history of peritoneal dialysis
Reading File
Searching the Web
history of peritoneal dialysis timeline development
Finding Sources
Reading Web Page
https://ispd.org/media/pdf/Genesis.pdf
I now have a rich set of sources. Let me compile the full history:
History of Peritoneal Dialysis
Precursors (1740s)
The idea of using the peritoneal cavity for fluid therapy predates modern medicine. In the early 1740s, Christopher Warrick in England treated a 50-year-old woman with severe ascites by instilling fluid into the peritoneal cavity and draining it - an early form of paracentesis. In 1743, Reverend Stephen Hales published modifications to the technique. Though these were not dialysis procedures in the modern sense, they demonstrated that the peritoneum could tolerate fluid manipulation.
Early Experimental Era (1920s)
1923 - Georg Ganter, a German physician, is credited with performing the first true peritoneal dialysis. He instilled hypertonic saline into the peritoneal cavity of a guinea pig and then attempted the procedure in humans suffering from uremia - without clinical success. His work established the theoretical basis for PD.
1926 - Physiologist R. Cunningham published a landmark review on the physiology of serous membranes, clarifying that the peritoneum acts as a semi-permeable membrane capable of selective solute transfer - the scientific underpinning of PD.
1927 - Heinrich Heusser and Hermann Werder treated 3 patients with continuous flow PD using two catheters simultaneously (one for inflow, one for outflow). They demonstrated measurable decreases in blood urea nitrogen - the first evidence of clinical efficacy - but could not achieve sustained clinical improvement.
1938 - Jonathan Rhoads introduced lactate to the PD solution to buffer metabolic acidosis, correcting one of the major biochemical problems with early dialysate. Lactate buffering remains in use today.
First Clinical Success (1940s)
1945-1946 - Howard Frank, Arnold Seligman, and Jacob Fine at Beth Israel Hospital, Boston, achieved the first undisputed clinical success. They treated a 51-year-old man with acute renal failure caused by sulfathiazole (sulfa drug) poisoning. Their system used sterilized large bottles of solution and two catheters to prevent outflow obstruction. The patient fully recovered - a defining moment in PD history.
Their innovation also addressed several technical problems: optimal flow rates, solution modification for patient needs, and sterility through pre-sterilized bottles.
Intermittent PD and Technical Refinements (1950s-1960s)
1952 - Arthur Grollman at Southwestern Medical School, Dallas, published a comprehensive book on PD. He described a 1-liter container connected via plastic tubing to a flexible polyethylene catheter with small holes at the distal end to prevent tissue obstruction - dramatically improving inflow and outflow. This design became the forerunner of modern intermittent PD (IPD) systems.
1959 - Paul Doolan and Richard Ruben at Naval Hospital Oakland performed the first PD for end-stage renal disease (ESRD) - not just acute kidney failure. Their patient, Willie Mae Stewart, a 33-year-old woman, underwent 6 months of intermittent PD. Though she eventually declined further treatment and died in June 1960, this was the first demonstration that PD could sustain a chronic kidney failure patient.
1962 - Fred Boen and colleagues at the University of Washington reported using periodic peritoneal dialysis for managing chronic uremia, publishing the kinetics of PD - the first quantitative framework for dosing.
1964-1965 - Henry Tenckhoff, G. Shilipetar, and Fred Boen at the University of Washington reported the first successful home peritoneal dialysis program with long-term results, despite the technical burdens at the time.
1968 - Henry Tenckhoff created the Tenckhoff catheter - a silicone rubber catheter with two Dacron cuffs that anchored the catheter subcutaneously and reduced infection. Before this, a new catheter had to be placed into the abdomen before every single treatment session. The Tenckhoff catheter allowed permanent, chronic access and remains the standard PD catheter in use today.
Automation and the Cycler (1960s-1970s)
1964 - Boen developed a machine for automated cycling of PD fluid, reducing the manual labor burden of IPD.
1966-1970 - Norman Lasker combined the work of Boen, Tenckhoff, and Russell Palmer to create the "Lasker cycler" - an automated PD machine. By 1970, the first patients were receiving home dialysis with a cycler.
1969-1974 - Dimitrios Oreopoulos at Toronto Western Hospital built the largest IPD program in the world. After visiting Philadelphia to observe the Lasker cycler, he adopted it for home patients. By 1974 he was managing over 70 home PD patients - an unprecedented scale at the time.
CAPD: The Landmark Innovation (1976-1978)
1976 - Robert Popovich and Jack Moncrief at the University of Texas developed the concept of Continuous Ambulatory Peritoneal Dialysis (CAPD). The key insight was that keeping dialysate continuously in the peritoneal cavity - with manual bag exchanges 4 times daily - could achieve adequate solute clearance without a machine, 24 hours a day, 7 days a week.
1978 - Popovich, Moncrief, and Karl Nolph published the first clinical CAPD results, demonstrating that patients could manage their own dialysis at home without a cycler. The simplicity and freedom of CAPD transformed the field: patients could work, travel, and live more normally.
The 1972 US Medicare legislation funding dialysis for all ESRD patients had created the financial environment that made large-scale CAPD programs possible.
Automated PD and Modern Era (1980s-present)
1981 - José Diaz-Buxo proposed Continuous Cyclic Peritoneal Dialysis (CCPD) - overnight automated cycling with a daytime dwell. This is now the most widely used form of Automated PD (APD), using 10-15 liters of dialysate overnight.
1980s-1990s - Biocompatible PD solutions were developed. Standard glucose-lactate solutions caused long-term peritoneal membrane damage. New formulations using:
- Icodextrin (a glucose polymer) for long dwells
- Amino acid-based solutions
- Bicarbonate/bicarbonate-lactate buffers (lower glucose degradation products) ...were introduced to better preserve the peritoneal membrane.
Late 1980s-1990s - The International Society for Peritoneal Dialysis (ISPD) was established, creating global guidelines, a registry, and standardized training protocols.
2000s-present - Continuous advances include:
- Better connectology (Y-set and twin-bag systems) to reduce peritonitis rates
- Peritoneal equilibration testing (PET) to characterize membrane transport type and tailor prescriptions
- Assisted PD programs enabling elderly and disabled patients to receive PD with nurse or caregiver help at home
- Improved outcomes data from registries (USRDS, ANZDATA, PDOPPS) guiding prescriptions
Key Figures at a Glance
| Person | Contribution | Year |
|---|---|---|
| Georg Ganter | First PD experiment | 1923 |
| Howard Frank / Seligman / Fine | First clinical success | 1945-46 |
| Arthur Grollman | Flexible catheter design, published IPD system | 1952 |
| Henry Tenckhoff | Tenckhoff catheter (permanent PD access) | 1968 |
| Norman Lasker | Automated cycler for home IPD | 1970 |
| Dimitrios Oreopoulos | Large-scale home IPD programs | 1974 |
| Robert Popovich / Jack Moncrief | Invention of CAPD | 1976 |
| José Diaz-Buxo | CCPD / Automated PD | 1981 |
The Wikipedia PD history timeline and the ISPD's Genesis document are excellent primary references. The clinical detail above also draws on Brenner and Rector's The Kidney and Fischer's Mastery of Surgery from the medical library.
pd apparatus solutions transfer set connectologies access for pd catheter and exit site care in detail
Reading File
Finding Sources
Finding Sources
Searching the Web
peritoneal dialysis apparatus solutions transfer set connectology exit site care ISPD guidelines
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is the full, detailed synthesis:
PD Apparatus, Solutions, Transfer Sets, Connectology, Access (Catheter), and Exit Site Care
1. PD APPARATUS
1.1 Manual Exchange System (CAPD)
In continuous ambulatory peritoneal dialysis (CAPD), the patient performs exchanges manually, 4-5 times per day. The equipment consists of:
- PD bag (typically 2 L) containing dialysate, connected via tubing
- A transfer set/extension tubing that connects the bag to the catheter
- A clamp and titanium or plastic connector
- No electricity or machine is required
Each exchange involves: drain (gravity empties old dialysate) → fill (new dialysate infuses by gravity) → dwell (fluid remains in peritoneum for prescribed time). A standard 2-L bag should run in within 15 minutes under gravity.
1.2 Automated PD Cycler (APD Machine)
The cycler (also called an automated peritoneal dialysis or APD machine) performs exchanges automatically, usually overnight (8-10 hours while the patient sleeps). Core components:
- Pump - drives controlled inflow and outflow of dialysate through cassette or peristaltic pump
- Heating element - warms dialysate bags to body temperature (37°C) before infusion
- Weighing or volumetric system - measures fill and drain volumes accurately per cycle
- Programmable controller - operator or clinician programs: dwell volume, dwell time, number of cycles, last fill (or "dry" day)
- Alarm system - alarms for drain failure, occlusion, low fill, patient disconnect
- Cassette/tubing set - single-use, sterile disposable tubing set that connects dialysate bags to the cycler and to the patient's catheter
- Bags - typically 5-L bags are used for overnight cycling; up to 15 L total dialysate used per session
The Continuous Cyclic PD (CCPD) prescription (the most common APD form) involves 4-6 overnight cycles with a final "last fill" left in the peritoneum during daytime for a continuous long dwell. Modern cyclers (e.g., Baxter HomeChoice, Fresenius Sleep•Safe) are fully programmable with remote data logging and connectivity to the dialysis unit.
Nocturnal Intermittent PD (NIPD): The cycler runs at night but the patient drains dry at the end of the session (no daytime dwell). Suitable only for patients with significant residual kidney function.
2. PD SOLUTIONS (DIALYSATE)
PD solutions are instilled into the peritoneal cavity and act as the dialysate. Their composition determines osmolality, buffering, and biocompatibility.
2.1 Standard Glucose-Based Solutions (Conventional)
These are the most widely used dialysate solutions:
| Component | Details |
|---|---|
| Osmotic agent | Dextrose (glucose) at 1.5%, 2.5%, or 4.25% |
| Buffer | Lactate (35-40 mEq/L) |
| Electrolytes | Na⁺ 132 mEq/L, Ca²⁺ 2.5 mEq/L (or 3.5 mEq/L), Mg²⁺ 0.5-1.5 mEq/L, Cl⁻ 96-102 mEq/L |
| pH | Acidic (~5.5) - due to sterilization processes |
| GDPs | High levels of glucose degradation products (GDPs) from heat sterilization |
Color-coding convention used clinically: yellow = 1.5%, green = 2.5%, red = 4.25%
The glucose concentration drives ultrafiltration: higher glucose = greater osmotic gradient = more water removed. However, higher glucose is associated with:
- Increased inward glucose absorption → worsening hyperglycemia in diabetics
- GDP accumulation → peritoneal membrane damage with long-term use
- Dyslipidemia, insulin resistance, obesity
2.2 Icodextrin Solution
- Osmotic agent: Icodextrin - a glucose polymer (starch-derived, high molecular weight polysaccharide)
- Buffer: Lactate
- pH: Physiologic (5.8-6.4)
- Concentration: 7.5%
Because icodextrin is a large polymer, it is minimally absorbed from the peritoneum, maintaining an effective osmotic gradient for up to 18 hours - making it ideal for the long dwell in CAPD (overnight) or the daytime dwell in APD.
Key advantages:
- Superior ultrafiltration in high/high-average transporters compared to 2.5-4.25% glucose during long dwells
- Regression of left ventricular hypertrophy (through better volume control)
- Better glycemic control and insulin sensitivity
- Reduced total body water
Important adverse effects and cautions:
- Skin rash (exfoliating, palms/soles) - occurs 2-3 weeks after starting, resolves on stopping
- False high glucose readings - glucometers using glucose dehydrogenase pyrroloquinoline quinone (GDH-PQQ) will overestimate blood glucose due to accumulated maltose (icodextrin metabolite); extreme caution is required to prevent inadvertent insulin administration
- Aseptic peritonitis - rare, linked historically to peptidoglycan contamination from manufacturing; largely eliminated with process improvements
(Brenner and Rector's The Kidney; Comprehensive Clinical Nephrology, 7th Ed.)
2.3 Low-GDP (Biocompatible) Glucose Solutions
A dual-chamber bag design keeps the glucose and the buffer in separate compartments until just before use (to prevent GDP formation during sterilization):
- Buffer: Lactate, but mixed just before infusion to minimize GDPs
- pH: Physiologic (~7.0-7.4)
- GDPs: Undetectable or very low
Potential benefits: Better preservation of peritoneal membrane long-term; preservation of residual kidney function; possibly lower peritonitis rates. However, prospective clinical trial data showing a meaningful benefit (e.g., lower modality failure or mortality) remains inconsistent. Use is driven by availability and cost.
2.4 Bicarbonate-Based Solutions
Another dual-chamber design:
- Buffer: Bicarbonate (physiologic buffer) ± small amount of lactate
- pH: Neutral (~7.2-7.4)
- More complete correction of metabolic acidosis
- Reduced infusion pain (a common complaint with acidic conventional solutions)
- No conclusive evidence for better peritoneal membrane preservation
2.5 Amino Acid Solution
- Osmotic agent: 1.1% amino acids (provides ultrafiltration equivalent to 1.5% glucose)
- Buffer: Lactate
- Used as a single exchange in malnourished PD patients for nutritional supplementation
- Part of "glucose-sparing" regimens (reducing total daily glucose load)
- Risk: may worsen pre-existing azotemia or acidosis if used too frequently
2.6 Glucose-Sparing Regimens
To reduce cumulative glucose exposure, a structured prescription may combine:
- 3 exchanges of 1.5% glucose (CAPD)
- Replace overnight (long dwell) with icodextrin
- Replace one daytime exchange with amino acid solution
This reduces hyperglycemia, improves lipid profile, but carries a risk of volume overload (reduced ultrafiltration) and is typically reserved for selected patients, given higher cost.
3. TRANSFER SETS AND CONNECTOLOGY
The transfer set (also called an extension set or line set) is the piece of tubing that permanently connects the external end of the PD catheter to the dialysate exchange bags. It is a critical link in the PD circuit and is the main site of potential bacterial contamination.
3.1 Components of the Transfer Set
- A length of PD-grade silicone or polyurethane tubing (typically 30-40 cm long)
- A clamp on the tubing to prevent dialysate flow when not exchanging
- A connector end that attaches to the catheter's titanium adapter
- A disconnect cap or bag spike at the other end
The transfer set is changed every 6 months (or sooner if contamination occurs) by trained PD nurses.
3.2 Historical Evolution of Connectology
Early CAPD (late 1970s-early 1980s) used a spike system where each exchange required directly spiking a new bag. This "straight-line" connection had a high peritonitis rate (~1 episode per 9-12 patient-months) because the open connection was a major contamination risk.
Y-set system (introduced 1980s):
The most important advance in PD connectology. A Y-shaped tubing connects one arm to a fresh dialysate bag, one arm to a drain bag, and the common limb to the catheter. The sequence is:
- Connect the Y-set to the catheter
- Drain first (drain old dialysate into the drain bag)
- Flush a small volume of new dialysate through the drain line (the "flush-before-fill" step - flushes any introduced bacteria to the drain, not into the patient)
- Fill fresh dialysate from the new bag into the peritoneum
- Disconnect the Y-set and cap the catheter
The flush-before-fill step (the "Y-set" principle) is the single most impactful advance in preventing touch-contamination peritonitis. It reduced peritonitis rates from 1 episode per 9 months to approximately 1 episode per 24 months - as cited by Harrison's Principles of Internal Medicine (22nd Ed.).
3.3 Twin-Bag / Double-Bag System
A refinement of the Y-set: both the fresh dialysate bag and the drain bag come pre-attached as a single unit to the Y connector. This system:
- Eliminates the need to attach separate bags
- Reduces connections and disconnections (fewer touch events)
- Is now the standard for CAPD
- Combines flush-before-fill + disconnect system in a single device
3.4 Disconnect Systems
After filling, the patient disconnects the transfer set from the bag/tubing system and caps it with a sterile cap. This means the catheter and transfer set are not attached to anything between exchanges. This "disconnect" design reduces the burden of carrying a bag and further reduces peritonitis risk.
3.5 APD Connectology
In APD, the patient connects to the cycler's cassette tubing before bed and disconnects in the morning. The cycler tubing is:
- A single-use sterile cassette (in most modern machines)
- Connected via a spike connection to 2-5 dialysate bags
- Connected to the patient's transfer set via a sterile luer-lock or push-pull connector
Prevention principle: The ISPD recommends "flush-before-fill" of the tubing system as part of the infection prevention strategy, applicable to both CAPD and APD setups (ISPD 2023/2024 Guidelines on Catheter-Related Infections).
4. ACCESS FOR PD: THE PD CATHETER
4.1 Catheter Materials and Basic Design
Modern PD catheters are made of medical-grade silicone rubber (or polyurethane). Silicone is biocompatible, flexible, and durable. The standard catheter has:
- An intraperitoneal segment with multiple side holes and/or end holes for fluid distribution
- One or two Dacron felt cuffs - fibrous polyester cuffs that anchor the catheter in tissue; fibrous ingrowth seals the tract against bacteria
- A subcutaneous tunnel segment between the deep cuff and exit site
- An external segment exiting through the skin
4.2 Catheter Designs
Tenckhoff Catheter (1968 - still the most widely used):
- Straight or coiled intraperitoneal segment (coiled design reduces infusion pain by distributing the jet effect of flow)
- Single cuff or double cuff (double cuff is preferred - deep cuff in rectus muscle, superficial cuff ~2-3 cm from skin)
- Deep cuff prevents intraperitoneal leaks; superficial cuff reduces infection tracking along the tunnel
Swan-Neck Catheter (Twardowski design):
- The external segment has a permanent downward-facing curve ("swan-neck" shape)
- Directs the exit site downward, which promotes drainage of any discharge away from the site
- Reduces cuff extrusion and improves catheter survival compared to straight-exit Tenckhoff
- Recommended by ISPD guidelines as the preferred design
Presternal Catheter:
- The external segment is tunneled subcutaneously to exit at the presternal (chest) location rather than the abdomen
- Particularly beneficial for: obese patients, patients with abdominal stomas, children in diapers, patients with fecal incontinence
- Associated with decreased exit site infection and peritonitis rates
- Access survival of up to 95% at 2 years reported
Toronto Western Catheter:
- Has two silicone discs in the intraperitoneal segment
- The discs act as flanges, anchoring the catheter tip within the pelvis and reducing tip migration
Coiled vs. Straight Intraperitoneal Tip:
- Coiled tip has multiple holes distributed over a larger area
- Reduces localized jet pain during fill
- May be slightly more prone to tip migration
4.3 Catheter Insertion Techniques
Four main approaches exist:
1. Surgical (open dissection / cut-down)
- Under general or regional anesthesia
- Direct visualization of catheter placement
- Most widely used historically but associated with higher rates of infection and outflow failure vs. minimally invasive methods
2. Seldinger Technique (Fluoroscopic / Ultrasound Guided)
- Most used by nephrologists
- Uses the same fluoroscope and disposables as central venous catheter placement
- Ultrasound guides an 18-21 gauge needle into the peritoneum
- Contrast injection produces "spider web" pattern confirming intraperitoneal position
- A guidewire is advanced, dilators track over it, and the catheter is inserted through a peel-away sheath
- Deep cuff placed in rectus muscle; tunnel and exit site created with a tunneling tool
- Requires local anesthesia ± conscious sedation (midazolam + fentanyl)
- Associated with fewer complications than open surgical technique in randomized studies
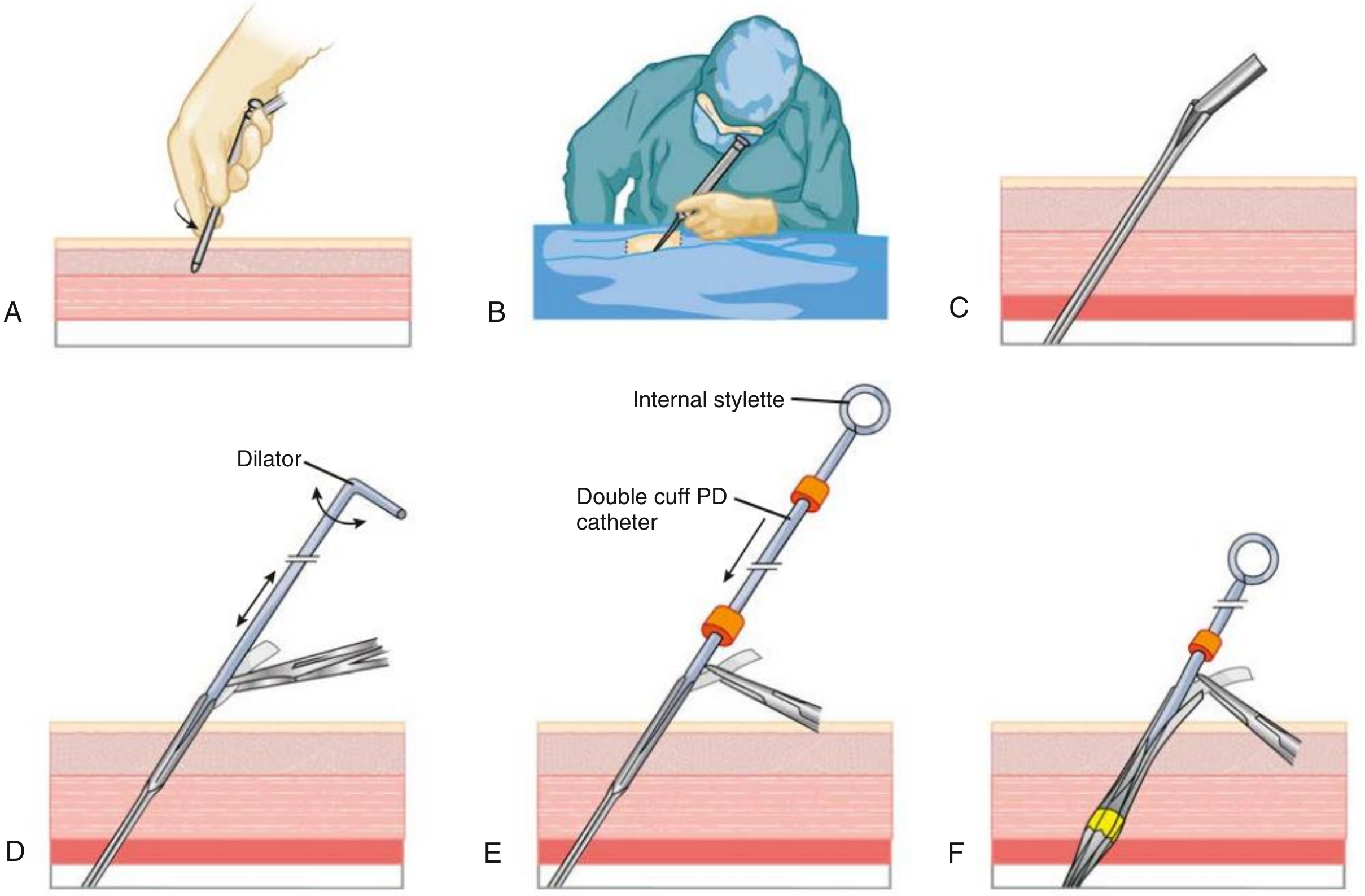
3. Peritoneoscopic Technique (Y-Tec)
- Single puncture using a 2.2-mm diameter optical peritoneoscope
- Air (600-1000 mL) insufflated for visualization
- Allows direct inspection of peritoneal surfaces for adhesions, hernias
- Trocar-cannula with spiral sheath inserted through rectus muscle at 45°; sheath dilated to 6 mm; catheter passed through dilated sheath with internal stylet
- Deep cuff implanted in rectus muscle with implanter tool (no dissection of anterior rectus sheath)
- Advantages: local anesthesia, less tissue dissection, lower rates of infection/outflow failure/pericatheter leak, immediate use possible for intermittent PD
4. Laparoscopic Technique
- General anesthesia; multiple port sites; CO₂ insufflation
- Best for patients with prior abdominal surgery, adhesions, hernias
- Allows advanced techniques: omentopexy (omentum tacked away from catheter), hernia repair, adhesiolysis
- Results in improved long-term catheter success
Comprehensive Clinical Nephrology, 7th Ed., Fig. 97.1
4.4 Optimal Timing of Catheter Insertion
- Catheter placed when GFR falls below 10 mL/min/1.73 m², aiming to start dialysis at GFR 7-8 mL/min/1.73 m²
- Allow 2-4 weeks between insertion and routine dialysis use (for wound healing, cuff ingrowth, leak prevention)
- If urgent start is required, low-volume PD can begin within 24 hours of insertion (with the patient recumbent)
- Catheter should not be used for 10-14 days; should be flushed 2-3 times/week with saline or dialysate until training
4.5 Burying (Embedding) the Catheter (Moncrief Technique)
When the patient will not need PD immediately (e.g., pre-dialysis planning):
- Catheter inserted in standard fashion, tunneled to a 1-cm skin exit site, filled with heparin 1000 U/mL, then the external tip is redirected back into the subcutaneous space toward the midline
- Primary incision and exit site are closed over the catheter
- Benefits: tissue ingrowth into cuffs is undisturbed; no exit site to care for; eliminates early infection; catheter can be placed electively months before it is needed
- Exteriorization: small incision through original exit site, catheter located with hemostats and brought out; can be successfully exteriorized years after placement
5. EXIT SITE CARE
The exit site is where the PD catheter enters the skin. It is the first line of defense against tunnel and catheter-related infections. Proper exit site care (ESC) is one of the most important elements of PD maintenance.
5.1 Anatomy of the Exit Site and Tunnel
- Exit site: the skin opening where the catheter emerges
- Sinus tract: the tissue channel between exit site and superficial cuff
- Subcutaneous tunnel: the tissue path between the two cuffs
- A mature, healthy exit site is epithelialized, dry, non-tender, with no discharge
5.2 Post-Insertion Wound Care (Early Phase - First 4-6 Weeks)
- The original post-surgical dressing is kept in place for 5-7 days after insertion (removed only for frank bleeding or excessive drainage)
- Dressing changes performed using sterile technique by trained PD staff wearing masks
- Non-occlusive gauze dressings are preferred over transparent occlusive dressings (gauze allows drainage away from the exit site; occlusive dressings trap moisture)
- The catheter must be immobilized - taped securely to prevent traction injury (traction injury is a risk factor for exit site infection)
- The transfer set is taped separately, away from the dressing, for catheter access without disturbing the wound
- Cytotoxic agents must be avoided during healing: povidone-iodine and hydrogen peroxide damage healing tissue and should not be used
- The patient should NOT take over exit site care until the exit site is fully healed (typically 4-6 weeks)
(ISPD 2023 Catheter-Related Infection Guidelines; Children's Health Ireland PD Guideline, 2026)
5.3 Chronic/Ongoing Exit Site Care (After Healing)
Frequency: Daily exit site care using:
Step-by-step procedure:
- Wash hands thoroughly before touching the catheter
- Inspect the exit site for signs of infection: redness, swelling, crusting, sanguinous or purulent discharge, pain
- Cleanse the exit site with a non-irritating, non-toxic agent:
- Chlorhexidine gluconate 2% is widely recommended - applied in a circular outward motion (not probed into the sinus)
- Allow to air dry ~30 seconds
- Avoid iodine, hydrogen peroxide, alcohol (impair skin cell turnover)
- Apply topical prophylactic antibiotic to the exit site (see section 5.4)
- Place a sterile gauze pad under the catheter at the exit site (catheter rests on gauze, not skin)
- Apply a final sterile dressing (gauze + hypofix or mepore)
- Tape/anchor the catheter to the skin in a comfortable position, minimizing tension on the exit site; catheter and transfer set may be looped and secured with an immobilizer
Important restrictions:
- Avoid scratching or picking at the exit site or removing scabs forcibly
- Do not sleep on the abdomen
- Cover the exit site when swimming (sea water or well-maintained pools only, per ISPD physical activity guidelines)
- Masks and gloves are not required for chronic exit site care by the patient at home (clean technique); sterile technique is required during the healing phase
5.4 Topical Prophylactic Antibiotics (Exit Site)
ISPD strongly recommends daily topical application of antibiotic cream or ointment to the exit site. This is one of the most evidence-based infection prevention measures in PD:
| Agent | Organism Targeted | Notes |
|---|---|---|
| Mupirocin 2% cream/ointment | S. aureus (including MRSA) | Strongest evidence; reduces S. aureus ESI; also applied intranasally 5 days/month for nasal S. aureus carriers |
| Gentamicin 0.1% cream | Gram-negatives (Pseudomonas, Enterobacteriaceae); also staphylococci | Some reports of increased gram-negative ESI after switching from mupirocin; use with caution |
| Honey (medical-grade antibacterial) | Broad spectrum | Non-inferior to intranasal mupirocin in a randomized trial for preventing S. aureus exit site infections |
The choice between mupirocin and gentamicin depends on local microbiology and resistance patterns.
5.5 Exit Site Scoring (Assessment)
The Twardowski-Prowant classification and the ISPD numerical scoring system are used:
| Feature | 0 pts | 1 pt | 2 pts |
|---|---|---|---|
| Swelling | None | Exit only, <0.5 cm | >0.5 cm or involves tunnel |
| Crust | None | <0.5 cm | >0.5 cm |
| Redness | None | <0.5 cm | >0.5 cm |
| Pain | None | Slight | Severe |
| Drainage | None | Serous | Purulent |
Score ≥ 4 = infection assumed. Purulent drainage alone (any amount) = infection, regardless of score.
5.6 Exit Site Infection (ESI)
Organisms: S. aureus (most common), then Pseudomonas spp., other gram-negatives.
Diagnosis: Clinical - marked erythema or purulent discharge. Swab the exit site for culture. Ultrasound to assess tunnel involvement.
Treatment:
- First-line empiric (pending culture): oral agent effective against S. aureus (e.g., flucloxacillin, dicloxacillin, cloxacillin; first-gen cephalosporin if penicillin-allergic)
- Minimum 2 weeks of treatment; 3 weeks for Pseudomonas
- Pseudomonas ESI is particularly difficult - often requires two antibiotics simultaneously
- If gram-negative: ciprofloxacin 500-750 mg once daily orally
- MRSA: systemic vancomycin
- Systemically unwell: IV antibiotics ± hospitalization
- No improvement at 7 days → ultrasound to exclude tunnel abscess
- No complete healing at 4 weeks → consider cuff shaving (exteriorizing and trimming the outer cuff)
- Persistent/relapsing ESI → catheter removal (high risk of peritonitis)
5.7 Prevention Summary (ISPD Framework)
| Intervention | Evidence |
|---|---|
| Prophylactic antibiotic at catheter insertion (glycopeptide or 1st-gen cephalosporin) | Strong |
| Flush-before-fill Y-set/double-bag connectology | Strong |
| Daily topical mupirocin or gentamicin to exit site | Strong |
| Immobilization and sterile wound care post-insertion | Strong |
| Patient training and periodic retraining | Strong |
| Transfer set change after contamination | Strong |
| Prophylactic antifungals when antibiotics prescribed | Moderate |
| Exit site care continued after PD discontinuation | Recommended (ISPD 2023) |
Sources: Comprehensive Clinical Nephrology, 7th Ed. (Crabtree et al., Ch. 97/102); Brenner and Rector's The Kidney, 2-Vol Set (Ch. 68/36); NKF Primer on Kidney Diseases, 8th Ed. (Ch. 57); The Washington Manual of Medical Therapeutics; Harrison's Principles of Internal Medicine, 22nd Ed.; ISPD Catheter-Related Infection Recommendations 2023; ISPD 2024 PD-Associated Infections Update.
This is a shared conversation. Sign in to Orris to start your own chat.