

IMG_1527.jpg
IMG_1530.jpg
39 year old female TAH+BSO done for subserous fibroid posterior wall of uterus. Sections from left ovary. Is this choriocarcinoma explain each cell types
analyse_media
analyse_media
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the information needed for a thorough, well-referenced answer. Let me compose it.
Yes - These Sections Are Consistent with Choriocarcinoma of the Ovary
Both slides show the classic histological features of non-gestational (primary) ovarian choriocarcinoma - a malignant germ cell tumor. Here is a systematic breakdown.
Low-Power View (IMG_1527) - Architectural Features
What you see:
- A highly disorganized, destructive growth pattern with no chorionic villi - this is the single most important low-power finding. Villi are absent in choriocarcinoma, distinguishing it from hydatidiform mole.
- Extensive lakes of hemorrhage interspersed between cords and nests of atypical cells. This hemorrhagic pattern reflects direct vascular invasion by tumor cells that erode host blood vessels without forming a fibrovascular stroma.
- A plexiform/anastomosing pattern: sheets and cords of tumor cells wrap around blood-filled spaces.
- On the left margin, fibromuscular wall (ovarian capsule) is being invaded by the tumor.
- Absence of intrinsic stroma: the tumor nests have no internal supporting connective tissue - cells depend entirely on invaded host vessels for nutrients.
- Coagulative necrosis: amorphous eosinophilic debris in areas away from viable tumor cells, typical of rapidly growing malignancies.
This low-power architecture is exactly what Robbins & Kumar Pathologic Basis of Disease describes: "a soft, fleshy tumor with large pale areas of necrosis and extensive hemorrhage... histologically consists of proliferating syncytiotrophoblasts and cytotrophoblasts; chorionic villi are absent."
High-Power View (IMG_1530) - The Two Cell Types
Choriocarcinoma is defined by a dimorphic (biphasic) trophoblastic cell population. Both cell types are clearly visible.
1. Cytotrophoblasts (CT)
| Feature | What you see in IMG_1530 |
|---|---|
| Cell shape | Polygonal to rounded, relatively distinct cell borders |
| Nucleus | Single large, vesicular nucleus; prominent nucleoli |
| Chromatin | Coarse, hyperchromatic but with some openness |
| Cytoplasm | Clear to pale eosinophilic, well-defined borders |
| Mitoses | Abundant, sometimes atypical |
| Arrangement | Cohesive nests and clusters; form the "inner" layer |
Biology: Cytotrophoblasts are the proliferative, stem-like trophoblast. They are the mononuclear component and represent the cycling population of the tumor. They are the precursors that give rise to syncytiotrophoblasts. In the placenta, cytotrophoblasts correspond to Langhans layer.
2. Syncytiotrophoblasts (ST)
| Feature | What you see in IMG_1530 |
|---|---|
| Cell shape | Large, irregular, smudged-border giant cells |
| Nuclei | Multiple (3-30) hyperchromatic nuclei within shared cytoplasm; nuclei are crowded, overlapping, pleomorphic |
| Cytoplasm | Voluminous, deeply eosinophilic to amphophilic; irregular/branching outer border |
| Arrangement | Wrap around and cap the cytotrophoblast nests; "peripheral" position |
| Function | Secrete hCG - hence why serum hCG is markedly elevated |
Biology: Syncytiotrophoblasts are the non-dividing, differentiated component. They do not undergo mitosis themselves. They are the hCG-secreting cells and in normal placenta they form the outer syncytial layer covering the villi. Their irregular "smudged" borders in the image reflect cytoplasmic fusion and loss of cell membranes.
The Classic Dimorphic Pattern - The Diagnostic Key
The intimate association of these two cell types - the pale mononuclear cytotrophoblasts capped and surrounded by the dark multinucleated syncytiotrophoblasts - is pathognomonic. As Robbins & Kumar Basic Pathology states: "composed of anaplastic cuboidal cytotrophoblasts and syncytiotrophoblasts... mitoses are abundant and sometimes abnormal."
Why This Is Ovarian Choriocarcinoma (Not Gestational/Metastatic)
| Feature | This Case |
|---|---|
| Patient age | 39 years (within range for non-gestational) |
| Primary surgery | TAH+BSO for fibroid - ovaries removed; tumor found in left ovary |
| No history of pregnancy/mole mentioned | Supports primary ovarian (non-gestational) origin |
| Architecture | No villi - rules out mole; biphasic trophoblastic cells confirm choriocarcinoma |
Robbins notes: "Most ovarian choriocarcinomas exist in combination with other germ cell tumors, and pure ovarian choriocarcinoma is extremely rare. They are histologically identical to the more common placental lesions... aggressive and have usually metastasized hematogenously to lungs, liver, bone by the time of diagnosis."
Important note: Gestational choriocarcinoma metastatic to the ovary must also be considered in the differential. Distinction requires molecular analysis (paternal DNA in gestational type is absent in non-gestational). This is clinically important because gestational choriocarcinoma responds dramatically to chemotherapy (near 100% cure), while non-gestational ovarian choriocarcinoma has a poorer prognosis and is relatively chemoresistant.
Key Ancillary Tests to Order
- Serum beta-hCG - markedly elevated (secreted by syncytiotrophoblasts); critical for monitoring
- IHC panel:
- hCG - diffuse positivity in syncytiotrophoblasts
- CK (AE1/AE3) - positive in both cell types
- PLAP - may be positive
- Inhibin - negative (helps rule out sex cord-stromal tumor)
- EMA - positive
- Molecular/genotyping - to distinguish gestational (paternal alleles present) vs. non-gestational (no paternal contribution) - this changes prognosis and treatment
Reference Images from Textbook for Comparison
Here is the classic choriocarcinoma histology from Robbins & Kumar for comparison - note the identical dimorphic pattern with cytotrophoblasts (left) and syncytiotrophoblasts (arrows, right):
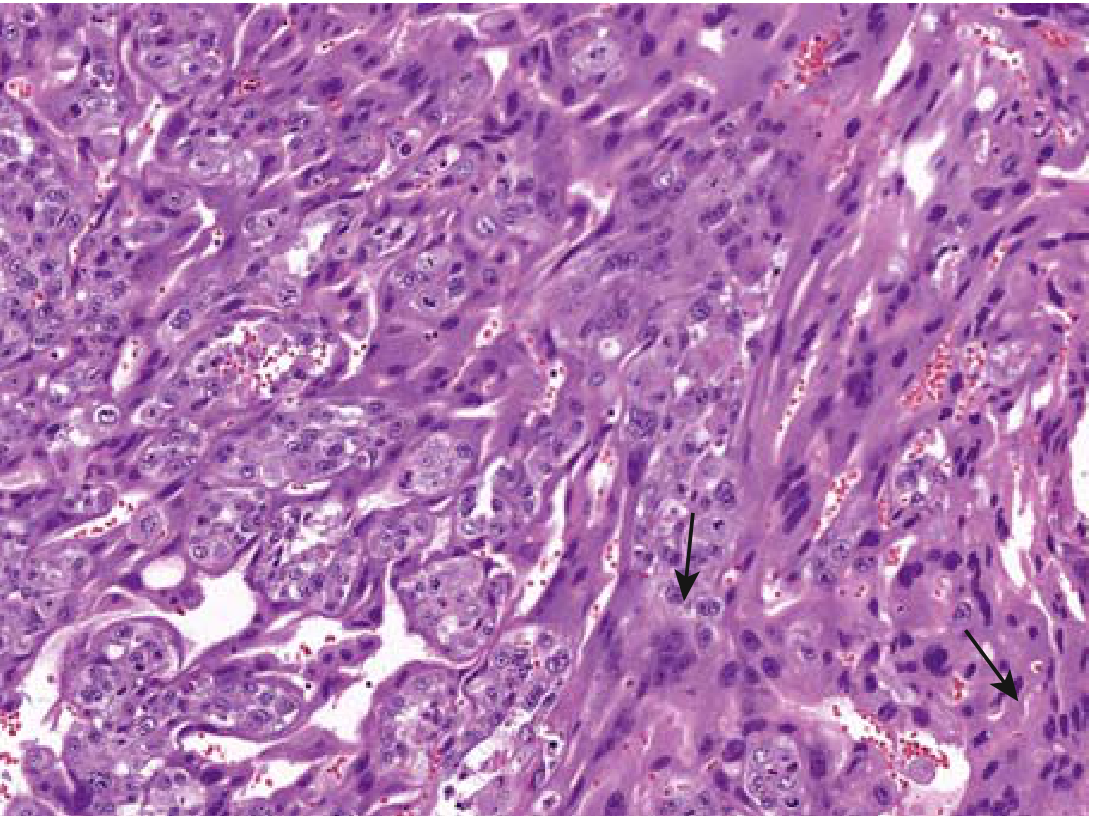
FIG. 17.22 from Robbins & Kumar Basic Pathology - Choriocarcinoma showing both neoplastic cytotrophoblast and multinucleate syncytiotrophoblast (arrows)
Summary
Yes, this is choriocarcinoma. The histological diagnosis rests on:
- Biphasic trophoblastic differentiation - cytotrophoblasts + syncytiotrophoblasts
- Absence of chorionic villi
- Extensive hemorrhage and necrosis
- Destructive, invasive growth without intrinsic stroma
- Abundant mitoses with nuclear pleomorphism
Given the clinical context (39F, specimen from left ovary during TAH+BSO for fibroid), this most likely represents primary non-gestational choriocarcinoma of the ovary, though gestational origin cannot be excluded without serum hCG history and molecular studies. Urgent oncology referral, serum hCG, and staging CT are the immediate next steps.
Teach me choriocarcinoma ovary
Finding Sources
Finding Sources
Searching PubMed
"choriocarcinoma" AND "ovary" AND "nongestational"
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Loading Image
I now have everything needed for a comprehensive teaching session. Here is the full lesson:
🎓 Choriocarcinoma of the Ovary - Complete Teaching Note
1. INTRODUCTION & CLASSIFICATION
Choriocarcinoma of the ovary fits within the Malignant Germ Cell Tumors (MGCT) category. Germ cell tumors arise from primordial germ cells of the ovary and constitute 15-20% of all ovarian tumors. Most are benign (mature teratomas); malignant types dominate in young females and children.
Where does choriocarcinoma fit?
Ovarian Germ Cell Tumors
├── Dysgerminoma (most common malignant GCT)
├── Yolk Sac Tumor (Endodermal Sinus Tumor) → AFP
├── Immature Teratoma
├── Choriocarcinoma ← we are here → hCG
├── Embryonal Carcinoma
├── Polyembryoma
└── Mixed Germ Cell Tumor
Germ cell tumors show differentiation toward:
- Oogonia → Dysgerminoma
- Extraembryonic yolk sac → Yolk sac tumor
- Placental tissue → Choriocarcinoma
- Multiple germ layers → Teratoma
(Robbins, Cotran & Kumar - Pathologic Basis of Disease)
2. THE TWO TYPES OF OVARIAN CHORIOCARCINOMA
This is a fundamental concept - there are two completely different diseases with the same histology:
| Feature | Gestational (Secondary) | Non-Gestational (Primary) |
|---|---|---|
| Origin | Trophoblastic cells from a prior pregnancy (mole, abortion, normal pregnancy) | Malignant germ cells in the ovary differentiating into trophoblast |
| DNA content | Contains paternal DNA (foreign) | No paternal DNA - only maternal |
| Detection | Molecular genotyping (STR analysis) | Same |
| Age | Any reproductive age | Usually < 20 years (most < 10 years for pure type) |
| Chemosensitivity | Remarkable - near 100% cure with EMA-CO/methotrexate | Poor - relatively chemoresistant |
| Prognosis | Excellent even with metastases | Poor; most have metastases at diagnosis |
| Why difference? | Tumor is antigenically foreign (paternal antigens) - immunologically targetable | Autologous - no immune recognition advantage |
The distinction matters enormously: misclassifying a gestational choriocarcinoma as non-gestational would deny the patient a near-curative treatment.
3. INCIDENCE & EPIDEMIOLOGY
- Pure non-gestational ovarian choriocarcinoma is extremely rare - only a few hundred cases in world literature
- Most "ovarian choriocarcinomas" are actually metastases from uterine/gestational choriocarcinoma, or occur as a component of a mixed germ cell tumor
- In mixed germ cell tumors, choriocarcinoma is found in ~20% of cases (combined with dysgerminoma, EST, immature teratoma)
- Pure form: typically presents in girls < 20 years, often pre-menarchal
- Age of your case (39F): relatively unusual for pure primary - needs gestational origin exclusion
(Berek & Novak's Gynecology)
4. PATHOGENESIS
Primordial Germ Cell
↓
Malignant transformation
↓
Differentiates along trophoblastic/extraembryonic pathway
↓
Produces BOTH cytotrophoblasts AND syncytiotrophoblasts
↓
Syncytiotrophoblasts secrete β-hCG
↓
Elevated serum hCG → clinical features
The tumor directly invades and erodes blood vessels without forming a fibrovascular stroma - this is the mechanism behind the characteristic hemorrhage.
5. GROSS PATHOLOGY
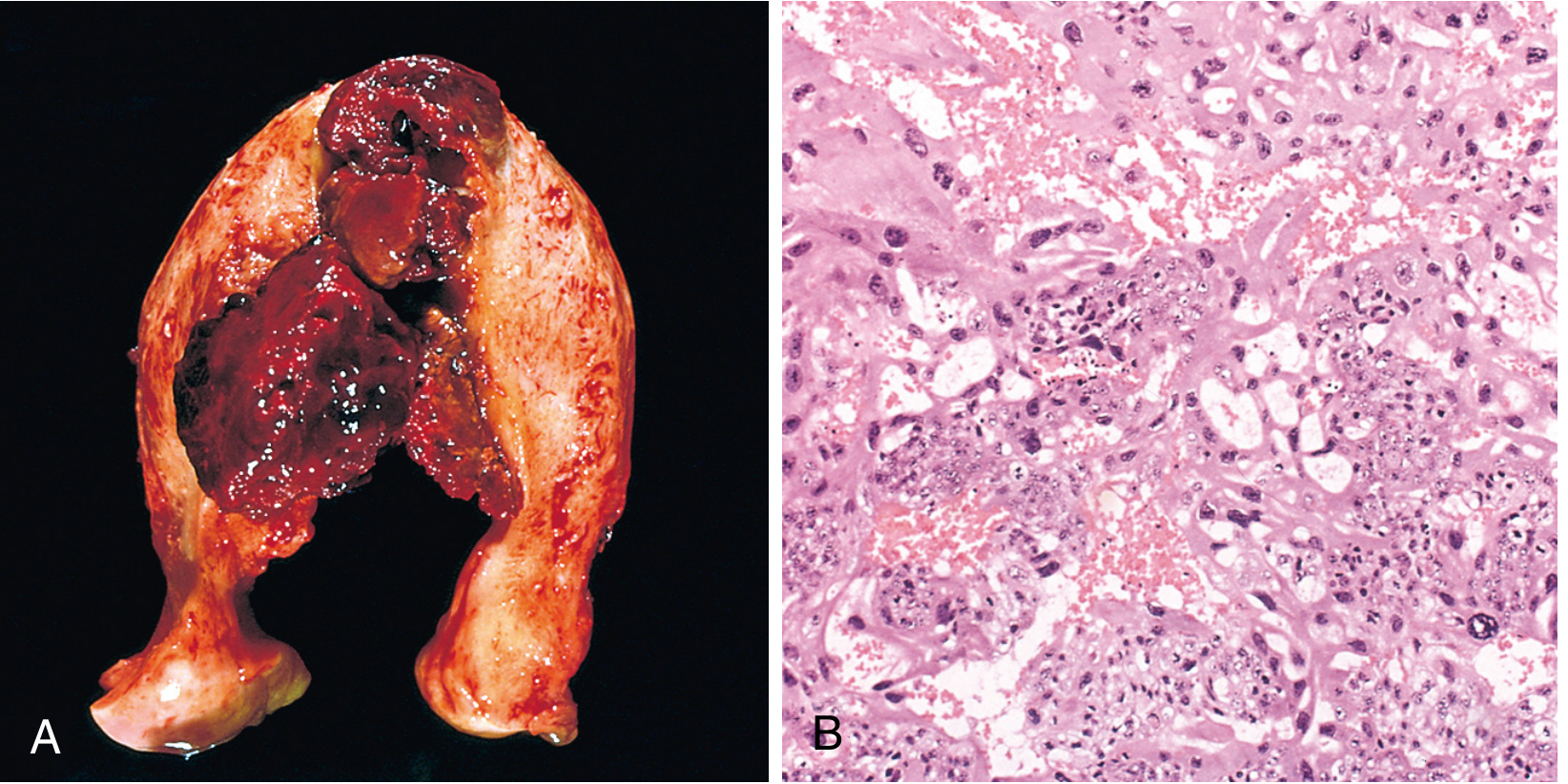
Fig. 22.56 from Robbins, Cotran & Kumar - (A) Bulky hemorrhagic mass invading uterine wall. (B) Malignant cytotrophoblast and syncytiotrophoblast.
Key gross features:
- Soft, fleshy, yellow-white tumor
- Extensive hemorrhage (dark red-brown areas)
- Large pale areas of necrosis
- Typically unilateral
- Can be large; the primary tumor may paradoxically be small even with widespread metastases (especially in testicular counterpart)
6. HISTOPATHOLOGY - THE DIAGNOSTIC CORE
The Golden Rule: Dimorphic Trophoblastic Pattern + No Villi
Fig. 17.22 from Robbins & Kumar Basic Pathology - Choriocarcinoma with cytotrophoblast and syncytiotrophoblast (arrows)
Cell Type 1: Cytotrophoblasts (CT)
- Small to medium polygonal cells
- Mononuclear - single large vesicular nucleus
- Prominent nucleoli
- Clear to pale eosinophilic cytoplasm with distinct cell borders
- Abundant mitoses (these are the proliferating cells)
- Arranged in cohesive nests and sheets - form the "inner" core
- Represent the stem/progenitor trophoblast - analogous to Langhans layer of placenta
Cell Type 2: Syncytiotrophoblasts (ST)
- Large to giant cells
- Multinucleated - 3 to 30+ nuclei in shared cytoplasm
- Nuclei are hyperchromatic, pleomorphic, irregular, crowded and overlapping
- Voluminous, deeply eosinophilic to amphophilic cytoplasm
- Irregular smudged outer borders - reflects cytoplasmic fusion
- Do NOT divide - no mitoses in ST themselves
- Cap and wrap around the CT nests - "peripheral" or "capping" arrangement
- Secrete β-hCG - the source of the hormonal manifestations
The Relationship Between CT and ST
Cytotrophoblasts (proliferate) → fuse → Syncytiotrophoblasts (functional, secrete hCG)
↑ mitotically active ↑ post-mitotic, non-dividing
↑ inner layer ↑ outer/capping layer
Other Key Histological Features
| Feature | Significance |
|---|---|
| Absent chorionic villi | Distinguishes from mole; ESSENTIAL for diagnosis |
| Extensive hemorrhage | Vascular invasion without stroma |
| Coagulative necrosis | Rapidly outgrows blood supply |
| No intrinsic fibrovascular stroma | Tumor relies on eroded host vessels |
| Abundant atypical mitoses | In CT compartment; reflects high proliferative activity |
| Invasive growth | Penetrates capsule, vessels |
7. IMMUNOHISTOCHEMISTRY
| Marker | Staining Pattern | Notes |
|---|---|---|
| β-hCG | Syncytiotrophoblasts strongly + | Diagnostic; correlates with serum levels |
| CK (AE1/AE3) | Both CT and ST + | Confirms epithelial/trophoblastic lineage |
| EMA | Positive | |
| PLAP | May be positive | |
| Inhibin | Negative | Rules out sex cord-stromal tumors |
| AFP | Negative | Helps exclude yolk sac tumor component |
| OCT3/4 | Negative | Unlike dysgerminoma |
| hPL (human placental lactogen) | Weak/focal | More prominent in intermediate trophoblast tumors |
8. CLINICAL FEATURES
Symptoms
- Abdominal pain / pelvic mass - most common presentation
- Irregular uterine bleeding - if uterus is present
- Isosexual precocious puberty - in ~50% of pre-menarchal girls with high hCG (hCG cross-reacts with LH receptor → stimulates estrogen production → early breast development, vaginal bleeding, pubic hair)
- Amenorrhea in reproductive age
- Hemoptysis if pulmonary metastases
Tumor Markers
- β-hCG: markedly elevated - the most important marker for diagnosis, staging, and monitoring
- AFP: negative (if elevated → think yolk sac tumor component → likely mixed GCT)
9. METASTATIC PATTERN
Choriocarcinoma has a propensity for early, widespread hematogenous spread because it invades blood vessels directly:
| Site | Frequency |
|---|---|
| Lungs | 50% - most common; "cannonball" metastases on CXR |
| Vagina | 30-40% |
| Brain | Less common but devastating |
| Liver | Less common |
| Bone, Kidney | Rare |
Lymphatic spread is uncommon - this tumor travels through blood.
10. DIFFERENTIAL DIAGNOSIS
| Tumor | How to Distinguish |
|---|---|
| Gestational choriocarcinoma metastatic to ovary | Clinical history; molecular genotyping (paternal DNA); much better prognosis |
| Embryonal carcinoma | Lacks syncytiotrophoblasts; CD30+, OCT3/4+; may have hCG (focal) |
| Yolk sac tumor | AFP+; Schiller-Duval bodies; reticular/microcystic pattern |
| Dysgerminoma | Large cells with lymphocytic stroma; PLAP+, OCT3/4+; no trophoblast dimorphism |
| Clear cell carcinoma | Hobnail cells; older patients; no hCG |
| Mixed GCT | Contains other components (teratoma, dysgerminoma) alongside choriocarcinoma |
| PSTT (Placental Site Trophoblastic Tumor) | Mononuclear intermediate trophoblasts; hPL+; low hCG; no dimorphism |
11. STAGING (FIGO)
Same staging system as other ovarian malignancies (FIGO 2014):
- Stage I: Confined to ovary/ovaries
- Stage II: Pelvic extension
- Stage III: Peritoneal/retroperitoneal nodes
- Stage IV: Distant metastases (pleural, hepatic parenchyma, brain)
Most patients present at Stage III or IV due to early vascular dissemination.
12. TREATMENT
Surgery
- Unilateral salpingo-oophorectomy with frozen section - fertility-preserving if possible (important given young age of most patients)
- Staging laparotomy; debulk gross metastases
- Hysterectomy + contralateral oophorectomy generally NOT needed unless disease demands it
Chemotherapy
For non-gestational ovarian choriocarcinoma:
- BEP (Bleomycin + Etoposide + Cisplatin) - first-line for ovarian germ cell tumors; 3-4 cycles
- MAC (Methotrexate + Actinomycin D + Cyclophosphamide) - used in gestational form; some reports of complete response in non-gestational too
For gestational choriocarcinoma (if origin is gestational):
- EMA-CO (Etoposide, Methotrexate, Actinomycin D, Cyclophosphamide, Oncovin/Vincristine) - near 100% cure
- Single-agent methotrexate or actinomycin D for low-risk disease
Key difference: Gestational type responds dramatically to chemotherapy (near 100% remission). Non-gestational ovarian type is relatively chemoresistant and has a poor prognosis.
(Berek & Novak's Gynecology; Robbins, Cotran & Kumar)
13. PROGNOSIS
| Type | Prognosis |
|---|---|
| Non-gestational ovarian choriocarcinoma | Poor - most have metastases at diagnosis; relatively chemoresistant |
| Gestational choriocarcinoma (even with metastases) | Excellent - near 100% cure with chemotherapy |
| Mixed GCT containing choriocarcinoma (< 1/3 of tumor) | Good prognosis |
| Mixed GCT where choriocarcinoma is dominant component | Poor |
Important: For mixed GCTs, the most malignant component and its relative proportion determine prognosis. Stage IA tumors < 10 cm have 100% survival.
14. WORKUP SUMMARY (What to Order)
Suspected Ovarian Choriocarcinoma
│
├── SERUM: β-hCG (diagnostic + monitor), AFP, LDH, CA-125
├── IMAGING: CT chest/abdomen/pelvis (staging), MRI pelvis, CXR
├── HISTOLOGY: Frozen section → paraffin H&E
├── IHC: β-hCG, CK, AFP, inhibin, OCT3/4, CD30
├── MOLECULAR: STR genotyping to distinguish gestational vs non-gestational
└── ONCOLOGY REFERRAL: Urgent (aggressive tumor)
15. QUICK MEMORY AIDS
"Choriocarcinoma = 2 cells + No Villi + Hemorrhage"
CT = "Cuboidal, Cycling, Clear" (mononuclear, proliferating, pale cytoplasm)
ST = "Syncytia, Secretes hCG, Smudged" (multinucleated, non-dividing, hCG maker)
Gestational vs Non-gestational = "Paternal DNA = Curable"
Metastases = "Lung first, then Vagina, then Brain"
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (10th ed.); Robbins & Kumar Basic Pathology; Berek & Novak's Gynecology (16th ed.)
Teach me fibrosadenoma with lactational change in vulva
Finding Sources
Finding Sources
Searching PubMed
"fibroadenoma" AND "vulva" AND "lactational change"
Finding Sources
Finding Sources
Searching PubMed
"ectopic breast" AND "vulva" AND "fibroadenoma"
Reading File
Reading Article
PMID: 21169735
Reading Article
PMID: 41040519
Reading File
Reading Article
PMID: 32983911
Finding Sources
Finding Sources
Finding Sources
Searching the Web
fibroadenoma with lactational change vulva anogenital mammary-like glands histopathology
Reading Web Page
https://basicmedicalkey.com/lesions-of-anogenital-mammary-li…
Loading Image
I now have all the material needed. Here is the comprehensive teaching note:
🎓 Fibroadenoma with Lactational Change in the Vulva - Complete Teaching Note
1. UNDERSTANDING THE FOUNDATION: What Is the Tissue of Origin?
This is the most important concept to grasp first. To understand fibroadenoma of the vulva, you must understand Anogenital Mammary-Like Glands (AGMLG).
What are AGMLGs?
These are specialized glands normally present in the vulvar/perianal skin that are structurally and functionally identical to breast glandular tissue. They were previously thought to be ectopic breast tissue, but the current view (since Kazakov et al., 2011) is that they represent a normal constituent of the anogenital area - not an anomaly.
They share:
- The same morphology as breast lobular units (ductal + acinar structures)
- Identical immunohistochemical profile (ER+, PR+, GCDFP-15+, GATA3+, p63+ myoepithelium)
- The same hormonal responsiveness (enlarge during pregnancy, involute after menopause)
- The same capacity to develop all the same lesions as the breast
The landmark Kazakov et al. review established that these glands should be approached "through the eyes of a breast pathologist."
The Embryological Basis: The Milk Line
Axilla
↓
Breast (normal)
↓
Inframammary region
↓
Abdomen
↓
Groin
↓
VULVA ← ← ← ← (AGMLG territory)
↓
Perineum
During embryogenesis, the milk ridge (mammary line) extends bilaterally from axilla to groin. Normally only the pectoral segment persists to form the breast. Remnants along this line can persist as ectopic breast tissue OR the anogenital region normally retains mammary-like glands.
Key point: Because vulvar tissue contains breast-like glandular elements, it can develop any lesion that the breast develops - fibroadenoma, phyllodes tumor, lactating adenoma, sclerosing adenosis, DCIS, invasive carcinoma, and Paget disease.
2. FIBROADENOMA OF THE VULVA - DEFINITION
Fibroadenoma of the vulva (also called ectopic breast fibroadenoma of the vulva) is a benign biphasic fibroepithelial tumor of the vulva arising from either:
- AGMLG tissue (most current explanation), OR
- Ectopic breast tissue along the milk line that persisted in the vulva
It is histologically identical to fibroadenoma of the breast. As the UPMC Case 863 discussion states: "a breast-like benign biphasic fibroepithelial neoplasm composed of an epithelial glandular component and a stromal component... common neoplasm in an uncommon site."
3. EPIDEMIOLOGY & CLINICAL FEATURES
| Feature | Detail |
|---|---|
| Incidence | Extremely rare - ~50 benign ectopic breast lesions reported in world literature |
| Age | Predominantly reproductive age (20s-40s); rare case reports in postmenopausal women |
| Site | Labia majora most common; labia minora less common |
| Presentation | Slowly enlarging, painless, firm, mobile nodule - identical to breast fibroadenoma |
| Hormonal responsiveness | Yes - may enlarge rapidly during pregnancy/lactation |
| Bilaterality | Rare but reported; may coexist with axillary ectopic breast fibroadenoma |
| Key paper | He et al., 2025 (PMID 41040519) - 41-year-old with incidental painless right vulvar mass confirmed as ectopic breast fibroadenoma |
Misdiagnosis risk: Clinically it can be mistaken for a Bartholin gland cyst, lipoma, epidermal cyst, or soft tissue tumor. Pre-operative imaging (ultrasound) shows a well-circumscribed hypoechoic nodule - same as breast fibroadenoma.
4. GROSS PATHOLOGY
Identical to breast fibroadenoma:
- Well-circumscribed, rubbery, gray-white nodule
- Bulges above cut surface when sectioned
- Slit-like spaces visible on cut surface (represents compressed glandular elements)
- No hemorrhage, necrosis, or infiltrative borders
(Robbins, Cotran & Kumar - Pathologic Basis of Disease)
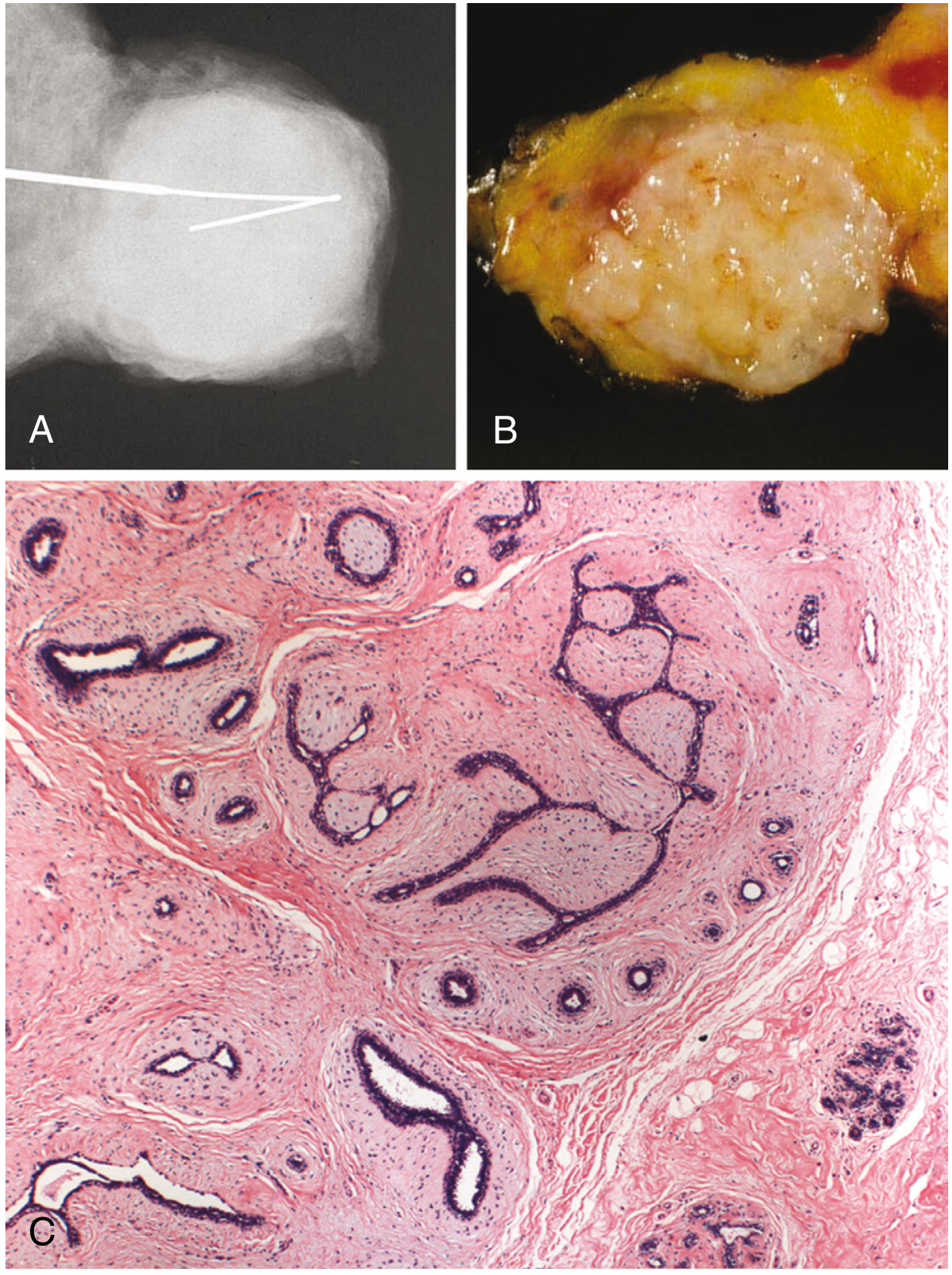
Fig. 23.24 from Robbins, Cotran & Kumar - Fibroadenoma: (A) well-circumscribed mass on imaging, (B) gray-white rubbery gross appearance, (C) histology showing fibrous stroma surrounding and distorting glandular elements - identical features apply to vulvar fibroadenoma
5. HISTOPATHOLOGY - STANDARD FIBROADENOMA
Basic Biphasic Architecture
FIBROADENOMA = EPITHELIAL component + STROMAL component
Epithelial Component:
- Branching glandular/ductal structures
- Inner epithelial layer + outer myoepithelial layer (bilayered)
- Luminal cells are cuboidal to columnar, uniform, no atypia
- Nuclei: small, round, regular with inconspicuous nucleoli
Stromal Component:
- Delicate, myxoid to fibrous stroma resembling normal intralobular stroma
- Hypocellular (paucicellular) - this is a key distinguishing feature from phyllodes tumor
- No stromal atypia, no significant mitoses
Two Growth Patterns
| Pattern | Description | Appearance |
|---|---|---|
| Pericanalicular | Stroma surrounds patent, round ducts | Ducts remain open/oval |
| Intracanalicular | Stroma compresses ducts into slit-like/irregular clefts | Distorted branching "antler" shapes |
Both patterns can coexist in the same tumor.
6. LACTATIONAL CHANGE - THE SPECIAL FEATURE
What Is Lactational Change?
When a fibroadenoma of the vulva (or breast) undergoes lactational change, the epithelial cells of the glandular component transform under the influence of prolactin and progesterone during pregnancy or lactation to show active secretory activity.
Histological Features of Lactational Change:
| Feature | Description |
|---|---|
| Cytoplasmic vacuoles | Cells contain large, bubbly, pale cytoplasmic lipid/secretory vacuoles - the hallmark |
| Hobnail appearance | Nuclei pushed to base by vacuoles; apical cytoplasm protrudes into lumen (apocrine-like snouts) |
| Intraluminal secretion | Eosinophilic proteinaceous or milky secretion within gland lumens |
| Acinar dilation | Round, dilated acini/tubules, closely packed |
| Stroma | Fibrous stroma persists but may appear less prominent against expanded glands |
| Mitoses | May be present - do not interpret as malignancy in this context |
| Architecture | Well-circumscribed; the fibroadenoma architecture (biphasic) is maintained |
Schematic of Lactational Change:
Normal epithelial cell:
[Nucleus in center] [Pale cytoplasm]
With Lactational Change:
[Nucleus pushed to base ↓] [Vacuolated cytoplasm with fat globules ↑↑↑]
[Secretion into lumen →]
Why Does This Happen in the Vulva?
Because AGMLGs are hormonally responsive - they express estrogen receptors (ER) and progesterone receptors (PR), just like breast tissue. During pregnancy, rising prolactin and progesterone stimulate secretory differentiation. The fibroadenoma's glandular epithelium responds in exactly the same way as breast lobular epithelium.
This is why vulvar fibroadenomas may:
- Enlarge rapidly during pregnancy - raising clinical suspicion of malignancy
- Become tender or fluctuant during lactation
- Spontaneously regress after delivery/cessation of breastfeeding
7. LACTATIONAL CHANGE vs. LACTATING ADENOMA - KEY DISTINCTION
These two entities overlap and are often confused:
| Feature | Fibroadenoma with Lactational Change | Lactating Adenoma (vulvar) |
|---|---|---|
| Background | Pre-existing fibroadenoma + lactational change in epithelium | De novo lactational lesion; no pre-existing FA |
| Architecture | Biphasic - both glandular AND fibrous stroma components | Purely epithelial - densely packed tubules, minimal stroma |
| Stroma | Fibrous stroma present (key!) | Stroma minimal/absent |
| Gland pattern | Distorted/compressed (intracanalicular) + secretory cells | Round, closely packed, acini-only |
| Vacuoles | Present in epithelium | Present and dominant |
| Timing | Usually post-pregnancy enlargement of known nodule | De novo mass during pregnancy |
| Key reference | Kazakov et al., 2010 (Am J Surg Pathol) | Same authors |
Practical pearl: "Other lesions of anogenital mammary-like glands can exhibit lactational changes such as a fibroadenoma." - Basicmedical Key (citing Kazakov)
A fibroadenoma with lactational change retains the biphasic architecture - you can still identify the fibrous stroma compressing glandular elements. If stroma is absent and it is purely secretory acini, think lactating adenoma.
8. IMMUNOHISTOCHEMISTRY
| Marker | Result | Significance |
|---|---|---|
| ER (Estrogen Receptor) | Positive (epithelial component) | Confirms breast-like lineage; explains hormonal behavior |
| PR (Progesterone Receptor) | Positive | Same |
| GATA3 | Positive | Mammary lineage marker |
| p63 | Positive (myoepithelial layer) | Confirms bilayered architecture (rules out carcinoma which lacks myoepithelium) |
| CK5/6, SMA | Myoepithelial layer positive | |
| GCDFP-15 | May be positive | Gross cystic disease fluid protein; apocrine/mammary marker |
| Ki-67 | Low | Confirms benign behavior |
| MED12 mutation | Present in ~2/3 | Same driver mutation as breast fibroadenoma |
The bilayered ductal architecture (epithelium + myoepithelium) confirmed by p63/SMA is the single most important feature distinguishing fibroadenoma from carcinoma.
9. DIFFERENTIAL DIAGNOSIS
| Lesion | How to Distinguish |
|---|---|
| Lactating adenoma | No fibrous stroma; purely packed acini; no biphasic pattern |
| Phyllodes tumor | Leaf-like projections; cellular stroma with mitoses; stroma overgrows epithelium |
| Hidradenoma papilliferum | Papillary-glandular architecture; anastomosing tubules; no fibrous stroma |
| Bartholin gland cyst | Cystic; lined by transitional/squamous epithelium; no glandular elements |
| Epidermal inclusion cyst | Keratinous contents; squamous lining |
| Pseudoangiomatous stromal hyperplasia (PASH) | Slit-like empty spaces in stroma mimicking vascular channels; no glandular component |
| Sclerosing adenosis | More compressed, distorted acini with myoepithelial proliferation |
| Invasive carcinoma from AGMLG | Infiltrative borders; loss of myoepithelium (p63 negative); cytologic atypia |
| Extramammary Paget disease | Intraepidermal Paget cells; CK7+, GCDFP-15+; no mass |
10. TREATMENT & PROGNOSIS
- Simple (complete) surgical excision - curative; en-bloc excision is preferred
- Recurrence: rare with complete excision; incomplete excision or hormone exposure (pregnancy) can drive recurrence
- Long-term surveillance: warranted because:
- Hormonal re-stimulation (future pregnancies) can cause recurrence
- Small risk of malignant transformation (same as breast fibroadenoma - slightly elevated if complex)
- Prognosis: Excellent - benign behavior identical to breast fibroadenoma
- Fertility preservation: surgery is straightforward; no impact on fertility or breastfeeding from the contralateral breast
11. FULL SPECTRUM OF AGMLG LESIONS (Context)
Because AGMLGs behave like breast tissue, the full spectrum of breast pathology can occur here:
BENIGN BORDERLINE MALIGNANT
├── Fibroadenoma ├── Phyllodes tumor ├── Invasive carcinoma
├── Lactating adenoma │ (borderline) ├── DCIS
├── Hidradenoma papilliferum ├── Phyllodes (malignant)
├── Sclerosing adenosis ├── Hidradenocarcinoma papilliferum
├── Fibrocystic change └── Extramammary Paget disease
├── PASH
└── Intraductal papilloma
12. QUICK MEMORY FRAMEWORK
FIBROADENOMA VULVA = "Breast tumor in wrong address"
Origin: Anogenital Mammary-Like Glands (AGMLG) - normally present in vulva
Histology: BIPHASIC = glands (ER+, bilayered) + fibrous stroma
Lactational change = glands + cytoplasmic vacuoles + secretion + maintained stroma
IHC: ER+, PR+, GATA3+, p63+ myoepithelium
Clinically: Painless mobile nodule in labia majora, reproductive age woman
Pregnancy: Rapid enlargement (do NOT panic - benign)
Treatment: Excise completely; follow up
Distinguish from phyllodes: stroma cellularity + mitoses
Distinguish from lactating adenoma: biphasic vs. purely secretory
Sources: Robbins, Cotran & Kumar - Pathologic Basis of Disease (10th ed.); Kazakov DV et al., Adv Anat Pathol 2011, PMID 21169735; He Y et al., Front Oncol 2025, PMID 41040519; Hernandez Lopez AL et al., Case Rep Womens Health 2020, PMID 32983911; UPMC Pathology Case 863
This is a shared conversation. Sign in to Orris to start your own chat.