Ra ,ankylospolisis txt
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Searching Images
rheumatoid arthritis joint deformity hands
Searching Images
ankylosing spondylitis bamboo spine X-ray
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content on both conditions. Let me compile the full structured answer.
Rheumatoid Arthritis (RA) vs. Ankylosing Spondylitis (AS)
RHEUMATOID ARTHRITIS (RA)
Overview
RA is a chronic inflammatory systemic disease in which cellular and autoimmune mechanisms destroy tissues, primarily the synovium. Without treatment, polyarticular, RF-positive RA has >70% chance of joint damage within 2 years. — Textbook of Family Medicine 9e
Epidemiology
| Feature | Detail |
|---|---|
| Sex ratio | Women : Men = 3 : 1 |
| Peak incidence | 20–50 years |
| Prevalence | 1–2% of adults |
| Genetics | HLA-DR association (MHC class II) |
Pathophysiology
An inciting event (possibly infectious) triggers synovial lining cell proliferation, forming a pannus. Leukocyte invasion follows, with a cascade involving proteases and cytokines. Rheumatoid factor (RF) = autoantibody to IgG Fc fragment — associated with more severe extraarticular disease.
Clinical Features
- Onset: Insidious in 70%, acute in 10%, intermediate in 20%
- Hallmark: Symmetric synovitis + morning stiffness >1 hour
- Joints affected first: Small joints — PIP, MCP (hands/feet); DIP joints are spared
- Constitutional symptoms: Fatigue, malaise, weight loss, low-grade fever, anemia
- Cervical spine: C1–C2 instability (transverse ligament tenosynovitis) — can cause neurological complications
- Classic late deformities:
- Swan neck: PIP hyperextension + DIP flexion
- Boutonnière: PIP flexion + DIP hyperextension
- Ulnar deviation at MCP joints
- Z-thumb deformity
Extraarticular Manifestations
- Rheumatoid nodules (subcutaneous, over pressure points)
- Rheumatoid vasculitis
- Pulmonary (pleural effusion, interstitial fibrosis)
- Cardiac (pericarditis)
- Ocular (Sjögren's syndrome, scleritis)
- Felty's syndrome (RA + splenomegaly + neutropenia)
Diagnosis — ACR 1987 Criteria (≥4 required, criteria 1–4 must be ≥6 weeks)
- Morning stiffness ≥1 hour
- Arthritis in ≥3 joint areas
- Arthritis of hand joints (wrist, MCP, or PIP)
- Symmetric arthritis
- Rheumatoid nodules
- Serum RF positive
- Radiographic erosions / periarticular osteoporosis
Investigations
- RF (not specific — positive in normals too)
- Anti-CCP (more specific)
- CBC: normocytic anemia, elevated ESR/CRP
- Synovial fluid: >2000 WBCs/mm³, no crystals
- X-ray: periarticular osteopenia → joint space narrowing → erosions (appears months–1 year after onset)
Treatment
Step 1 — DMARDs (Disease-Modifying): Start early; slow/halt joint destruction
- Methotrexate (MTX) — first-line DMARD; weekly dosing; requires folic acid supplementation; monitor LFTs
- Hydroxychloroquine (Plaquenil) — mild disease; monitor for retinal toxicity
- Sulfasalazine — moderate disease
- Leflunomide — alternative to MTX
Step 2 — Biologics (for MTX-refractory disease):
- Anti-TNF-α: Etanercept (SC weekly), Infliximab (IV q4–8 weeks, must be combined with MTX), Adalimumab (SC q2 weeks)
- Screen for TB (PPD) before starting biologics; treat latent TB with isoniazid ×9 months
Adjuncts:
- NSAIDs: Symptom control only; do not alter disease progression; risk of GI bleed
- Glucocorticoids: Bridge therapy while awaiting DMARD onset; intraarticular injections (≤3×/year per joint)
RA Hand X-ray — classic changes:

Bilateral hand X-ray: ulnar deviation, MCP joint space narrowing, subluxation, and cortical erosions — late-stage RA.

Swan-neck deformity (5th digit left hand), synovial swelling at wrist — characteristic RA hand findings.
ANKYLOSING SPONDYLITIS (AS)
Overview
AS is a chronic multisystem inflammatory spondyloarthropathy primarily affecting the axial skeleton. It belongs to the seronegative spondyloarthropathies (RF negative). Sacroiliitis and enthesitis are its hallmarks. — Grainger & Allison's Diagnostic Radiology; Textbook of Family Medicine 9e
Epidemiology
| Feature | Detail |
|---|---|
| Sex ratio | Men : Women = 5 : 1 |
| Age of onset | 20s–30s (young adults) |
| Genetics | HLA-B27 positive (strong association) |
| Peripheral joints | Involved in ~30% |
Pathophysiology
Inflammation at the annulus fibrosus–vertebral bone margin (enthesis). This is replaced by fibrocartilage, then ossified. Progressive ossification → vertebral fusion = bamboo spine (late finding). Enthesitis also occurs at ligament/tendon attachments in spine and pelvis → ossification.
Clinical Features
- Onset: Insidious low back pain, often felt in buttocks or sacroiliac area
- Morning stiffness relieved by activity (not rest — opposite to mechanical back pain)
- Pain relieved by hot shower or exercise
- Can disturb sleep → fatigue, malaise, low-grade fever, weight loss
- Key clue: Back stiffness in a man <40 years, relieved by exercise, persistent
- Juvenile onset: hip and shoulder symptoms may predominate
- Decreased spinal mobility (early = pain/spasm; late = ankylosis)
- Chest expansion reduced (costovertebral joint involvement → diaphragmatic breathing)
Extraarticular Manifestations
| System | Manifestation |
|---|---|
| Eyes | Acute anterior uveitis (iritis) — most common |
| Cardiovascular | Aortitis, aortic regurgitation |
| Pulmonary | Upper lobe bilateral fibrobullous disease (late) |
| Neurological | Cervical fractures from minor trauma |
Diagnosis
- Clinical: History + physical + radiology
- Physical exam: Palpation of sacroiliac joints; Schober's test (spinal mobility)
- Imaging:
- Plain X-ray: sacroiliitis (bilateral, symmetric) → erosions → sclerosis → ankylosis; vertebral squaring; Romanus lesions (sclerotic 'shiny' corners); bamboo spine (late)
- MRI: Earliest detection — subchondral bone marrow edema at SI joints and vertebral corners (before X-ray changes)
- CT: confirms erosive change and sclerosis
- Labs: HLA-B27 positive (not diagnostic alone); ESR/CRP elevated; RF negative
Radiological Progression
- Romanus lesions — sclerotic shiny corners of vertebral bodies (enthesitis at Sharpey fibers)
- Vertebral squaring — due to erosion + anterior longitudinal ligament ossification
- Syndesmophytes — vertical, thin, bilateral, marginal (annulus fibrosus ossification)
- Bamboo spine — complete bony fusion of spine (end-stage)
- Sacroiliac joints — bilateral symmetric ankylosis
Treatment
- NSAIDs — mainstay; 70–80% report substantial relief; continuous use may slow radiographic progression
- Biologics: Anti-TNF agents (e.g., etanercept, adalimumab) for NSAID-refractory disease
- Physiotherapy: Back extensor strengthening; maintain erect posture; swim for exercise; firm mattress; sleep with spine extended
- Corticosteroids: NOT generally helpful for axial disease
- Supervised group exercise > home exercise > no exercise
- No role for splints or braces
AS — Bamboo spine X-ray:

Lateral lumbosacral X-ray: classic bamboo spine — vertical marginal syndesmophytes, vertebral fusion, loss of lumbar lordosis — end-stage AS.

AP pelvis + lumbar spine: bamboo spine (blue arrows) + bilateral SI joint ankylosis (red arrows).
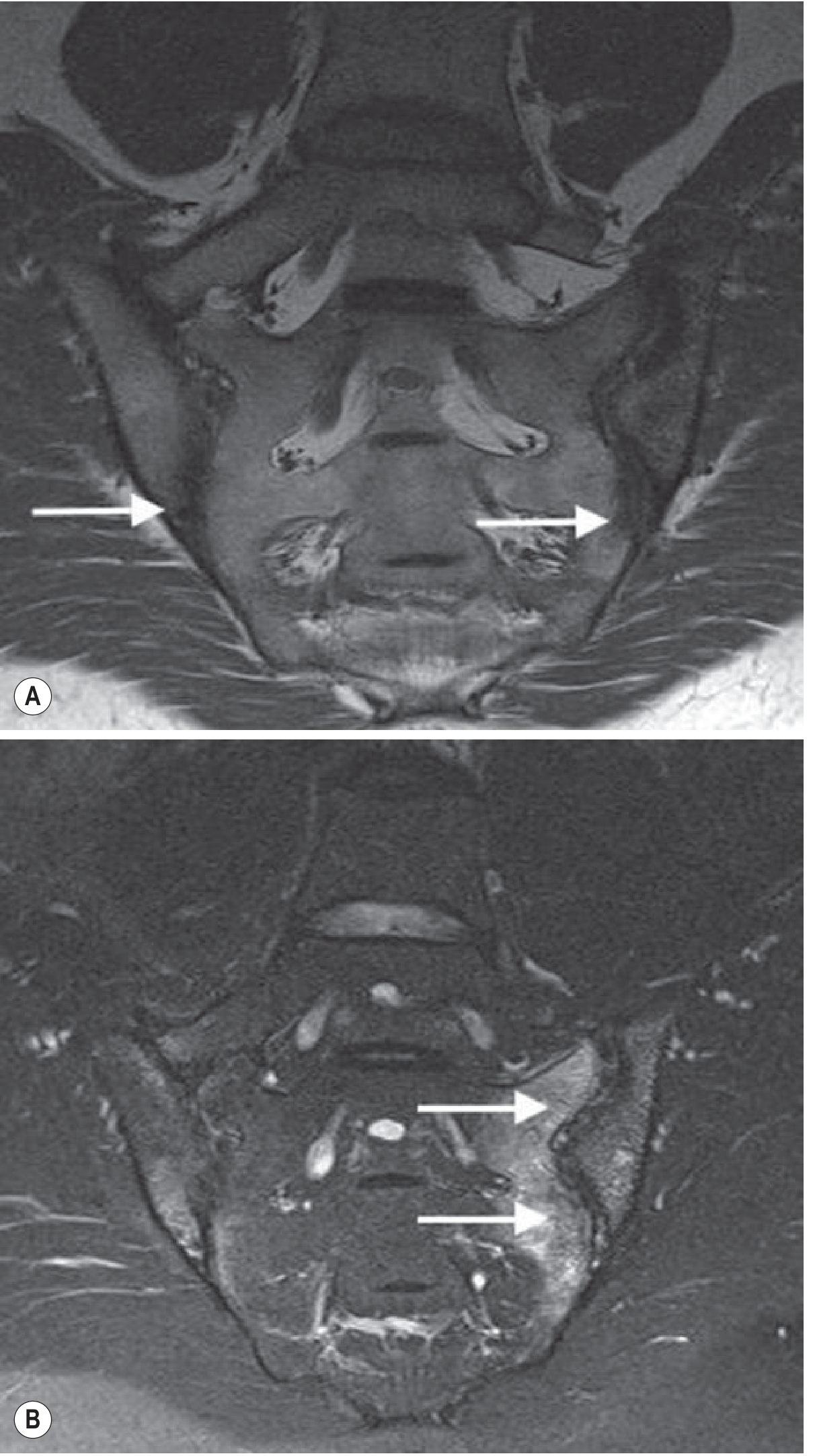
MRI of SI joints in AS: T1 shows erosions with joint space loss; T2 fat-suppressed shows extensive subchondral edema (disease activity).
KEY COMPARISON TABLE: RA vs. AS
| Feature | RA | AS |
|---|---|---|
| Type | Systemic autoimmune | Seronegative spondyloarthropathy |
| Sex | F > M (3:1) | M > F (5:1) |
| Age | 20–50 (any age) | 20s–30s |
| Genetics | HLA-DR | HLA-B27 |
| Joints | Peripheral (small joints) — symmetric | Axial skeleton (SI joints, spine) |
| DIP joints | Spared | Can be involved (if peripheral) |
| Morning stiffness | >1 hour, worsens with activity | Improves with activity |
| RF | Positive (70%) | Negative (seronegative) |
| Key X-ray finding | Periarticular erosions, ulnar deviation | Bamboo spine, sacroiliitis |
| Hallmark pathology | Pannus formation, synovitis | Enthesitis, syndesmophytes |
| Eye involvement | Sjögren's, scleritis | Acute anterior uveitis (iritis) |
| Treatment | MTX + biologics (anti-TNF) | NSAIDs + anti-TNF; physiotherapy |
| Corticosteroids | Bridge therapy (systemic/local) | Not helpful for axial disease |
Sources: Textbook of Family Medicine 9e, p. 878–884; Grainger & Allison's Diagnostic Radiology, p. 1119–1120
This is a shared conversation. Sign in to Orris to start your own chat.