Explain me about furosemide(lasix) its mechanisms of action in diuretics and it mechanism in pulmonary edema. Time taken for its onset of action?. How long does the action last?. How long does it take for the patient to urinate?
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Loading Image
I now have all the key information needed. Let me compile a thorough answer.
Furosemide (Lasix) - Complete Pharmacology
What is Furosemide?
Furosemide (brand name Lasix) is the most commonly used loop diuretic. It belongs to a class that includes bumetanide, torsemide, and ethacrynic acid. The name "Lasix" directly encodes its duration - it "lasts six" hours. It is the drug of choice for treating pulmonary edema, acute/chronic peripheral edema from heart failure, and renal impairment.
1. Mechanism of Action as a Diuretic
Furosemide works at the thick ascending limb of the Loop of Henle in the nephron.
Molecular target: It inhibits the Na⁺/K⁺/2Cl⁻ cotransporter (NKCC2) located on the luminal (apical) membrane of tubular cells in the ascending limb.
Step-by-step mechanism:
- Furosemide is secreted into the tubular lumen at the proximal convoluted tubule (this is how it reaches its site of action - it must be excreted into the urine to work).
- It binds to and blocks NKCC2, preventing the reabsorption of Na⁺, K⁺, and Cl⁻ from the tubular fluid into the renal medulla.
- This lowers the osmotic pressure in the medulla, so less water is reabsorbed from water-permeable segments (like the descending loop of Henle).
- The result is a large increase in urinary output of Na⁺, Cl⁻, K⁺, water, Ca²⁺, and Mg²⁺.
Why is it the most powerful diuretic?
- The ascending limb normally reabsorbs 25-30% of all filtered NaCl. Downstream nephron segments (distal tubule, collecting duct) cannot compensate for this flood of extra Na⁺, so the diuretic effect is massive.
- No other class of diuretic achieves this magnitude of sodium and water excretion.
Important note: NSAIDs (like ibuprofen) inhibit renal prostaglandin synthesis and can blunt furosemide's diuretic action.
Dose-response curve: Furosemide follows a sigmoidal ("S"-shaped) curve with three zones:
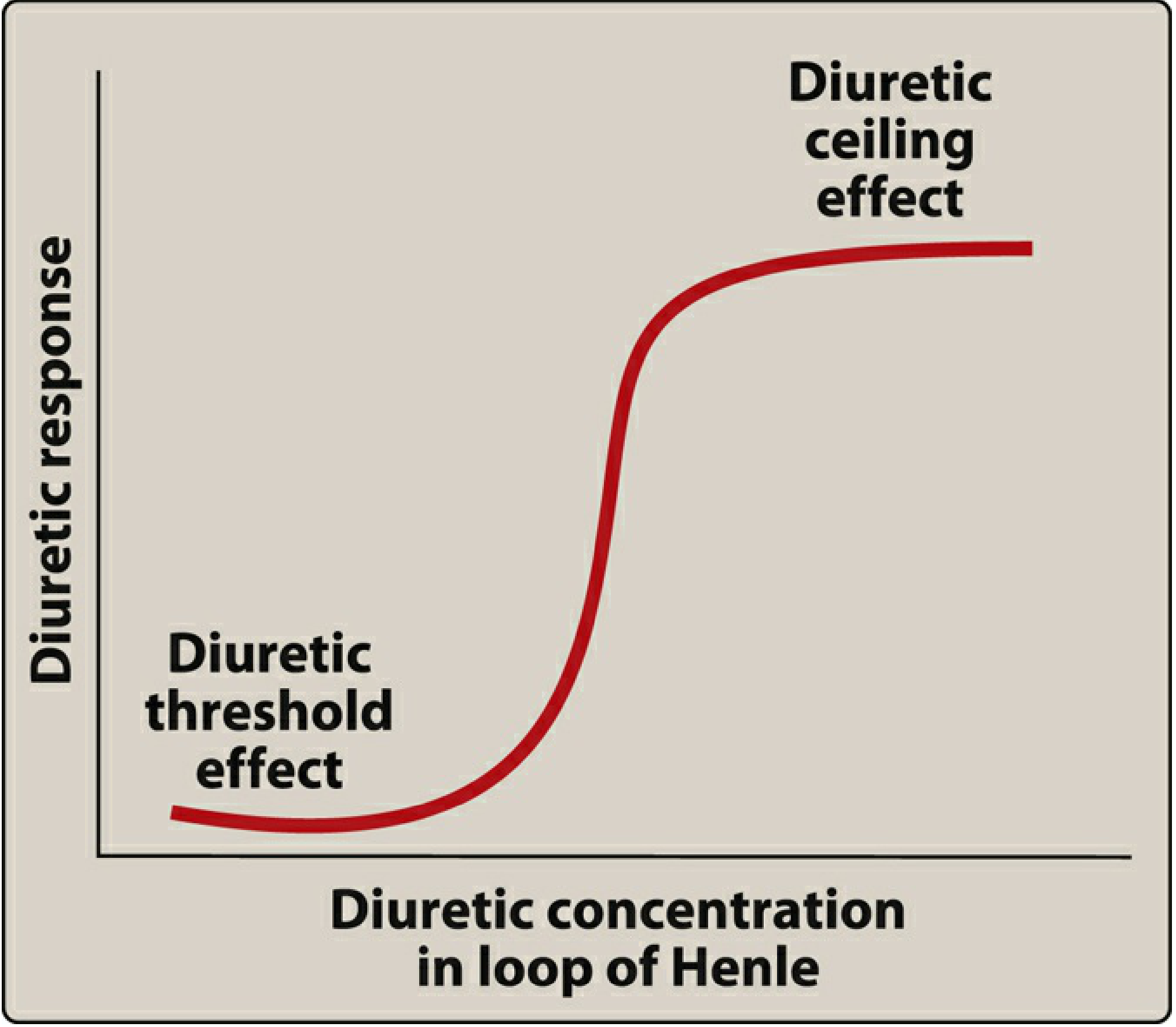
- Below the threshold: no diuresis occurs
- Steep middle zone: small dose increases produce large diuresis
- Ceiling effect: increasing the dose beyond a point produces no additional diuresis - instead, increase the frequency of dosing
2. Mechanism in Pulmonary Edema
In acute pulmonary edema, furosemide works through two distinct mechanisms - and importantly, the first one acts even before significant diuresis begins:
A. Rapid Venodilation (within minutes - before diuresis)
- IV furosemide causes immediate venodilation (dilation of venous capacitance vessels) by stimulating release of prostaglandins (particularly PGE₂) from the kidney and vascular endothelium.
- This reduces venous return to the heart (preload), rapidly lowering pulmonary capillary wedge pressure.
- Fluid is pulled back from the congested pulmonary capillaries into the venous system.
- This is why patients with acute pulmonary edema feel relief of dyspnea within 5-15 minutes of IV furosemide - before any significant urination has occurred.
B. Diuresis (over subsequent 30-60 minutes)
- The kidney effect then kicks in: inhibition of NKCC2 causes massive Na⁺ and water excretion.
- This reduces total circulating blood volume, further dropping preload and pulmonary congestion.
- The lungs "dry out" as fluid is mobilized from the alveolar interstitium and capillaries into the circulation and then excreted.
Together, these two mechanisms make furosemide the drug of choice for acute pulmonary edema. It can excrete up to 25% of filtered sodium when given intravenously.
3. Onset of Action
| Route | Onset of Action |
|---|---|
| Intravenous (IV) | 5 minutes (venodilation begins almost immediately; diuresis within 30-60 min) |
| Oral | 30-60 minutes |
| Intramuscular (IM) | ~30 minutes |
- IV furosemide provides rapid onset and avoids the unpredictable oral bioavailability (which ranges from 10% to 90% - highly variable). This is why IV is preferred in emergencies like acute pulmonary edema.
- Bumetanide and torsemide have more reliable oral bioavailability (80-100%), making them preferred when oral therapy is needed.
4. Duration of Action
| Drug | Duration |
|---|---|
| Furosemide | ~6 hours |
| Bumetanide | ~6 hours |
| Torsemide | Moderately longer than 6 hours |
The brand name Lasix literally means "lasts six" - a memory aid for its 6-hour duration. This predictable window allows patients and clinicians to plan the period of active diuresis.
5. When Does the Patient Urinate?
| Route | Time to Urination |
|---|---|
| IV furosemide | Within 30-60 minutes (often as early as 15-20 min in practice) |
| Oral furosemide | Within 1-2 hours |
- After IV administration, peak diuresis typically occurs at 1-2 hours.
- After oral administration, peak diuresis occurs around 1-2 hours after absorption.
- The entire active diuretic window lasts ~6 hours, after which urine output returns toward baseline.
Clinical tip for dosing timing: Because the diuretic window is predictable (6 hours), patients are usually advised to take their oral furosemide in the morning (or morning + early afternoon if twice daily) to avoid disruptive nighttime urination.
Summary Table
| Parameter | IV Furosemide | Oral Furosemide |
|---|---|---|
| Onset of action | 5 min (venodilation); 30-60 min (diuresis) | 30-60 min |
| Time to urinate | ~15-60 min | ~1-2 hours |
| Peak effect | 1-2 hours | 1-2 hours |
| Duration of action | ~6 hours | ~6 hours |
| Bioavailability | 100% (IV) | Unpredictable (10-90%) |
Sources: Lippincott Illustrated Reviews: Pharmacology, p. 337-341 | Braunwald's Heart Disease, 15th Ed., Chapter 49 | Fuster & Hurst's The Heart, 15th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.