examination of sinus or fistula in surgery details
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Reading File
Reading File
Reading File
I now have comprehensive material. Here is the full detailed answer:
Examination of a Sinus or Fistula in Surgery
Definitions
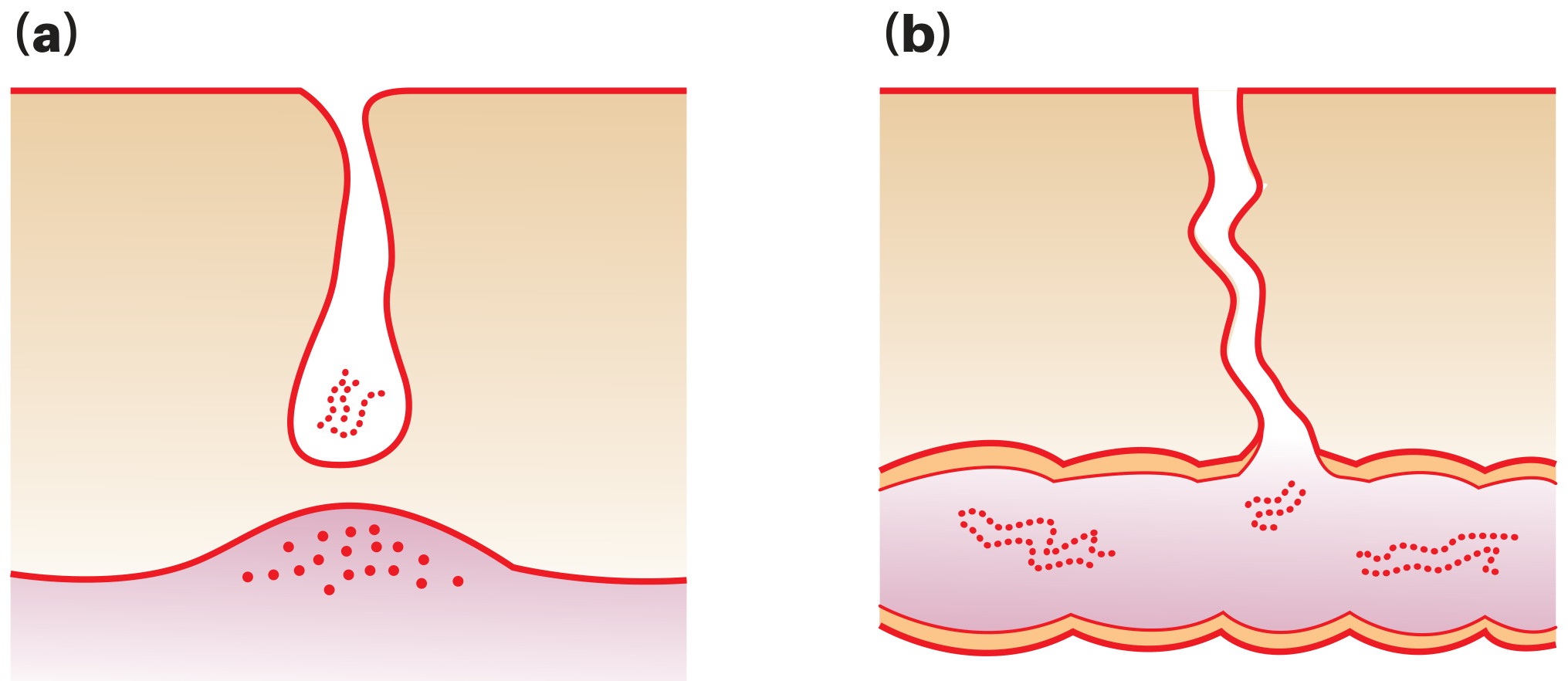
(a) Sinus - a blind-ending tract connecting a cavity lined with granulation tissue (usually an abscess cavity) to an epithelial surface. It has only ONE opening.
(b) Fistula - an abnormal communication between TWO epithelium-lined surfaces. It has an internal opening and an external opening (or connects two internal surfaces). The tract is usually lined by granulation tissue, but may become epithelialized in chronic cases.
Classification
Sinuses
| Type | Example |
|---|---|
| Congenital | Preauricular sinus |
| Traumatic | Foreign body implantation |
| Inflammatory | Osteomyelitic, tuberculous, actinomycotic |
| Neoplastic | Malignant growth with secondary infection |
| Miscellaneous | Pilonidal sinus |
Fistulae
| Type | Example |
|---|---|
| Congenital | Branchial fistula, thyroglossal fistula, tracheo-oesophageal fistula |
| Acquired - inflammatory | Crohn's disease (enterocutaneous), perianal (from abscess) |
| Acquired - post-surgical | Pharyngocutaneous after laryngectomy, anastomotic leak |
| Arteriovenous | Traumatic or congenital A-V fistula |
History Taking
- Duration - congenital sinuses (e.g. preauricular) are present from birth
- Predisposing illness - tuberculosis, Crohn's disease, ulcerative colitis, actinomycosis, colloid carcinoma of the rectum
- Preceding abscess - most acquired sinuses and fistulae arise from a preceding abscess (osteomyelitic, ischiorectal, cold abscess)
- Previous surgery - sinuses/fistulae can be surgical complications (retained suture, anastomotic breakdown)
- Bone chips in discharge - suggests osteomyelitis with sequestrum
- Pain - points to active inflammation or blockage of the sinus opening
- Fever and redness - suggest inflammatory origin
- Family history - tuberculosis, Crohn's disease, ulcerative colitis, fistula-in-ano can run in families
Local Examination
A. Inspection
(1) Number
- Most fistulae are single
- Multiple sinuses/fistulae are seen in:
- "Watering-can" perineum (multiple perineal openings from urethral stricture/disease)
- Actinomycosis (always multiple sinuses)
- Crohn's disease affecting the rectum and anal canal
- Sometimes ulcerative colitis
(2) Position
Position alone can suggest the diagnosis:
- Preauricular sinus - at root of helix or tragus of pinna; tract runs upward and backward
- Branchial fistula/sinus - at lower third of neck, just anterior to sternocleidomastoid
- Pilonidal sinus - midline, posterior to anus (natal cleft)
- Tuberculous sinus - takes a position characteristic of the underlying node or bone
- Actinomycosis - multiple indurated sinuses in upper neck
- Osteomyelitic sinus - over irregular jaw suggests mandibular osteomyelitis
(3) Opening of the sinus
- Sprouting granulation tissue at the opening suggests a foreign body at the depth (sequestrum, retained drain, bullet, suture)
- Tuberculous sinus opening - wide mouth, thin bluish and undermined edges
- A biopsy should always be taken from the wall to exclude malignancy or specific infection
(4) Discharge
- Osteomyelitis - thick pus
- Tuberculosis - serosanguineous discharge
- Actinomycosis - pus containing sulphur granules (yellow, gritty particles)
- Fistulae - may discharge urine, faeces, bile, or intestinal content depending on internal communication
(5) Surrounding skin
- Old scars - chronic osteomyelitis or healed tuberculous sinus
- Dermatitis and pigmentation - characteristic of Crohn's disease and actinomycosis
B. Palpation
- Tenderness - inflammatory sinuses (e.g. osteomyelitic) are tender
- Wall thickness - chronic sinuses develop a thick fibrotic wall; thickening on palpation indicates chronicity
- Mobility - sinuses from osteomyelitis are fixed to the underlying irregular, thickened, and tender bone; mobile sinuses suggest no bony involvement
- Surrounding lump - a lump near a sinus often indicates tuberculous lymphadenitis
C. Examination with a Probe
This is the most important part of local examination, but must be done gently and with care to avoid creating false passages.
It reveals:
- Direction and depth of the sinus or fistula
- Foreign body (e.g. sequestrum) - felt as a gritty, moveable hard object at the base
- Communication with a hollow viscus - in fistulae, the probe may enter the bowel, bladder, or other cavity
- Fresh discharge produced on withdrawing the probe
Clinical principle: Never probe forcibly - a blunt malleable probe is used, following the natural direction of the tract.
D. Examination of Regional Lymph Nodes
Always essential and must not be omitted. Lymphadenopathy directs the diagnosis (e.g. tuberculosis, malignancy, chronic infection).
General/Systemic Examination
The systemic examination is guided by the site and suspected cause:
| Sinus/Fistula site | Systemic examination |
|---|---|
| Loin | Spine, ribs, kidneys (psoas abscess, renal TB) |
| Chest wall | Lungs (chronic empyema, TB) |
| Long bone | Full bone examination (osteomyelitis) |
| Perianal | Digital rectal examination, proctoscopy, sigmoidoscopy, full abdominal examination (Crohn's, carcinoma) |
Special Investigations
1. Discharge examination
- Macroscopic, physical, chemical analysis
- Microscopy - sulphur granules for actinomycosis
- Bacteriology - culture and sensitivity
2. Imaging
- Straight X-ray - shows sequestrum, osteomyelitic bone changes, or opaque foreign body
- Sinogram/Fistulogram - injection of radio-opaque contrast (Lipiodol or Hypaque) into the sinus or fistula tract; delineates the full course and identifies internal communications
- MRI - especially useful to differentiate pilonidal sinus from cryptoglandular fistula; preferred for complex anal fistulae
- CT scan - used when infection threatens major vessels (e.g. pharyngocutaneous fistula near carotid)
3. Coloured solution tests (for fistulae)
- Methylene blue instilled into the bladder - detected in vagina confirms vesicovaginal fistula
- Charcoal in food - detected in fistula discharge confirms upper GI fistula
- Pyridium (phenazopyridine) - excreted in urine, confirms urinary fistula if colour appears in discharge
4. Endoscopy
- Proctoscopy, sigmoidoscopy for perianal fistulae
- Barium swallow to confirm closure of pharyngocutaneous or oesophageal fistula before resuming oral feeding
Key Principles of Management
- Sinus - directed at removing the underlying cause (sequestrum removal, excision of foreign body, treating tuberculosis); biopsy the wall always to exclude malignancy
- Fistula - directed at the underlying aetiology (treat Crohn's, close surgically, address nutritional/radiation status); conservative management (wound care, NPO with enteral feeding) may suffice for low-output fistulae
- A fistula will not heal if there is: distal obstruction, irradiation damage, foreign body, epithelialization of the tract, malignancy, or active infection (the FRIENDS mnemonic: Foreign body, Radiation, Infection/Inflammation, Epithelialization, Neoplasm, Distal obstruction, Short/High-output tract)
Sources: S Das - A Manual on Clinical Surgery, 13th Edition; Bailey and Love's Short Practice of Surgery, 28th Edition; Sabiston Textbook of Surgery
This is a shared conversation. Sign in to Orris to start your own chat.