MUHS 2nd MBBS Pathology - Cardiovascular System: Complete Exam Notes
Source: Robbins & Kumar Pathologic Basis of Disease (9e) | Robbins & Kumar Basic Pathology | Harshmohan Pathology correlation included
TOPIC 1: ISCHEMIC HEART DISEASE (IHD) - Classification
Definition
IHD is a group of syndromes caused by an imbalance between myocardial oxygen supply and demand, most commonly (>90%) due to obstructive coronary atherosclerosis.
Classification of IHD (MUHS Exam High Yield)
IHD
├── 1. Angina Pectoris
│ ├── Stable angina (exertional)
│ ├── Unstable angina (crescendo/pre-infarction)
│ └── Prinzmetal / Vasospastic angina
├── 2. Myocardial Infarction (MI)
│ ├── STEMI (ST-elevation MI)
│ └── NSTEMI (Non-ST elevation MI)
├── 3. Chronic IHD with CHF (Ischemic cardiomyopathy)
└── 4. Sudden Cardiac Death (SCD)
Acute Coronary Syndrome = Unstable Angina + STEMI + NSTEMI + SCD
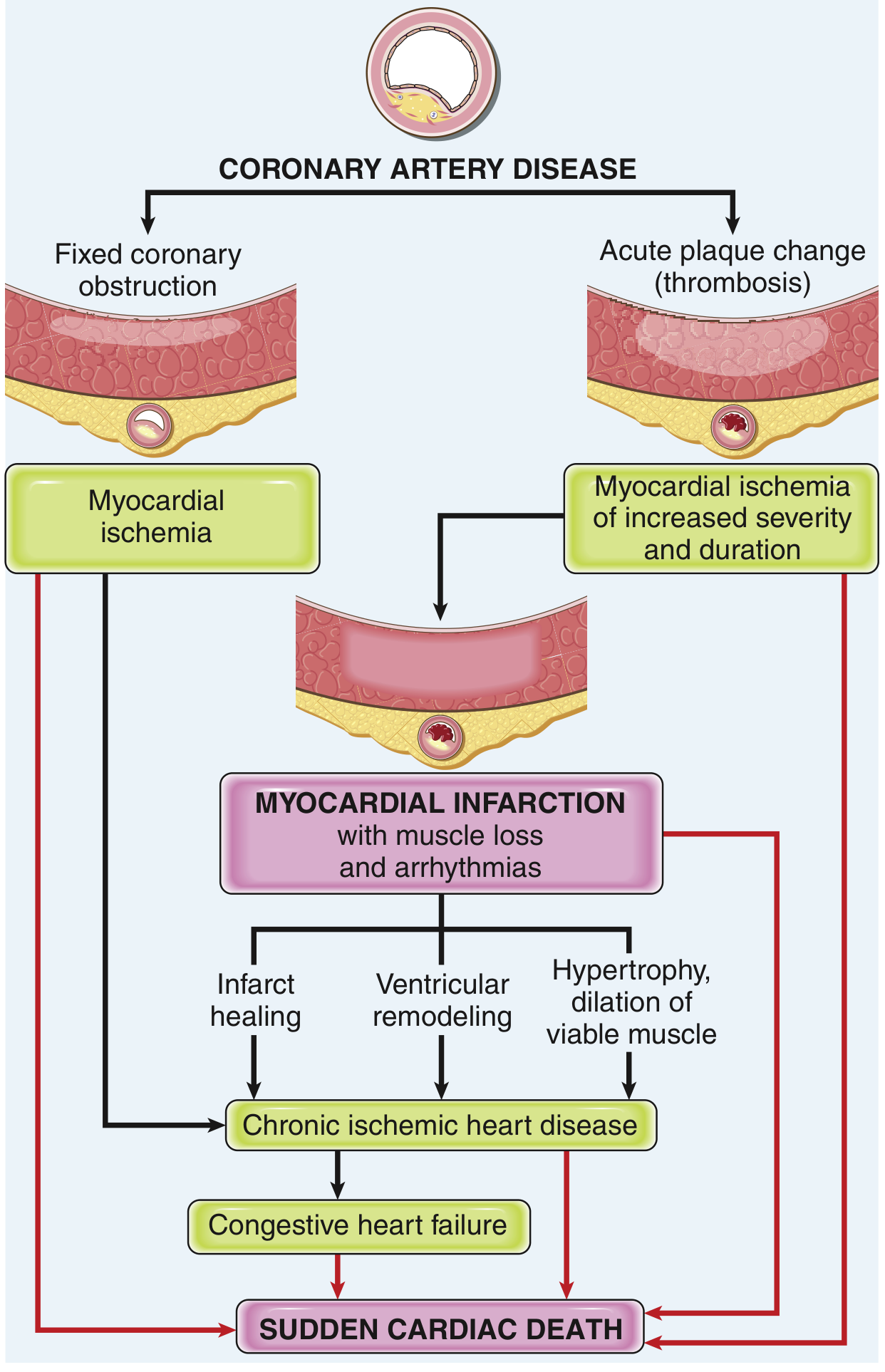
Pathogenesis of IHD
Fig. Pathways in progression of IHD - Robbins & Kumar, Pathologic Basis of Disease
Two mechanisms lead to inadequate coronary perfusion:
- Fixed ("preexisting") atherosclerotic occlusion - slowly progressive; causes stable angina
- Acute plaque change + superimposed thrombosis/vasospasm - causes MI, unstable angina, SCD
TOPIC 2: MYOCARDIAL INFARCTION (MI)
Definition of Infarct
An infarct is an area of ischemic coagulative necrosis in a tissue/organ resulting from sudden, severe reduction in its blood supply, usually due to arterial occlusion.
In the heart: MI is the death of cardiac muscle (coagulative necrosis) due to prolonged ischemia (usually >20-40 min of severe ischemia).
Pathogenesis of MI
Typical Sequence:
- Atheromatous plaque disrupted by endothelial injury, intraplaque hemorrhage, or shear forces
- Subendothelial collagen + necrotic plaque contents exposed to blood
- Platelet adhesion, aggregation, activation → release of TXA2, ADP, serotonin → vasospasm
- Coagulation activation by tissue factor → growing thrombus
- Within minutes → complete coronary occlusion → ischemia → necrosis
90% of MIs are due to coronary atherothrombosis. Angiography within 4 hours shows thrombosis in ~90% of STEMI cases.
Less common causes (10%):
- Coronary vasospasm (cocaine, ephedrine)
- Emboli (from mural thrombus in AF, IE vegetations, prosthetic valves)
- Vasculitis, sickle cell disease, amyloid deposition
Morphological Changes in MI as per Age of Infarct
This is the most asked topic in MUHS exams. Memorize the timeline:
| Time After Onset | Gross Appearance | Microscopic Appearance |
|---|
| 0 - 4 hours | No visible change (normal) | No change on routine H&E |
| 4 - 12 hours | Occasional dark mottling | Early coagulative necrosis; edema; wavy fibers; early neutrophil infiltration |
| 12 - 24 hours | Dark mottling; pallor begins | Coagulative necrosis with loss of nuclei and striations; neutrophil infiltration |
| 1 - 3 days | Pallor / yellow-tan area | Dense neutrophil infiltration; coagulative necrosis; karyolysis |
| 3 - 7 days | Hyperemic (red) border; yellow-tan center (soft) | Macrophage infiltration begins; phagocytosis of dead cells; disintegration of necrotic fibers |
| 1 - 2 weeks | Yellow-tan; hyperemic border; soft | Granulation tissue forms at margins; vascular proliferation; collagen deposition begins |
| 2 - 8 weeks | Gray-white scar formation | Progressive fibrosis; collagen replaces granulation tissue |
| > 2 months | White fibrous scar (firm) | Dense collagenous fibrous scar (complete healing) |
Exam Tip (MUHS): Earliest change visible on electron microscopy = swelling of mitochondria + amorphous densities in matrix within 30 minutes. First light microscopy change = wavy myocyte fibers at 4-12 hrs.
Key Microscopic Stages:
Phase 1 (Necrosis - 0-4 days):
- Coagulative necrosis - cell outlines preserved but nucleus lost
- Karyolysis (nuclear dissolution)
- Dense neutrophil infiltration (neutrophils peak at 24-48 hrs)
- "Wavy fiber" change at edges (due to stretching of viable myocytes)
Phase 2 (Removal - 5-10 days):
- Macrophages replace neutrophils (mononuclear cells)
- Phagocytosis of dead debris
- Most vulnerable time for rupture!
Phase 3 (Repair - 1-8 weeks):
- Granulation tissue at periphery
- Angiogenesis (new capillary buds)
- Fibroblast proliferation
- Collagen deposition
Phase 4 (Scar - >2 months):
- Dense collagenous scar
- Thin gray-white fibrous tissue
Laboratory Diagnosis / Evaluation of MI
Cardiac Biomarkers (Enzymes used in diagnosis)
| Enzyme/Marker | Rises | Peaks | Returns to Normal | Comments |
|---|
| Troponin I / T ⭐ | 3-6 hrs | 24-48 hrs | 7-10 days (cTnI) / 10-14 days (cTnT) | Most sensitive & specific; GOLD STANDARD |
| CK-MB (Creatine Kinase-MB) | 3-6 hrs | 24 hrs | 48-72 hrs | Best for re-infarction detection; cardiac-specific isoform |
| Myoglobin | 1-3 hrs | 4-6 hrs | 24 hrs | FIRST to rise; not cardiac-specific; useful for early rule-out |
| LDH (LDH1 > LDH2) | 24-48 hrs | 3-6 days | 8-14 days | "Flip pattern" of LDH1 > LDH2; useful in late presentation |
| SGOT (AST) | 6-8 hrs | 24-48 hrs | 3-4 days | Not cardiac-specific |
MUHS Exam Key Points:
- Troponin = gold standard for MI diagnosis (most sensitive and specific)
- CK-MB = best marker for detecting re-infarction (returns to normal quickly)
- Myoglobin = earliest marker (rises within 1-3 hrs)
- LDH "flip" = LDH1 > LDH2 (normally LDH2 > LDH1) - diagnostic of MI
Other Lab Findings:
- ECG changes: ST elevation (STEMI), ST depression (NSTEMI), Q waves (transmural infarct)
- Leukocytosis: neutrophilia within 24-48 hrs
- ESR elevation: raised (due to inflammatory response)
- Echocardiography: wall motion abnormalities
- Imaging: Coronary angiography (gold standard for CAD)
Gross Appearance of MI
Types:
- Transmural MI: Full thickness of wall - due to complete coronary occlusion
- Subendocardial MI: Inner 1/3 of myocardium - due to hypoperfusion/shock
Typical Site:
- LAD occlusion → Anterior wall + anterior septum of LV (most common)
- RCA occlusion → Posterior wall + posterior septum of LV + RV
- LCX occlusion → Lateral wall of LV
Gross sequence:
- 0-12 hours: Normal or slightly pale area
- 12-24 hours: Pale, slightly mottled area
- 1-3 days: Pale yellow-tan, hyperemic border (red-brown rim)
- 3-7 days: Central yellow-tan softening, prominent red hyperemic border
- 1-2 weeks: Depressed, red-brown gelatinous area (granulation)
- Weeks-months: Gray-white fibrous scar
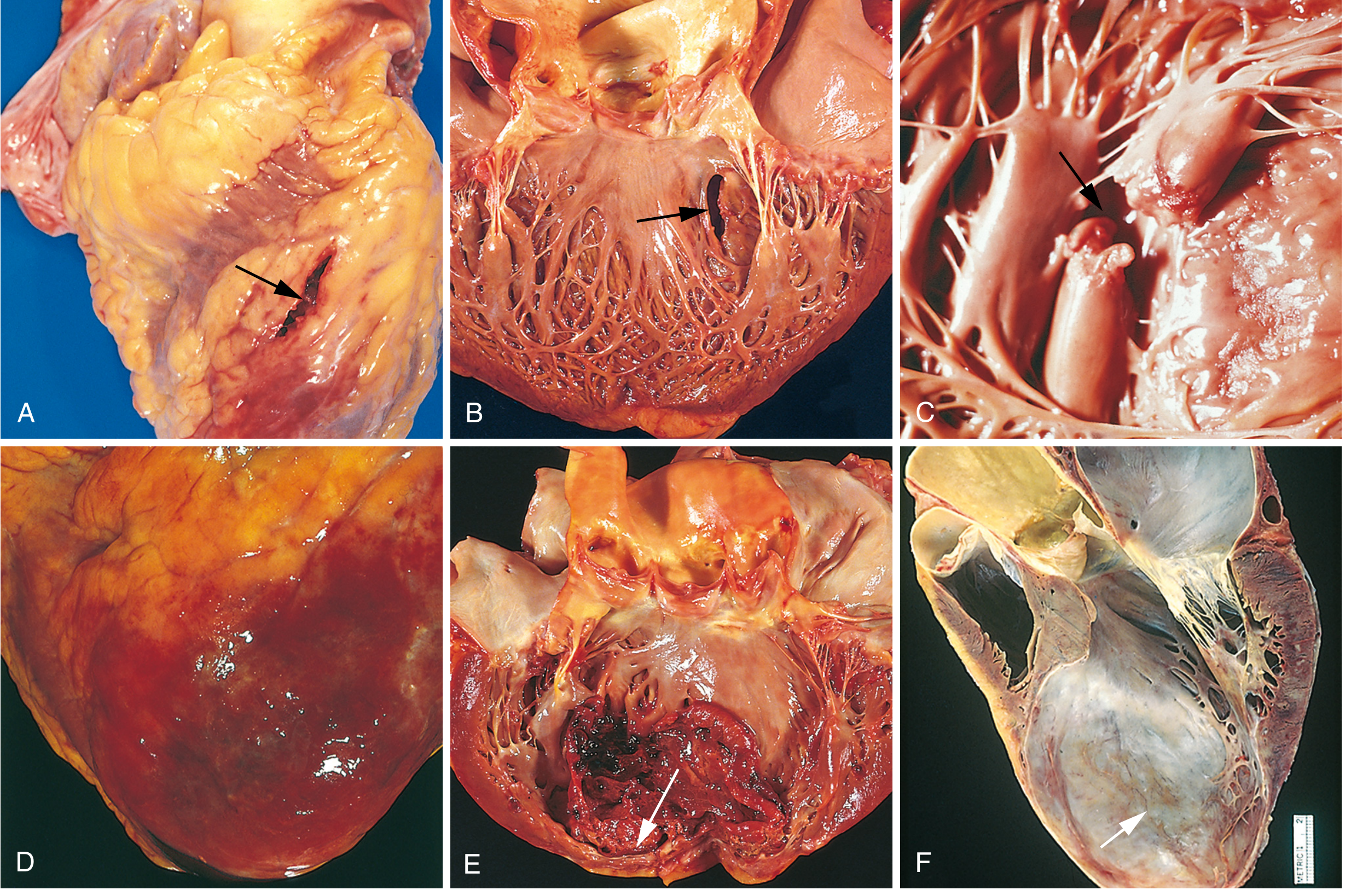
Fig. Complications of MI - (A) Anterior myocardial rupture; (B) Ventricular septal rupture; (C) Papillary muscle rupture; (D) Fibrinous pericarditis; (E) Mural thrombus in LV; (F) LV aneurysm. (Robbins, Pathologic Basis of Disease)
Consequences and Complications of MI
Nearly 75% of patients experience at least one complication after acute MI:
Immediate/Early Complications (1st Week):
| Complication | Details |
|---|
| Arrhythmias | Most common cause of death within first 24-48 hrs; ventricular fibrillation commonest lethal arrhythmia; occurs due to conduction system ischemia |
| Cardiogenic Shock | Occurs in ~10% of transmural MI; when >40% LV damaged; hypotension, pulmonary edema |
| Contractile Dysfunction / LV Failure | Most common non-lethal complication; pulmonary congestion, dyspnea |
| Papillary Muscle Dysfunction | Ischemia of papillary muscle → mitral regurgitation → acute pulmonary edema |
| Right Ventricular Infarction | Complicates inferior MI (RCA territory); presents with raised JVP but clear lungs |
Late Complications (After 1st Week):
| Complication | Time Frame | Details |
|---|
| Myocardial Rupture | 3-7 days (peak) | Most dangerous; occurs when softening is maximal; free wall rupture → haemopericardium + cardiac tamponade; septal rupture → VSD; papillary rupture → acute MR |
| Fibrinous Pericarditis (Dressler Syndrome) | 2-10 weeks post-MI | Immune-mediated; fever, pleuritic chest pain, pericardial rub |
| Mural Thrombus | 1-2 weeks | Blood clot on endocardium over infarct → risk of systemic embolism (stroke, renal infarction) |
| Ventricular Aneurysm | Weeks-months | Bulging, thin-walled fibrous scar; no rupture risk (unlike pseudoaneurysm); causes CHF, arrhythmias, mural thrombus |
| Progressive CHF (Ischemic Cardiomyopathy) | Months-years | Chronic pump failure due to infarct + remodeling |
Summary Diagram of MI Complications:
MYOCARDIAL INFARCTION
│
├─ EARLY (1-7 days)
│ ├─ Arrhythmias (VF → Sudden Death) ⭐
│ ├─ Cardiogenic shock (>40% LV damage)
│ ├─ Acute LV failure / pulmonary edema
│ ├─ Papillary muscle dysfunction → MR
│ └─ Right ventricular infarction
│
├─ INTERMEDIATE (3-14 days)
│ ├─ Myocardial RUPTURE (free wall → tamponade)
│ ├─ Ventricular SEPTAL RUPTURE → VSD
│ ├─ Papillary RUPTURE → acute MR
│ └─ Mural thrombus → embolism
│
└─ LATE (weeks-months)
├─ Fibrinous pericarditis / Dressler syndrome
├─ Ventricular aneurysm
└─ Chronic IHD / CHF
TOPIC 3: HYPERTENSIVE HEART DISEASE - Morphology
Definition
HHD results from pressure overload on the heart caused by systemic hypertension. Diagnostic criteria:
- Left ventricular hypertrophy in the absence of other cardiovascular pathology
- Clinical history or pathologic evidence of hypertension in other organs (kidneys)
Morphology
GROSS:
- Concentric left ventricular hypertrophy (increased wall thickness WITHOUT early dilation)
- Heart weight may exceed 500 g (normal 320-360 g for a 60-70 kg individual)
- LV wall thickness may exceed 2.0 cm (normal 1.2-1.4 cm)
- Left atrial dilation (due to stiff LV impairing diastolic filling)
- In long-standing decompensated disease: LV dilation (eccentric hypertrophy)
- Right-sided changes: RV hypertrophy in pulmonary hypertension (Cor Pulmonale)
MICROSCOPIC:
- Increased transverse diameter of cardiomyocytes (hypertrophy)
- Nuclear enlargement and hyperchromasia - "boxcar nuclei" (prominent, enlarged, squared-off nuclei)
- Interstitial fibrosis (perivascular and interstitial connective tissue increase)
- Thickened intramural coronary arteries (medial hypertrophy)
Clinical Features:
- Asymptomatic initially (detected on ECG/echo as LV hypertrophy)
- May present with atrial fibrillation (due to left atrial dilation)
- Progressive CHF
- Higher risk of MI, sudden cardiac death, ventricular arrhythmias, stroke
HYPERTENSIVE HEART DISEASE - KEY POINTS
Systemic Hypertension
↓
Pressure Overload on LV
↓
Concentric LV Hypertrophy (adaptive)
- Heart wt >500g
- LV wall >2.0 cm
- Boxcar nuclei
- Interstitial fibrosis
↓
Diastolic Dysfunction → LA Dilation → AF
↓
Progressive pump failure → CHF / SCD
TOPIC 4: RHEUMATIC HEART DISEASE (RHD)
Etiopathogenesis
Etiology:
- Preceded by Group A beta-hemolytic Streptococcal pharyngitis (Streptococcus pyogenes)
- Latent period: 2-3 weeks between throat infection and symptoms of acute rheumatic fever (ARF)
- Occurs in 0.3-3% of patients with streptococcal pharyngitis
Pathogenesis - Molecular Mimicry (Cross-Reactivity Hypothesis):
- Streptococcal M protein antigens are similar to cardiac antigens (myosin, tropomyosin, sarcolemmal proteins, valvular glycoproteins)
- Antibodies + CD4+ T cells raised against Streptococcal M proteins cross-react with cardiac proteins
- Antibody binding activates complement and Fc-receptor cells (neutrophils, macrophages)
- T cells stimulate cytokine production → macrophage activation → Aschoff bodies
- Streptococci are absent from the lesions (purely immunologic damage)
- Genetic susceptibility: certain HLA alleles predispose to cross-reactive immune responses
Group A Strep Pharyngitis
↓
Anti-Strep Antibodies (esp. anti-M protein)
↓
MOLECULAR MIMICRY
(Cross-reaction with cardiac antigens: myosin, sarcolemma, valve glycoproteins)
↓
T-cell and Antibody-mediated cardiac injury
↓
ACUTE RHEUMATIC FEVER → PANCARDITIS
↓
Repeated attacks → CHRONIC RHD
Morphology of Acute Rheumatic Fever - Pancarditis
PERICARDITIS:
- "Bread and butter" pericarditis - fibrinous pericarditis with characteristic shaggy exudate
- Usually resolves without significant sequelae
MYOCARDITIS:
- Aschoff Bodies (pathognomonic lesion of acute RF) - circumscribed granulomatous foci containing:
- Anitschkow cells (caterpillar cells) - plump activated macrophages with:
- Abundant cytoplasm
- Large round-to-ovoid nucleus
- Central chromatin condensed into a central wavy ribbon - "caterpillar" or "owl-eye" appearance
- Occasional multinucleated giant cells (Aschoff giant cells)
- T lymphocytes, plasma cells
- Central fibrinoid necrosis
- Diffuse Aschoff body distribution in myocardium
- Interstitial edema and mononuclear infiltration
ENDOCARDITIS:
- Fibrinoid necrosis within valve cusps
- Small (1-2 mm) verrucous vegetations (verrucae) along the line of closure of valves
- MacCallum plaques: irregular subendocardial thickenings in left atrium (at posterior wall)
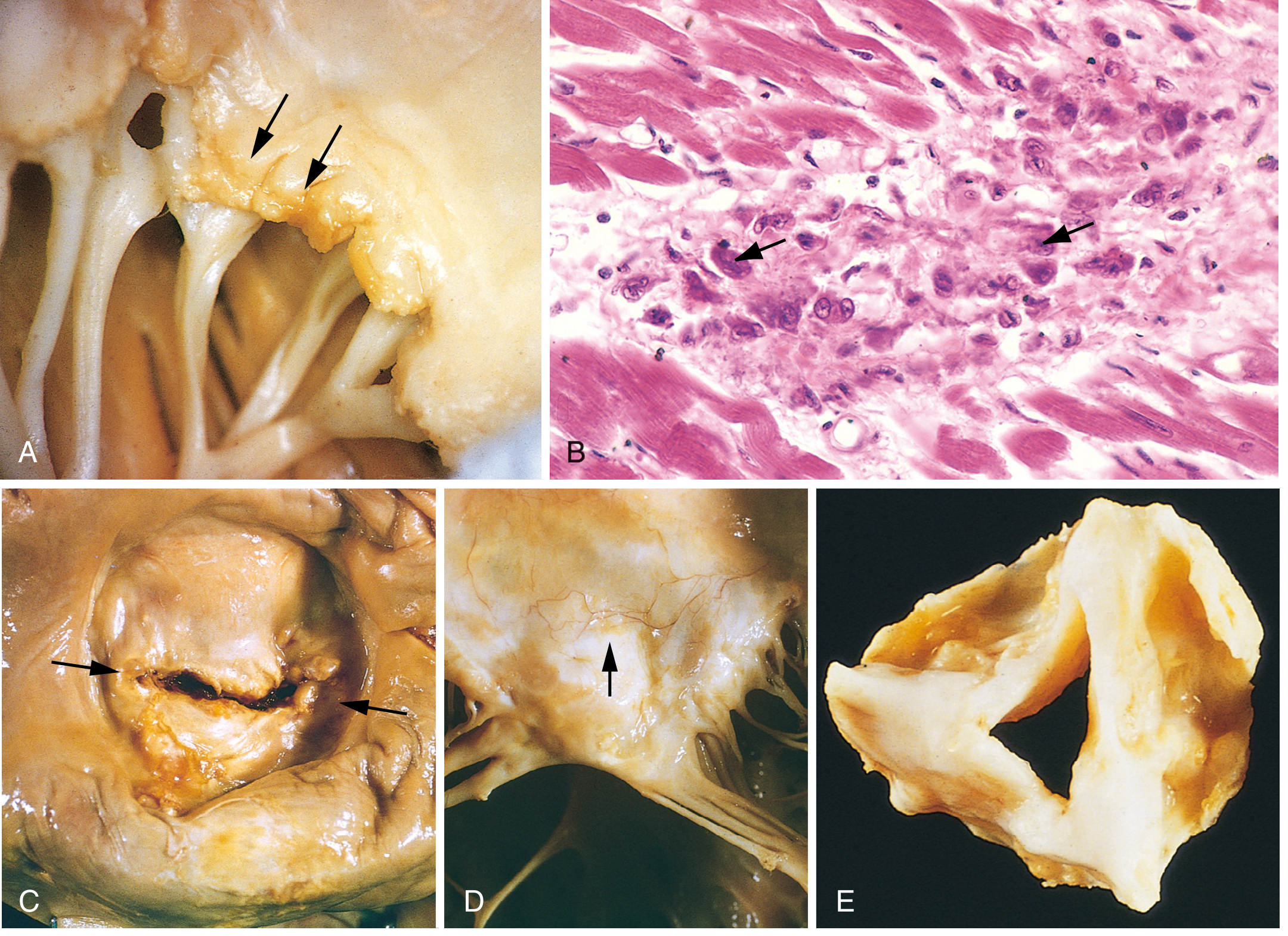
Morphology of Chronic RHD
Fig. RHD - (A) Small verrucous vegetations along mitral leaflet closure line; (B) Anitschkow cells (caterpillar cells) with wavy chromatin; (C) "Fish-mouth" mitral stenosis with commissural fusion; (D) Thickened, fused chordae tendineae; (E) Fused aortic cusps with commissural fusion - Robbins PBD
Cardinal features of mitral valve in chronic RHD:
- Leaflet thickening
- Commissural fusion and shortening → "fish-mouth" or "button-hole" stenosis
- Thickening and fusion of chordae tendineae (calcification common)
- Left atrial dilation (result of mitral stenosis/regurgitation)
Valve involvement frequency:
- Mitral alone: ~65-70%
- Mitral + Aortic: ~25%
- Tricuspid: infrequent
- Pulmonary: rare
Extracardiac Lesions in Rheumatic Heart Disease
Jones Criteria (Major) - Extracardiac manifestations:
| Lesion | Description | Notes |
|---|
| Polyarthritis | Migratory, fleeting, non-suppurative arthritis of large joints (knees, ankles, elbows, wrists) | Most common manifestation (75%); does NOT cause permanent joint damage |
| Sydenham's Chorea (St. Vitus Dance) | Involuntary, rapid, purposeless movements; emotional lability | CNS involvement; basal ganglia; usually reversible |
| Subcutaneous Nodules | Painless, firm nodules over bony prominences (elbows, wrists, occiput, knees); 0.5-2 cm | Similar histologically to Aschoff bodies; seen in severe carditis |
| Erythema Marginatum | Macular rash with erythematous serpiginous margins and pale center; evanescent; trunk and proximal limbs | Characteristic but infrequent; non-pruritic |
| Fever | Low-grade; accompanies acute episode | Minor criterion but present universally |
Minor Criteria (extracardiac):
- Fever
- Prolonged PR interval on ECG
- Raised ESR / CRP
- Leukocytosis
- Arthralgia (if arthritis is not a major criterion)
MUHS Exam Tip: Erythema Marginatum + Subcutaneous nodules are minor in UPDATED Jones criteria. The classic 5 major criteria = Carditis, Polyarthritis, Chorea, Erythema Marginatum, Subcutaneous Nodules (CEPSS mnemonic).
TOPIC 5: CAUSES OF VEGETATIONS IN HEART
Types of Vegetative Endocarditis
| Feature | Rheumatic Endocarditis | Infective (Bacterial) Endocarditis - SBE | Infective Endocarditis - ABE | NBTE (Non-Bacterial Thrombotic / Marantic) | Libman-Sacks (SLE) |
|---|
| Vegetation size | Small (1-2 mm) | Moderate (0.5-2 cm) | Large, destructive | Small to medium (1-5 mm) | Small (1-4 mm) |
| Location | Line of closure, atrial surface | Irregular; anywhere; can destroy cusp | Destructive; ring abscesses | Line of closure | Both surfaces (atrial AND ventricular) |
| Composition | Fibrin + platelets; no organisms | Fibrin + organisms (bacteria) + inflammatory cells | Fibrin + organisms + destruction | Fibrin + platelets; NO organisms, NO inflammation | Fibrin + platelets; immune complexes |
| Organism | None | Streptococcus viridans (SBE) | Staph aureus (ABE) | None | None |
| Destructive? | No | Moderate | Yes | No | No (except with hemodynamic stress) |
| Embolism | Rare | Common | Common | Can occur | Can occur |
| Sterile? | Yes | No | No | Yes | Yes |
TOPIC 6: RHEUMATIC vs. BACTERIAL ENDOCARDITIS - Differentiation
Comparison Table (MUHS Exam Favorite)
| Feature | Rheumatic Endocarditis | Subacute Bacterial Endocarditis (SBE) |
|---|
| Etiology | Immune-mediated; Strep M-protein cross-reactivity | Streptococcus viridans (most common in SBE); Enterococci |
| Predisposing factor | Group A Strep throat infection | Pre-existing valve damage (rheumatic, congenital, prosthetic) |
| Vegetation | Small (1-2 mm), warty (verrucae), firm, at line of valve closure | Larger (0.5-2 cm), irregular, friable, bulky, at any part of valve |
| Location of vegetation | Atrial surface of AV valves; along line of closure | Ventricular surface of semilunar valves; irregular location |
| Destruction | No valve destruction | Moderate valve destruction |
| Organisms in vegetation | Absent (sterile) | Present (bacteria, fungi) |
| Ring abscess | Absent | Can occur (especially in ABE) |
| Embolism | Rare | Common; septic emboli → abscesses in brain, kidney, spleen |
| Base of vegetation (Micro) | Fibrinoid necrosis | Granulation tissue (in SBE); extensive destruction in ABE |
| Healing | Fibrosis + calcification → chronic RHD | Fibrosis + scarring + valve deformity |
| MacCallum plaque | Present (left atrial endocardium) | Absent |
| Aschoff bodies | Present in myocardium | Absent |
| Systemic features | Arthritis, chorea, rash (Jones criteria) | Fever, night sweats, Osler nodes, Janeway lesions, Roth spots, splinter hemorrhages |
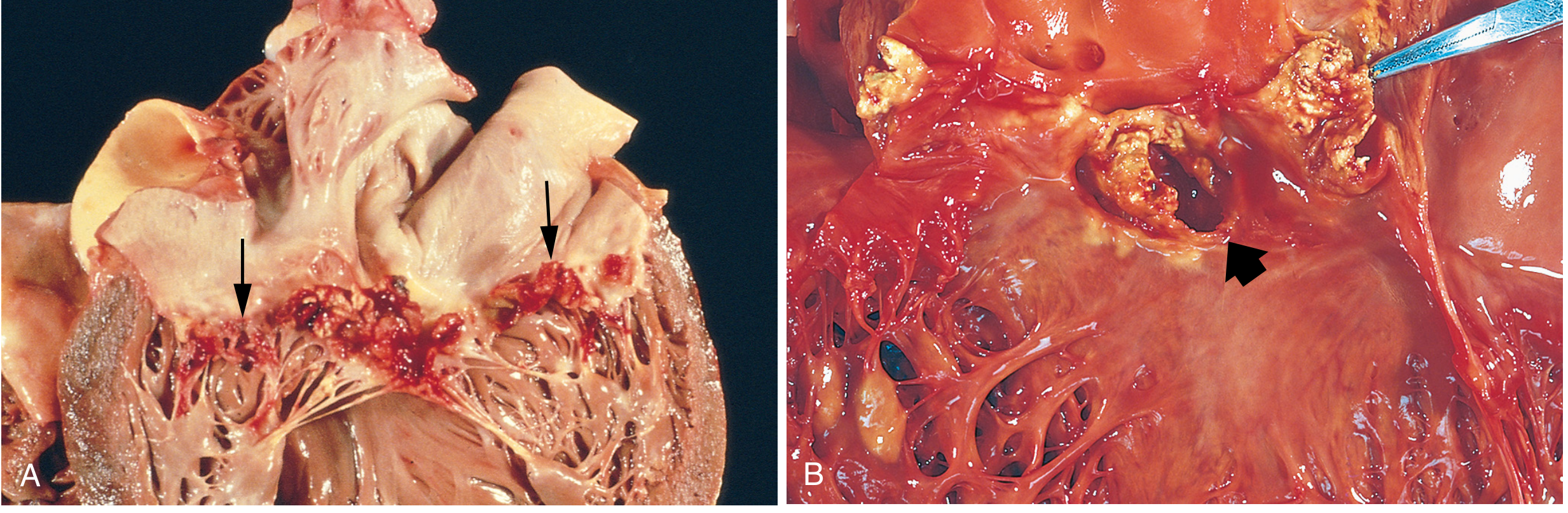
Fig. Infective Endocarditis - (A) Large, friable vegetations on mitral valve (SBE by S. viridans); (B) Acute endocarditis of bicuspid aortic valve (S. aureus) with cuspal destruction and ring abscess - Robbins PBD
Subacute Bacterial Endocarditis (SBE) - Detailed
Definition:
Infective endocarditis caused by organisms of low virulence (usually normal commensals) in patients with pre-existing valve damage, producing a slower, subacute clinical course.
Most Common Organism:
Streptococcus viridans (alpha-hemolytic streptococcus; normal oral flora)
Predisposing Conditions:
- Previously damaged valves (RHD, congenital bicuspid aortic valve, MVP)
- Dental procedures (bacteremia)
- IV drug abuse (right-sided endocarditis)
- Prosthetic valves (Staphylococcus epidermidis common)
Morphology:
- Vegetations: Irregular, friable, bulky (0.5-2 cm); contain fibrin, inflammatory cells, bacteria
- Located at irregular positions on valve leaflets
- Less destructive than acute endocarditis (ABE)
- Microscopy: Granulation tissue at base of vegetation (indicates healing/subacute nature)
- With time: fibrosis, calcification, chronic inflammatory infiltrate
Systemic/Embolic Manifestations of IE:
- Osler nodes: Painful nodules on fingertips/toes (immune complex-mediated)
- Janeway lesions: Painless hemorrhagic lesions on palms/soles (embolic)
- Roth spots: Oval retinal hemorrhages with pale centers
- Splinter hemorrhages: Linear subungual hemorrhages
- Glomerulonephritis: Antigen-antibody complex deposition
- Petechiae: On skin and mucous membranes
- Splenomegaly: Due to immune stimulation
Complications:
- Septic emboli → Brain (septic meningitis/abscess), kidneys (septic infarcts), spleen
- Mycotic aneurysms (cerebral vasculature most commonly)
- Ring abscess formation (especially ABE)
- Valvular regurgitation → acute CHF (if untreated)
QUICK REVISION TABLE - MUHS Exam
| Topic | Most Important Points |
|---|
| MI - First enzyme to rise | Myoglobin (1-3 hrs) |
| MI - Gold standard enzyme | Troponin I or T |
| MI - Best for re-infarction | CK-MB |
| MI - Earliest light microscopy change | Wavy fibers at 4-12 hrs |
| MI - Time of maximum softening/rupture risk | 3-7 days |
| MI - Complete scar formation | >2 months |
| MI - Most common cause of death in first 24 hrs | Arrhythmia (VF) |
| HHD - Gross key feature | Concentric LV hypertrophy; heart >500g; LV wall >2 cm |
| HHD - Micro key feature | Boxcar nuclei + interstitial fibrosis |
| RHD - Pathognomonic lesion | Aschoff body (Anitschkow/caterpillar cells) |
| RHD - Most affected valve | Mitral (alone in 65-70%); Mitral + Aortic in 25% |
| RHD - Extracardiac: most common | Migratory polyarthritis |
| RHD - Extracardiac: CNS | Sydenham's chorea |
| RHD vs SBE - Vegetation | RHD = small, sterile, at line of closure; SBE = large, friable, bacteria-laden |
| SBE - Most common organism | Streptococcus viridans |
| Vegetations causing embolism | SBE/ABE (infective), NBTE (Libman-Sacks less common) |
| MacCallum plaque | Subendocardial thickening of left atrial posterior wall in RHD |
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease 10e | Robbins & Kumar Basic Pathology 11e (Robbins Pathology) | Harshmohan Pathology 7e correlation throughout