Generate me an eg for brachial example
Asking for Preferences
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Here is a complete clinical example of the Brachial Plexus, drawn from Gray's Anatomy for Students, S. Das Manual on Clinical Surgery, and the Harriet Lane Handbook.
Brachial Plexus - Structure & Clinical Examples
Anatomy at a Glance
The brachial plexus is formed by the anterior rami of C5-C8 and T1. It originates in the neck, passes over rib I, and enters the axilla. Its parts from medial to lateral are:
| Level | Components |
|---|---|
| Roots | C5, C6, C7, C8, T1 (anterior rami) |
| Trunks | Superior (C5+C6), Middle (C7), Inferior (C8+T1) |
| Divisions | Each trunk splits into anterior + posterior |
| Cords | Lateral, Medial, Posterior (named by position relative to axillary artery) |
| Terminal nerves | Musculocutaneous, Median, Radial, Ulnar, Axillary |
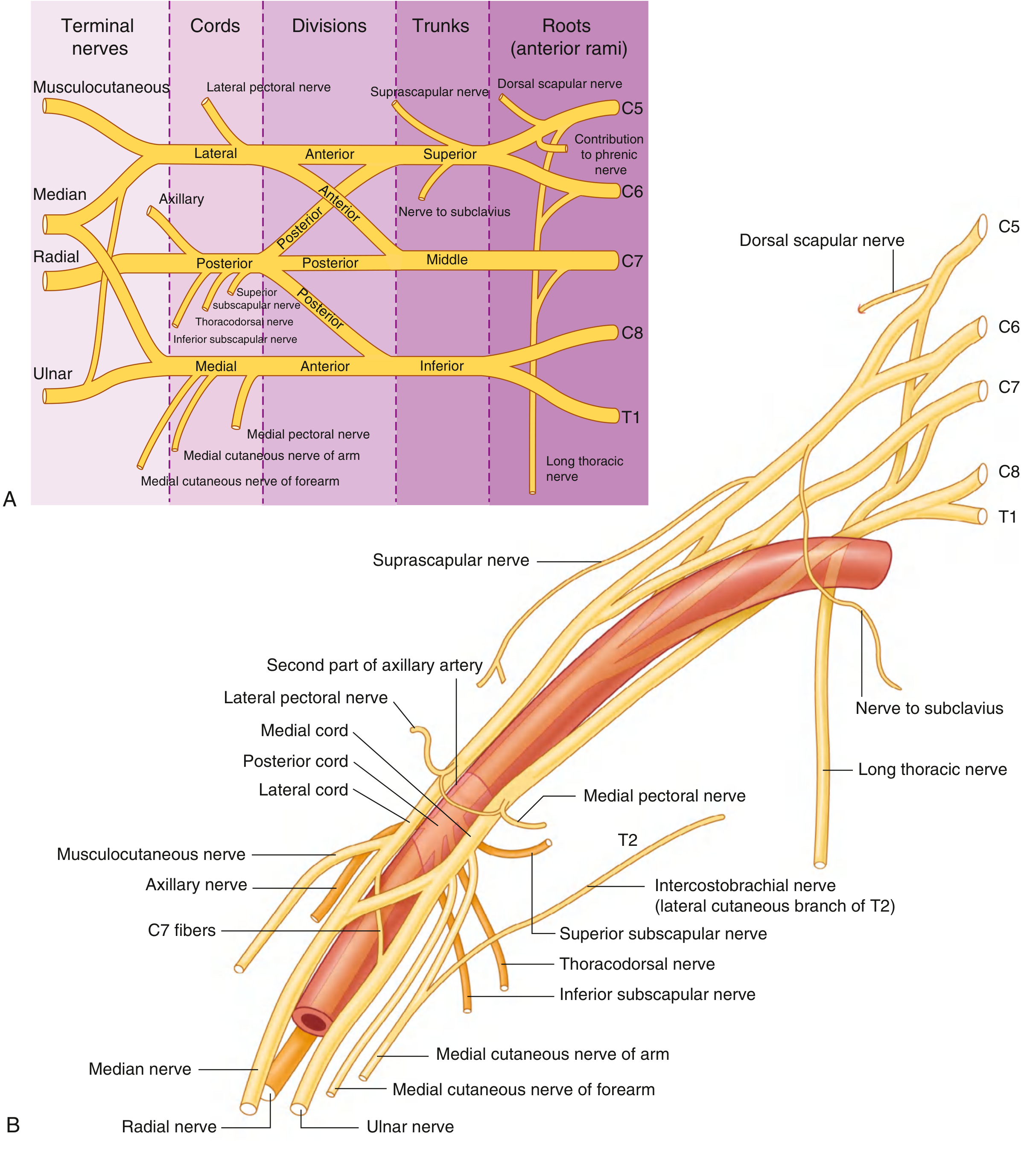
Fig. 7.53 - Brachial Plexus: (A) Schematic showing branches, (B) Relationships to the axillary artery - Gray's Anatomy for Students
Clinical Example 1: Erb-Duchenne Palsy (Upper Brachial Plexus Injury)
Roots injured: C5 and C6
Mechanism:
- Adult: fall of weight on shoulder, motorcycle accident (head forcefully moved away from shoulder)
- Neonate: difficult labour - angle between shoulder and neck is forced open
Muscles paralysed: Deltoid, biceps, brachialis, brachioradialis, supinator
Classic posture - "Policeman taking a tip" / "Waiter's tip" deformity:
- Arm: adducted, internally rotated
- Elbow: extended
- Forearm: pronated
- Wrist: flexed
Sensory loss: Outer arm and upper lateral forearm
Prognosis: Best prognosis of all brachial plexus injuries; accounts for ~90% of birth-related cases.
Clinical Example 2: Klumpke's Palsy (Lower Brachial Plexus Injury)
Roots injured: C8 and T1
Mechanism:
- Forceful hyperabduction of the shoulder (e.g., breech delivery with arms above head, a person falling and grabbing onto an object overhead)
Muscles paralysed: Intrinsic muscles of the hand (interossei, lumbricals, thenar, hypothenar)
Clinical findings:
- Claw hand (hyperextension at MCPs, flexion at IPs)
- Features of combined median + ulnar nerve palsy
- Sensory loss: medial forearm, hand, and inner 1.5 fingers
Associated finding - Horner's syndrome (if T1 root is avulsed):
- Ptosis (drooping eyelid)
- Enophthalmos (sunken eye)
- Miosis (constricted pupil)
- Anhidrosis (no sweating on ipsilateral face)
Prognosis: Poor; less than 2% of birth brachial plexus cases.
Summary Table (from Harriet Lane Handbook)
| Injury | Roots | Clinical Features | Prognosis |
|---|---|---|---|
| Erb-Duchenne | C5-C6 (±C4) | Adduction + internal rotation arm; forearm pronated; wrist flexed | Best (90% of cases) |
| Total palsy | C5-T1 (±C4) | Entire arm involved; Horner syndrome if T1 | Intermediate (8-9%) |
| Klumpke | C7-T1 | Flaccid hand; Horner syndrome if T1 | Worst (<2%) |
Memory Aid
- ERB = Upper (C5-C6) = "wAITER's tip" - arm hangs limp in internal rotation, looks like a waiter asking for a tip
- KLUMPKE = Lower (C8-T1) = "CLAW hand" - intrinsic hand muscles lost + Horner's syndrome
Sources: Gray's Anatomy for Students, p. 858-859 | S. Das Manual on Clinical Surgery, 13th Ed., p. 140 | Harriet Lane Handbook, 23rd Ed.
This is a shared conversation. Sign in to Orris to start your own chat.