ovarian malignancy survivor
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ovarian cancer" AND "survivorship"
Finding Sources
Finding Sources
Finding Sources
Searching the Web
ovarian cancer survivor follow-up guidelines 2024 surveillance recurrence
Finding Sources
Reading Web Page
https://pmc.ncbi.nlm.nih.gov/articles/PMC10891493
Finding Sources
Finding Sources
Reading File
Reading File
Loading Image
Finding Sources
Here is a thorough overview of ovarian malignancy survivorship - covering surveillance, recurrence risk, long-term effects of treatment, and quality of life.
Ovarian Malignancy Survivorship
1. Epidemiology & Context
Ovarian cancer is the second most common gynecologic malignancy in the United States but accounts for the majority of gynecologic cancer deaths, with ~22,280 new cases and ~14,240 deaths per year. Over two-thirds of patients present with advanced disease (Stage III-IV), which defines much of the survivorship landscape. - Berek & Novak's Gynecology
2. Prognosis by Stage (5-Year Survival)
The figure below shows Kaplan-Meier survival curves by stage from a large international dataset:
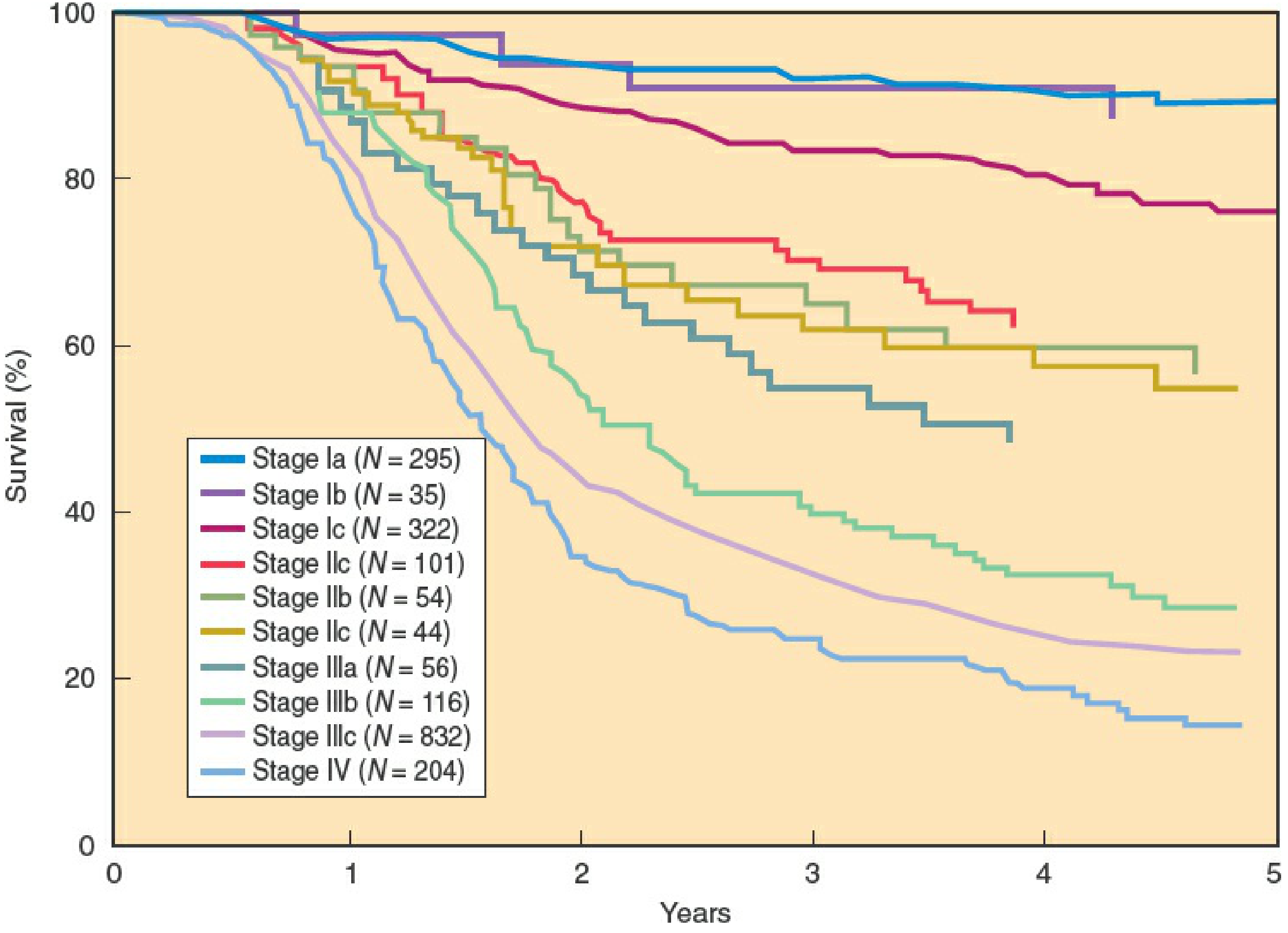
| Stage | 5-Year Survival |
|---|---|
| Stage I | ~93-94% |
| Stage II | ~70-73% |
| Stage III | ~23-37% (varies by residual disease) |
| Stage IV | ~11-25% |
| Borderline tumors | ~86-90% (all stages); Stage I = 98% at 15 years |
For Stage III specifically, patients with microscopic residual disease at the start of treatment achieve 40-75% 5-year survival, compared to only ~5% for suboptimal debulking. - Berek & Novak's Gynecology, p. 2374
3. Post-Treatment Surveillance
Clinical Follow-Up Schedule (standard practice)
- Years 1-2: Every 2-4 months
- Years 3-5: Every 6 months
- Beyond 5 years: Annually
What to Monitor
- CA-125 (Cancer Antigen 125): The primary serum tumor marker for detecting recurrence and monitoring therapy response. Serial CA-125 is used to track treatment response and identify early relapse. A rising CA-125 during remission often precedes clinical recurrence by weeks to months. - Tietz Textbook of Laboratory Medicine, 7th Ed.
- Clinical examination: Pelvic exam at each visit
- Imaging (CT/ultrasound): CT is the primary modality for staging, surgical planning, and follow-up; used when symptoms arise or CA-125 rises. Annual surveillance imaging in asymptomatic patients has not been shown to improve survival. - Grainger & Allison's Diagnostic Radiology
- Symptom review: Bloating, pelvic pain, urinary symptoms, bowel changes
Note: Routine early detection of asymptomatic recurrence via CA-125 alone has not been shown to improve overall survival compared to treating at symptomatic recurrence (the MRC OV05 trial findings). Current evidence favors a patient-centered approach based on clinical symptoms and rising CA-125.
4. Recurrence - Risk and Management
- Most recurrences (70-80%) occur within 2 years of completing primary treatment.
- Platinum-sensitive recurrence (relapse >6 months after platinum chemotherapy): retreatable with platinum-based regimens; better prognosis.
- Platinum-resistant recurrence (relapse within 6 months): treated with non-platinum agents (liposomal doxorubicin, gemcitabine, topotecan, weekly paclitaxel).
PARP Inhibitors in Survivorship
A major development in recent years is maintenance therapy after response to platinum-based chemotherapy:
- Olaparib and niraparib are FDA-approved for maintenance in platinum-sensitive disease
- Significantly improve progression-free survival (PFS), especially in patients with BRCA1/2 mutations (germline or somatic)
- Benefit observed regardless of BRCA status, but greatest in BRCA mutation carriers
- Rucaparib also showed PFS benefit in platinum-sensitive recurrent disease
- Berek & Novak's Gynecology, Key Points 11
All patients should undergo BRCA1/2 genetic testing (germline +/- somatic) as it directly affects maintenance therapy decisions and family counseling.
5. Long-Term Treatment Effects
From Surgery
- Surgical menopause (if bilateral oophorectomy, especially in premenopausal women): hot flashes, vaginal dryness, dyspareunia, osteoporosis risk, cardiovascular risk
- Bowel/bladder changes from cytoreductive surgery: adhesions, obstruction, altered bowel habits
- Lymphedema (if lymph node dissection performed)
From Chemotherapy (Carboplatin + Paclitaxel)
- Peripheral neuropathy (paclitaxel): often the most persistent long-term toxicity; numbness and tingling in hands and feet
- Ototoxicity and nephrotoxicity (cisplatin-containing regimens)
- Fatigue: Commonly persists months to years post-treatment
- Cognitive changes ("chemo brain"): Memory, concentration difficulties
- Bone marrow suppression during treatment; risk of secondary myeloid malignancies (rare, but elevated)
- Alopecia: Usually reversible
From PARP Inhibitors (maintenance)
- Nausea, fatigue, anemia, thrombocytopenia (especially early on)
- Risk of treatment-emergent myelodysplastic syndrome (MDS) or acute myeloid leukemia (AML) - rare but recognized
6. Fertility and Hormonal Considerations
- Bilateral oophorectomy results in premature surgical menopause with abrupt estrogen loss. Hormone replacement therapy (HRT) is generally considered safe in epithelial ovarian cancer survivors (non-hormone-sensitive subtypes), but decisions must be individualized.
- Fertility-sparing surgery (unilateral salpingo-oophorectomy) is an option for selected young patients with Stage IA, Grade 1-2 epithelial tumors, or germ cell tumors. The uterus and contralateral ovary are preserved.
- Germ cell tumors and sex cord-stromal tumors: fertility preservation is the standard approach in most young patients. - Berek & Novak's Gynecology, Key Point 13
7. Psychosocial and Quality of Life
Evidence consistently shows significant psychological burden in ovarian cancer survivors:
- Recurrence anxiety is among the most commonly reported impairments to well-being - given that most patients do relapse, the uncertainty is real and persistent
- Depression: Risk remains elevated for years post-treatment; a register-based cohort study with up to 19 years of follow-up found increased depression risk persisting long-term
- Sexual dysfunction: Dyspareunia, decreased libido, and vaginal changes are common, amplified by surgical menopause
- Social and relational impacts: Caregiver burden, relationship strain, social isolation
- A 2024 systematic review on psychosocial interventions for ovarian cancer survivors identified cognitive-behavioral therapy, mindfulness, and peer support as beneficial interventions
Supporting Evidence (Recent)
- Post-diagnosis physical activity is associated with improved mortality outcomes in gynecologic cancer survivors (Meta-Analysis, 2026, PMID 42400650)
- Exercise interventions show benefit for quality of life but evidence base remains heterogeneous (Systematic Review, 2025, PMID 39721835)
8. Survivorship Care Plan Essentials
A comprehensive survivorship care plan for ovarian cancer patients should address:
- Treatment summary (surgical staging, chemo regimen, maintenance therapy)
- Surveillance schedule (CA-125, exam intervals, imaging triggers)
- Genetic testing results and implications for family members
- Long-term side effect management (neuropathy, menopause, fatigue)
- Mental health and psychosocial support referrals
- Lifestyle recommendations: weight management, physical activity (improves QOL and survival), smoking cessation
- Sexual health counseling and referral (vaginal moisturizers, pelvic floor PT, HRT if appropriate)
- Second primary cancer screening (endometrial, breast - especially in BRCA carriers)
Key takeaway: Ovarian cancer survivorship is shaped by the high recurrence rate, the shift toward PARP inhibitor maintenance therapy, and the substantial long-term physical and psychological effects of treatment. Ongoing oncology follow-up is standard, and a proactive, patient-centered approach to quality of life is as important as tumor surveillance.
This is a shared conversation. Sign in to Orris to start your own chat.