum
Clinical Features & Diagnosis
By Age Group
Newborn / <6 months:
- Ortolani test - gentle abduction reduces a dislocated hip (clunk = positive = dislocated but reducible)
- Barlow test - adduction + posterior pressure dislocates a dislocatable hip (positive = subluxable/dislocatable)
- Phases: Dislocated → Dislocatable → Subluxable
- Infant must be calm; examine one hip at a time
>3-6 months (laxity resolves, stiffness sets in):
- Limited hip abduction on the affected side (most reliable sign)
- Caution: bilateral dislocation gives symmetric limitation
- Galeazzi sign - apparent femoral shortening; patient supine with feet together and knees flexed; affected knee is lower
- Asymmetric skin/gluteal folds (less reliable)
Walking age / Older children:
- Trendelenburg gait (abductor weakness)
- Increased lumbar lordosis
- Pelvic obliquity
- Limb length discrepancy
Investigations
Ultrasound (Graf Classification)
- Best for infants <4-6 months (before femoral head ossifies)
- Graf alpha angle >60° = normal; measures bony acetabular coverage
- Also assesses dynamic stability and reduction in Pavlik harness
- Avoid before 6 weeks of age - physiologic ligamentous laxity causes false positives
- Highly operator-dependent
Plain Radiograph (used >4 months)
Key lines and measurements on AP pelvis:
| Parameter | Description | Normal |
|---|---|---|
| Acetabular index (AI) | Angle of acetabular roof slope | <25° (25-30° borderline, >30° abnormal) |
| Hilgenreiner's line | Horizontal line through both triradiate cartilages | Reference line |
| Perkin's line | Vertical line from lateral acetabular edge | Femoral head ossific nucleus should be medial to this |
| Shenton's line | Curved line along femoral neck and superior pubic ramus | Disrupted in dislocation |
| Center-edge (CE) angle | Lateral femoral head coverage | >20° normal in older children |
- Delayed ossification of femoral head on affected side
- Femoral head displaced laterally and superiorly in dislocation
Treatment (Age-Based)
0-6 Months - Pavlik Harness
- First-line treatment; maintains hip in ~100° flexion and mild abduction ("safe zone of Ramsey")
- Worn 23 hrs/day for ≥6 weeks post-reduction, then part-time 6-8 weeks
- Confirm reduction by ultrasound/X-ray after placement
- Safe zone of Ramsey: between maximum adduction (risk of re-dislocation) and excessive abduction (risk of AVN)
Contraindications to Pavlik harness:
- Teratologic dislocations
- Narrow safe zone (<40° - consider adductor tenotomy first)
Pavlik harness failure (if no reduction in 3 weeks): Stop harness to prevent "Pavlik disease" (erosion of pelvis above acetabulum)
Risk factors for Pavlik failure:
- Age >7 weeks at start
- Bilateral dislocation
- Male sex
If dislocated and harness fails: transition to rigid abduction orthosis or closed reduction + spica cast
6-18 Months - Closed Reduction + Spica Cast
- Hip arthrography + percutaneous adductor tenotomy + closed reduction + hip spica cast
- Post-reduction CT or MRI to confirm concentric reduction
- Open reduction if closed fails
18 Months - 3 Years - Open Reduction
- Open reduction + femoral shortening osteotomy + possible acetabular osteotomy
3-8 Years - Acetabular Osteotomy
Options: Salter, Dega, Pemberton, or Staheli procedure
>8 Years (>6 years for bilateral)
- Triradiate cartilage still open: Triple (Steele) or Double pelvic (Sutherland) osteotomy, Staheli procedure
- Triradiate closed: Ganz periacetabular osteotomy (PAO) or Chiari osteotomy
- Reduction after age 8 is controversial (acetabulum has limited remodeling potential)
- Total hip arthroplasty eventually as an adult
Specific Osteotomies
| Procedure | Type | Key Feature |
|---|---|---|
| Salter | Redirectional | May lengthen limb up to 1 cm; triradiate must be open |
| Pemberton | Volume-reducing | Bends on triradiate cartilage; good for residual dysplasia |
| Dega | Volume-reducing | Favored for paralytic dislocations, posterior deficiency |
| Ganz (PAO) | Redirectional | 3D correction; triradiate must be closed; single incision; allows joint inspection |
| Chiari | Salvage | Medial displacement osteotomy; for older/congruent joint |
| Staheli (shelf) | Salvage/augmentation | Adds bony coverage |
Complications
- Avascular necrosis (AVN) of femoral head - the most feared complication of both closed and open reduction; caused by vascular injury (medial femoral circumflex artery) or excessive abduction in the harness
- Redislocation after reduction
- Residual dysplasia requiring later osteotomy
- Femoral nerve palsy - from excessive flexion in Pavlik harness (transient)
- Failure of open reduction - very difficult to salvage (50% osteonecrosis rate on revision)
Key memory aids:
-
Risk factors: "Big Fat FirstBorn" = Breech, Female, Family history, FirstBorn
-
Ortolani = Out → In (reduces the dislocated hip)
-
Barlow = Bad test → can dislocate the hip
-
Left hip > right (LOA position in utero)
-
Miller's Review of Orthopaedics, 9th Ed., pp. 264-268
-
Campbell's Operative Orthopaedics, 15th Ed. 2026, pp. 1403-1410
Ctev from Maheshwari
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Loading Image
Finding Sources
I now have all the content needed for a comprehensive answer. Let me compile it.
CTEV (Congenital Talipes Equinovarus) - Clubfoot
(Maheshwari's "Essential Orthopaedics" is not in the available library catalog. The content below is drawn from Miller's Review of Orthopaedics, 9th Ed. and Campbell's Operative Orthopaedics, 15th Ed. - the same standard material Maheshwari covers.)
Definition
CTEV is a complex three-dimensional congenital foot deformity characterized by four fixed positional abnormalities, remembered by the mnemonic:
C-A-V-E
- C - Cavus (high arch / plantar flexion of forefoot)
- A - Adduction of forefoot
- V - Varus of hindfoot
- E - Equinus (plantar flexion of ankle)
This same sequence (CAVE) is also the order of correction in the Ponseti method.
Epidemiology
| Feature | Detail |
|---|---|
| Incidence | ~1 in 1000 live births |
| Sex | Boys affected twice as often as girls |
| Bilaterality | 50% of cases are bilateral |
| Left vs. right | Equal when bilateral; left more common unilaterally |
Etiology / Causes
- Majority are idiopathic - but a strong genetic basis is suspected
- Genetic pathway: PITX1-TBX4 transcriptional pathway implicated
- Associated syndromic causes:
- Arthrogryposis multiplex congenita
- Myelomeningocele (spina bifida)
- Diastrophic dwarfism
- Streeter dysplasia (congenital constriction band syndrome)
- Prune-belly syndrome
- Tibial hemimelia
- Other neuromuscular conditions
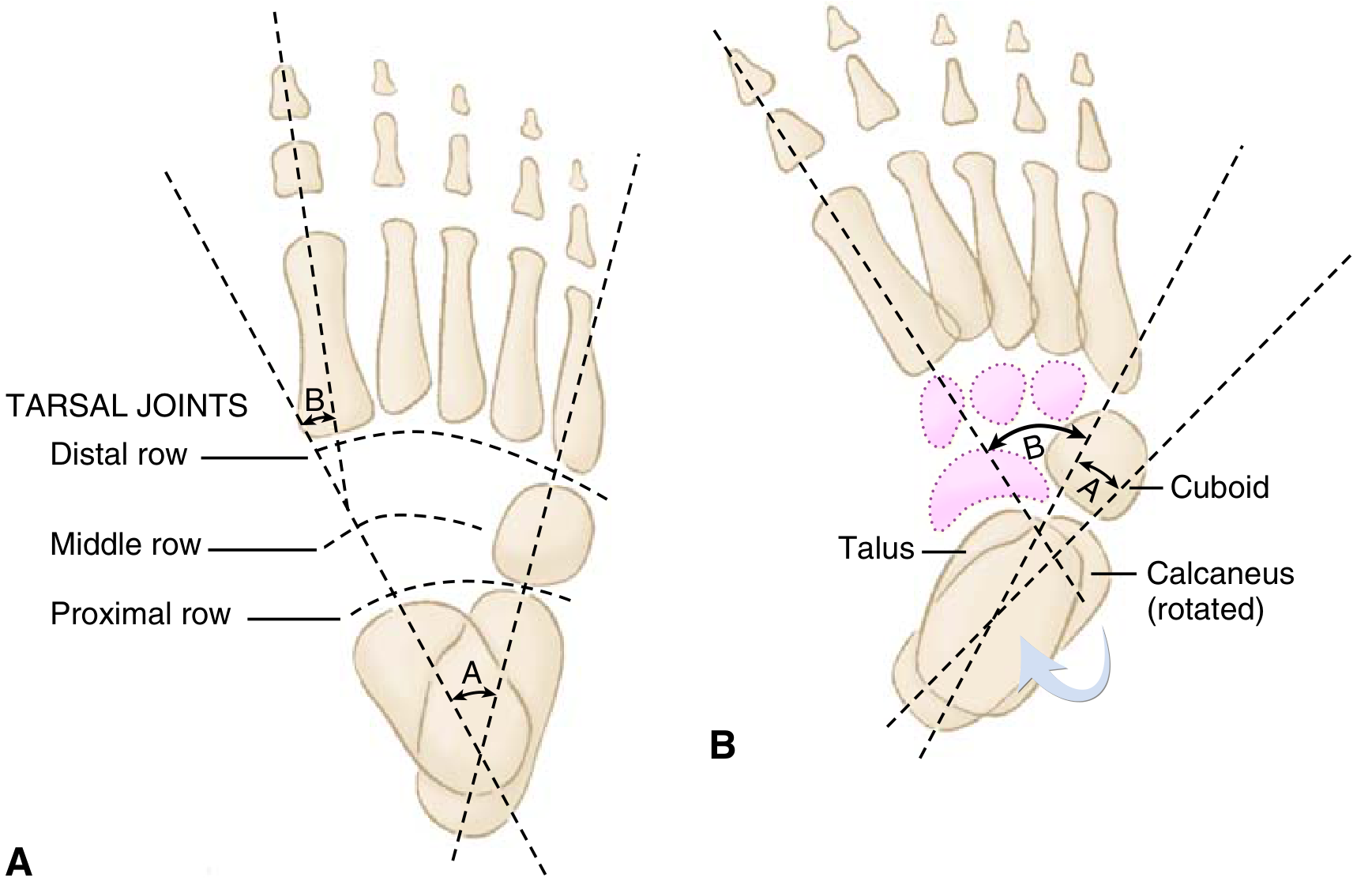
Pathological Anatomy
The primary bony abnormality is medial and plantar deviation of the talar neck, with:
- Medial rotation of calcaneus under the talus
- Medial displacement of navicular (towards medial malleolus)
- Medial displacement of cuboid
Secondary soft tissue changes drive the deformity:
- Shortening and contracture of:
- Tibialis posterior
- Achilles tendon
- Flexor hallucis longus (FHL)
- Flexor digitorum longus (FDL)
- Intrinsic foot muscles
- Medial and posterior joint capsules and ligaments
- Plantar fascia
The diagram below shows the radiographic appearance - note "parallelism" of talus and calcaneus in clubfoot vs. the normal divergent relationship:
- Absence or diminutive anterior tibial artery is also associated
Clinical Features
On examination, the foot shows:
- Plantar flexion of the ankle (equinus)
- Heel in varus
- Forefoot adducted and supinated
- High arch (cavus)
- Calf wasting and a smaller, shorter foot on the affected side
- Skin creases on medial side and posterior heel
Scoring / Classification
Pirani Score (most common clinical scoring system):
- 6 clinical signs scored 0, 0.5, or 1
- Max score = 6 (most severe)
- Divided into midfoot score (3 signs) and hindfoot score (3 signs)
Dimeglio Classification: Grades clubfoot I-IV based on reducibility and stiffness; predicts difficulty during Ponseti casting.
Radiological Findings
(Radiographs rarely used in infants due to minimal ossification; used more in older children)
| View | Measurement | Normal | Clubfoot |
|---|---|---|---|
| AP (Kite's angle) | Talocalcaneal (TC) angle | 20-40° | <20° (parallelism) |
| Lateral (Turco) | Talocalcaneal angle | ~35° | <35° |
| AP | Talus-1st metatarsal angle | 0-20° (positive) | Negative |
| AP | Talo-calcaneal angle | Divergent | Parallel |
Key sign: Parallelism of talus and calcaneus on both AP and lateral views (normally they diverge).
Treatment
1. Ponseti Method (Gold Standard - First Line)
Serial weekly manipulation and long-leg plaster casting correcting deformities in the CAVE sequence:
| Cast | Correction |
|---|---|
| 1st cast | Corrects Cavus - supinating forefoot, dorsiflexing 1st ray |
| 2nd-4th casts | Correct Adductus + Varus - lateral pressure on distal talar head as fulcrum; foot externally rotated |
| Final cast | Placed in 70° of abduction |
| After casting | Percutaneous Achilles tenotomy (in ~90% of cases) for equinus |
Foot Abduction Brace (Dennis-Browne Splint):
- Imperative after casting - most common cause of recurrence is brace non-compliance
- Full time for 3 months, then nights and naps for 3 years
- Set at 60-70° of external rotation (affected side) and 40-45° (normal side)
2. French (Functional) Physiotherapy Method
- Daily stretching, manipulation, and taping followed by splinting
- Used less commonly; popular in France
3. Operative Treatment
Indications: Only ~5% of idiopathic clubfeet require surgery (resistant/refractory cases or recurrence after adequate conservative treatment)
Posteromedial Release (PMR):
- Cincinnati incision (circumferential posterior incision)
- Structures released:
- Achilles tendon lengthening (Z-plasty)
- Posterior ankle and subtalar joint capsulotomy
- Tibiotalar and talonavicular release
- Tibialis posterior, FHL, FDL lengthening
- Plantar fascia release
- Must protect the posterior tibial artery (dorsalis pedis often insufficient in clubfoot)
In Older Children (3-10 years) for residual adductus:
- Medial opening-wedge osteotomy
- Lateral column-shortening osteotomy (cuboid decancellation / Evans procedure)
For Late-presenting / Severe/Neglected Clubfoot:
- Triple arthrodesis (subtalar + talonavicular + calcaneocuboid joints) in older children
- Contraindicated in insensate feet (risk of ulceration due to rigidity)
Ilizarov frame: For very severe neglected cases
Complications
| Complication | Cause / Notes |
|---|---|
| Recurrence | Most common; strongly associated with brace non-compliance |
| Rocker-bottom deformity | Attempt to dorsiflex hindfoot before varus corrected |
| Flat-top talus | Aggressive dorsiflexion flattens talar dome |
| Avascular necrosis of talus | Excessive vascular disruption during surgery |
| Dynamic supination | Overpull of tibialis anterior; weak peroneus longus; in 15-20% post-treatment |
| Dorsal bunion | Post-surgery; tibialis anterior + flexor hallucis brevis overpull |
| Residual varus | Undercorrection |
| Overlength/stiffness | Over-aggressive PMR |
Treatment of Complications
| Complication | Management |
|---|---|
| Recurrence | Trial of recasting first; then surgery if refractory |
| Dynamic supination | Transfer of tibialis anterior tendon laterally (to 3rd cuneiform) |
| Dorsal bunion | Capsulotomy + FHL lengthening + FHB transfer to MTP extensor |
| Flat-top talus | Talectomy as salvage |
Key Memory Points
-
CAVE = deformities + order of correction
-
Boys : Girls = 2:1, Bilateral = 50%
-
Ponseti = CAVE correction sequence → 90% need Achilles tenotomy → Brace 3 years
-
Brace non-compliance = #1 cause of recurrence
-
Surgery needed in only 5% of idiopathic cases
-
Radiograph hallmark = parallelism of talus and calcaneus (TC angle <20° on AP)
-
Protect posterior tibial artery during PMR surgery
-
Miller's Review of Orthopaedics, 9th Ed., pp. 282-283
-
Campbell's Operative Orthopaedics, 15th Ed. 2026
What is kites method and what was the drawback?
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
Kite method clubfoot casting drawback calcaneocuboid fulcrum vs Ponseti
Excellent - the web search confirms the key information clearly. I now have a complete picture to answer this well.
Kite's Method of Clubfoot Treatment
What is Kite's Method?
Kite's method (described by Dr. Hiram Kite, 1930s-1950s) was the traditional serial casting technique for CTEV that preceded the Ponseti method and was widely used for several decades.
Technique:
- Serial plaster of Paris casts applied with manipulation
- The foot was abducted to correct adductus by applying pressure over the calcaneocuboid (CC) joint as the fulcrum
- The heel (calcaneus) was held firmly while the forefoot was swung laterally
- Equinus was corrected last, as in most methods
- Required a large number of casts over many months
Kite's Angle:
Kite also described the talocalcaneal (TC) angle on AP radiograph (also called Kite's angle), which is normally 20-40° and is reduced (parallelism) in clubfoot. This measurement remains clinically relevant today.
The Drawback - "Kite's Error"
This is the central flaw and is now specifically named "Kite's Error" in modern orthopaedic literature.
The Error:
When correcting adductus, Kite used the calcaneocuboid joint as the fulcrum - meaning he applied counter-pressure over the lateral aspect of the foot at the calcaneocuboid joint while abducting the forefoot.
Why This Is Wrong - The Biomechanical Explanation:
The subtalar joint operates through kinematic coupling - the calcaneus, talus, and navicular all move together as a linked unit. When you abduct the foot:
-
If pressure is applied over the calcaneocuboid joint (Kite's fulcrum) → this locks and blocks the calcaneocuboid joint → the kinematic coupling of the subtalar joint is blocked → heel varus CANNOT be corrected - the calcaneus remains locked in varus beneath the talus
-
If pressure is applied over the distal talar head (Ponseti's fulcrum) → the talar head acts as a pivot → the calcaneus is free to evert, abduct, and derotate under the talus → heel varus corrects simultaneously with forefoot adductus
In simple terms:
| Kite's Method | Ponseti's Method | |
|---|---|---|
| Fulcrum point | Calcaneocuboid joint | Lateral distal talar head |
| Effect on subtalar joint | Blocks correction | Allows correction |
| Heel varus | Persists / uncorrected | Corrects simultaneously |
| Result | Apparent forefoot correction only (midfoot break) | True correction of all components |
Consequence of Kite's Error:
- The forefoot appeared corrected but the hindfoot varus remained
- This created a "bean-shaped" foot or false correction - the midfoot broke rather than the subtalar joint correcting
- Led to high rates of residual deformity, recurrence, and ultimately more surgery
- Required many more casts (often 8-16) compared to Ponseti (average 5-6)
- Lower maximum dorsiflexion achieved at the ankle
- Higher surgical intervention rates
Kite vs. Ponseti - Summary Comparison
| Parameter | Kite's Method | Ponseti Method |
|---|---|---|
| Fulcrum | Calcaneocuboid joint | Distal talar head |
| Number of casts | Many (8-16+) | Fewer (~5-6) |
| Duration | Longer | Shorter |
| Ankle dorsiflexion achieved | Less | Greater |
| Recurrence rate | Higher | Lower |
| Surgery rate | Higher | ~5-10% (mostly tenotomy only) |
| Pathological anatomy understood | Incomplete | Correctly identified |
Key Teaching Point
Kite's error = applying pressure over the calcaneocuboid joint while correcting adductus, which blocks subtalar joint correction and prevents the calcaneus from derotating under the talus. This is why Ponseti specifically taught to use the lateral talar head as the fulcrum, keeping the CC joint free.
This is also listed in modern literature as a common technical error when practitioners incorrectly mix Kite's technique into the Ponseti method - it is specifically warned against during Ponseti training.
- Miller's Review of Orthopaedics, 9th Ed. (Kite's angle, p. 282)
- MDPI systematic review on Ponseti vs. Kite
- Common errors in clubfoot management - MDPI
This is a shared conversation. Sign in to Orris to start your own chat.