Coronary blood flow and coronary autoregulation in detail Dm cardiology level Cover brawnwald and other sources
Reading File
Finding Sources
Finding Sources
Searching PubMed
coronary autoregulation microcirculation
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Loading Image
Finding Sources
Reading File
Loading Image
Finding Sources
Loading Image
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive material from multiple authoritative textbooks. Let me compile the complete DM-level cardiology answer.
Coronary Blood Flow and Coronary Autoregulation
Sources: Guyton & Hall Medical Physiology; Boron & Boulpaep Medical Physiology; Fuster & Hurst's The Heart (15th ed.); Braunwald's Heart Disease; Harrison's Internal Medicine (22nd ed.); Barash's Clinical Anesthesia (9th ed.); Miller's Anesthesia (10th ed.); Katzung's Pharmacology
1. Anatomy of the Coronary Circulation
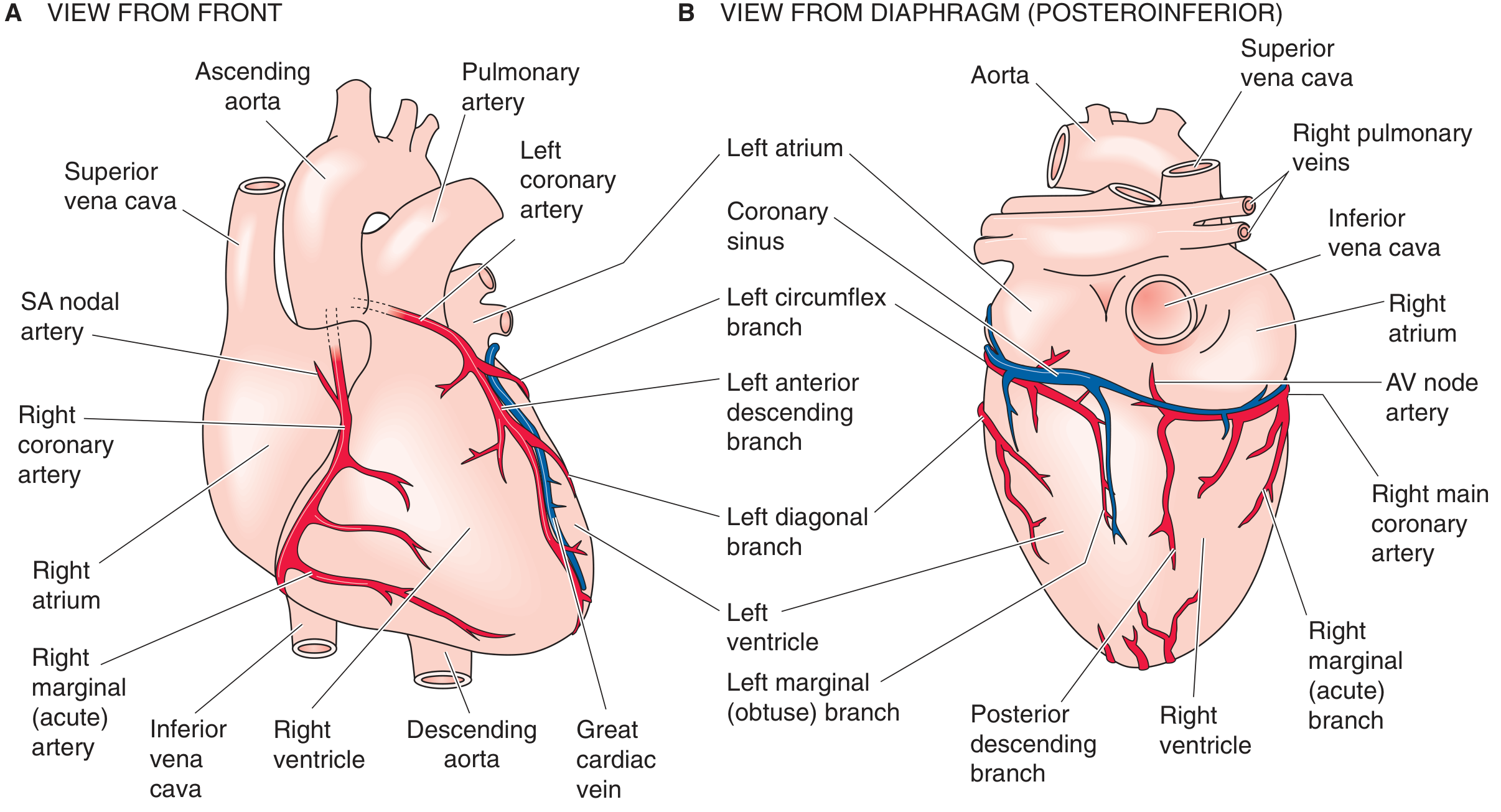
The coronary arteries arise from the aortic sinuses immediately above the aortic valve. The left main coronary artery bifurcates into the left anterior descending (LAD) and left circumflex (LCx) branches. The right coronary artery (RCA) supplies the right ventricle, the AV node artery, and (in right dominant systems, ~85% of people) the posterior descending artery.
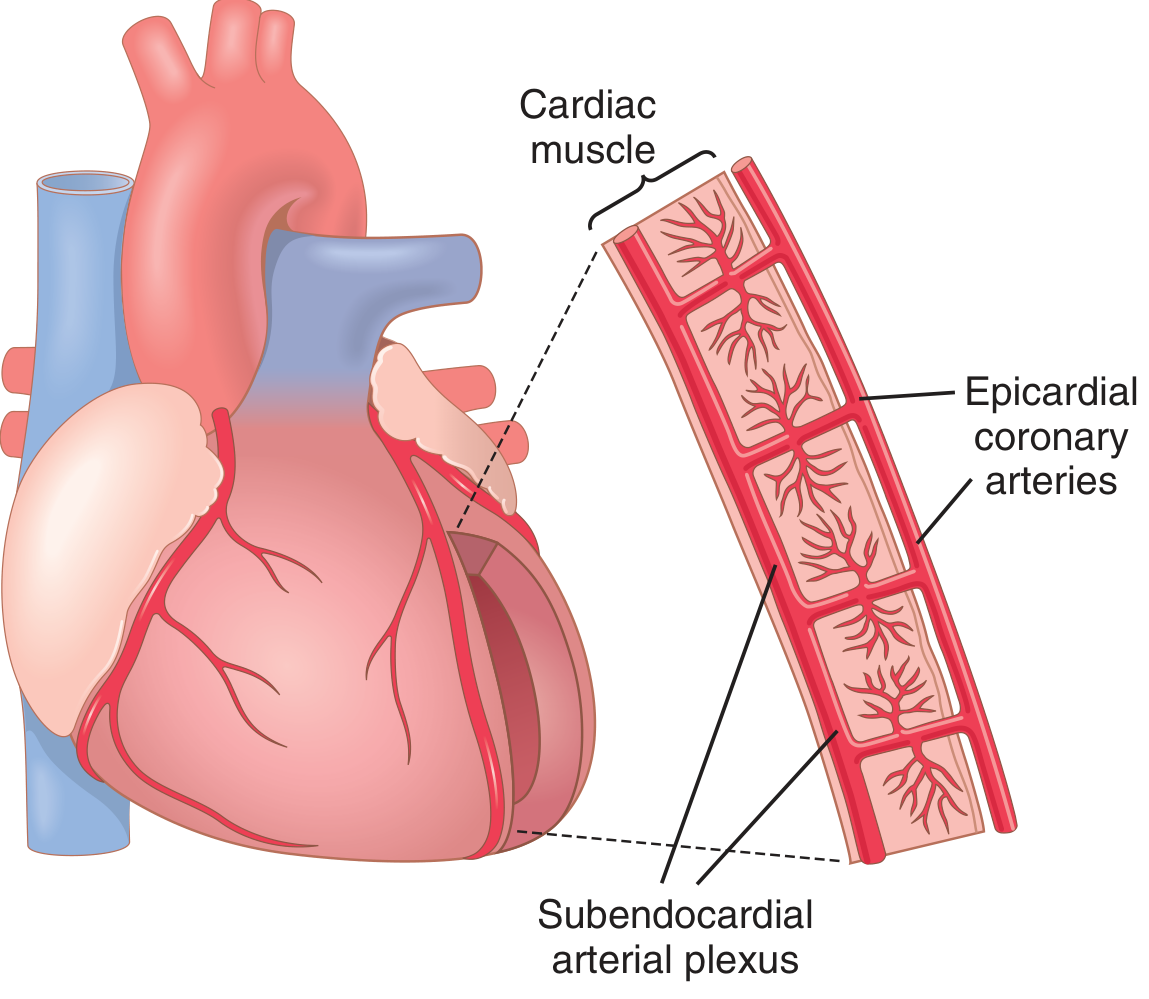
Vascular layers of the myocardium:
- Epicardial arteries - large conduit vessels on the surface, function primarily as low-resistance conduits with little direct control over flow; they are the principal sites of atherosclerosis
- Intramuscular arteries - penetrate from epicardium toward endocardium
- Subendocardial arterial plexus - a rich interconnected network just beneath the endocardium, compensates for systolic compression
Venous drainage: Coronary veins collect in venules, then epicardial veins, draining into the right atrium via the coronary sinus. Thebesian veins drain capillary beds within the ventricular walls directly into the cardiac chambers - because their deoxygenated blood exits mainly into the ventricles, this represents a physiological shunt that bypasses the pulmonary circulation.
2. Normal Coronary Blood Flow - Resting Values
| Parameter | Value |
|---|---|
| Resting CBF (whole heart) | ~225 mL/min (~5% of cardiac output) |
| Resting CBF per 100 g tissue | 60-70 mL/min/100 g |
| Maximal exercise CBF per 100 g | >250 mL/min/100 g |
| O2 extraction at rest | 70-80% of arterial content |
| Arterial O2 content | ~20 mL/dL |
| Coronary venous O2 content | ~5 mL/dL |
This near-maximal O2 extraction at rest (~70-80%) is a defining feature of the coronary circulation and is profoundly different from most other vascular beds (skeletal muscle extracts only ~25% at rest). The consequence: the heart cannot significantly increase O2 delivery by extracting more O2 from blood - it must increase flow. Any increase in myocardial O2 demand obligatorily requires an increase in coronary blood flow. - Guyton & Hall, p. 268; Boron & Boulpaep Medical Physiology, p. 824
3. Phasic Nature of Coronary Blood Flow
This is one of the most distinctive features of the coronary circulation and is mechanistically important for understanding ischemia.
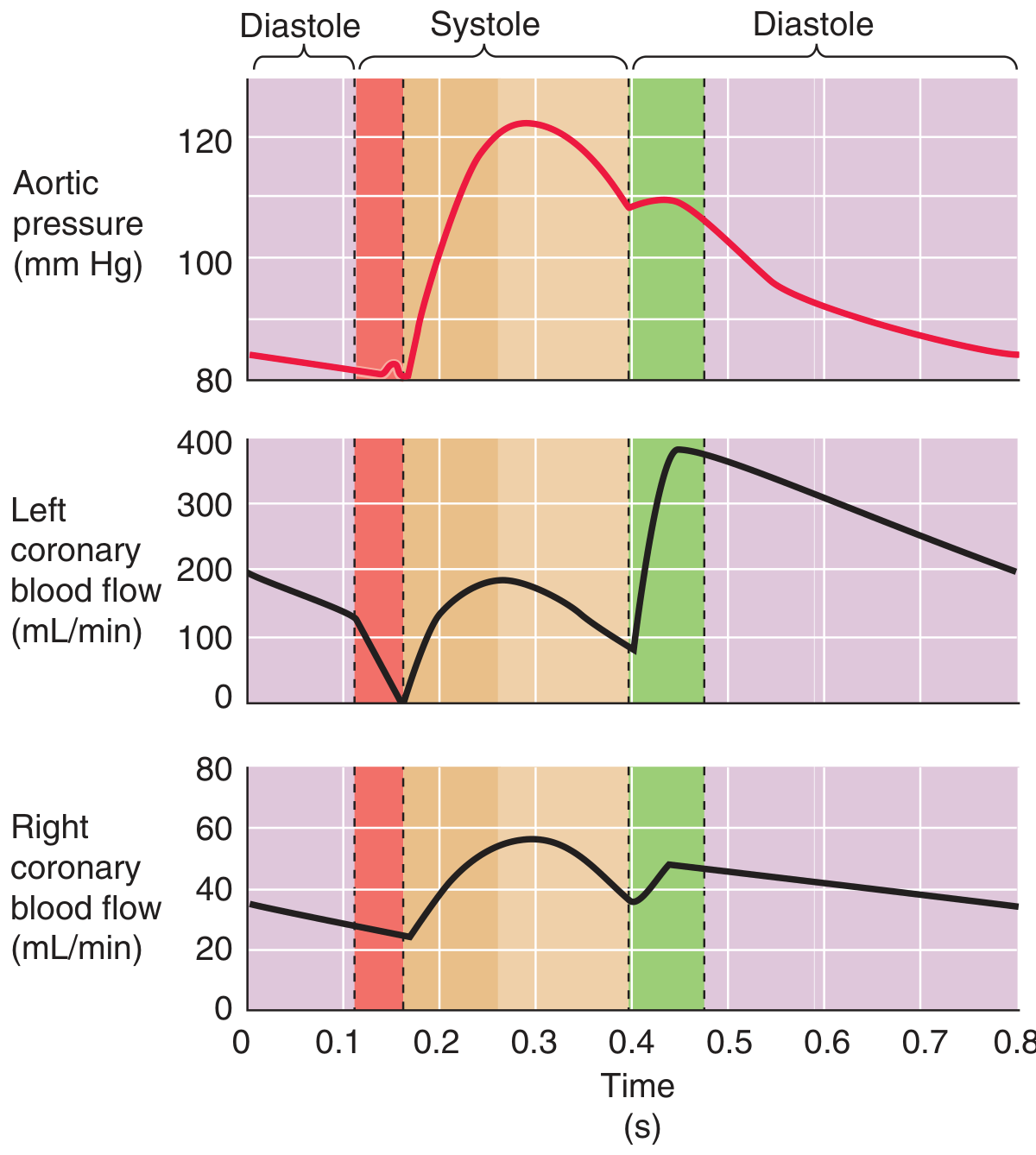
Left Coronary Artery
- Flow actually reverses transiently in early systole (isovolumetric contraction phase) because LV contraction compresses intramuscular vessels before the aortic valve opens and aortic pressure can rise
- During mid-to-late systole, flow resumes but at sub-maximal levels as aortic pressure drives flow against rising intramyocardial pressure
- Diastole is the critical phase: with relaxed ventricle no longer compressing vessels and aortic pressure still relatively high, flow spikes to peak values
- ~80% of total left coronary flow occurs during diastole - Barash's Clinical Anesthesia, p. 863; Miller's Anesthesia
Right Coronary Artery
- Flow profile more closely parallels aortic pressure throughout the cycle
- Systole contributes a substantially greater proportion than in the left
- No systolic reversal occurs
- Reason: RV wall tension is far lower (pulmonary resistance << systemic resistance), so RV contraction does not occlude intramural vessels
Clinical consequence - Tachycardia
Diastolic interval shortens disproportionately more than systolic interval during tachycardia. Summing all diastolic intervals over one minute shows markedly less total diastolic perfusion time, precisely when metabolic demands are highest. This double jeopardy (increased demand + reduced supply time) is why beta-blockers are anti-ischemic - they preserve diastolic duration. - Boron & Boulpaep, p. 825; Miller's Anesthesia, p. 7585
4. Epicardial vs. Subendocardial Blood Flow
The subendocardium is the most vulnerable myocardial layer:
- Intramyocardial pressure is greatest near the endocardium and least near the epicardium during systole
- Net subendocardial perfusion is preserved normally because the subendocardial plexus has lower intrinsic vascular resistance, achieving relatively greater diastolic flow to compensate
- When diastolic aortic pressure is pathologically low (e.g., aortic regurgitation) OR coronary resistance is high (e.g., stenosis, elevated LVEDP), subendocardial blood flow falls disproportionately below epicardial flow
- The coronary perfusion pressure for the LV = Aortic diastolic pressure - LVEDP. Elevated LVEDP directly impedes subendocardial perfusion
This is why the inner wall of the LV suffers the greatest ischemic damage in atherosclerotic disease. - Guyton & Hall, p. 268; Miller's Anesthesia, p. 7585; Boron & Boulpaep, p. 824
5. Determinants of Coronary Blood Flow
Coronary blood flow (CBF) obeys:
CBF = Coronary Perfusion Pressure / Coronary Vascular Resistance
5.1 Perfusion Pressure
- LV coronary perfusion pressure = Aortic diastolic pressure - LVEDP
- RV coronary perfusion pressure = Aortic diastolic pressure - RV end-diastolic pressure
- Flow is directly related to aortic diastolic pressure and the duration of diastole
5.2 Coronary Vascular Resistance
Resistance is the primary regulated variable and is determined by:
- Metabolic/local vasodilator factors (most dominant - see Section 6)
- Autonomic nervous system (see Section 7)
- Myogenic response (component of autoregulation - Section 8)
- Endothelial factors (NO, endothelin, prostacyclin)
- Extravascular compression (as above - systolic)
- Circulating hormones (angiotensin II, vasopressin, serotonin)
Damage to endothelium impairs vasodilation and increases coronary vascular resistance. - Katzung, p. 303
6. Metabolic Control of Coronary Blood Flow (Primary Regulator)
The primary controller of coronary flow is local metabolic regulation matched to O2 consumption.
The relationship between myocardial O2 consumption (MVO2) and coronary blood flow is nearly linear - a striking and unique feature confirmed even in isolated heart preparations, confirming metabolic signals as principal determinants of O2 delivery. - Boron & Boulpaep, p. 823
Vasodilator Mediators Released with Increased Metabolism or Hypoxia:
| Mediator | Mechanism |
|---|---|
| Adenosine (most important) | ATP degrades to ADP → AMP → adenosine under hypoxia/ischemia; diffuses to VSMCs; activates purinergic (A2A) receptors → lowers [Ca²+]i → vasodilation |
| K⁺ ions | Released transiently by contracting myocytes; contributes to initial vasodilation at exercise onset |
| CO₂ / H⁺ | Products of oxidative metabolism; local acidosis causes vasodilation |
| Adenosine phosphate compounds | AMP, ADP - direct vasodilatory effects |
| Nitric Oxide (NO) | Endothelial release; activates soluble guanylyl cyclase → cGMP → MLCK dephosphorylation → vasodilation |
| Prostaglandins (PGI₂) | Endothelium-derived; cAMP-mediated vasodilation |
| Low PO₂ itself | Direct effect on smooth muscle |
Adenosine is the best-characterized mediator. Under normal resting conditions, ATP is used for contraction and is regenerated. During ischemia or increased metabolic demand:
ATP → ADP → AMP → adenosine (released from cardiomyocytes)
Adenosine diffuses to VSMCs and arteriolar walls → purinergic receptor activation → vasodilation → restoration of perfusion.
After adenosine causes vasodilation, much of it is reabsorbed into cardiac cells for re-synthesis of ATP. However, with severe ischemia lasting >30 minutes, about half the adenine base can be lost from cardiac cells, replaced only at ~2%/hour - a major reason why prolonged ischemia causes irreversible injury. - Guyton & Hall, pp. 268-270
Important: Adenosine blockade alone does NOT fully abolish metabolic vasodilation - other mediators (NO, K⁺, CO₂, prostaglandins) contribute. None of the individual mechanisms has been shown to be wholly responsible.
7. Autonomic (Nervous) Control of Coronary Blood Flow
Autonomic control has direct effects on the coronary vessels and indirect effects via changing cardiac metabolism. The indirect metabolic effects dominate.
7.1 Sympathetic Stimulation
Direct effect (α-adrenoceptor mediated):
- α₁-adrenoceptors predominate in large and intermediate epicardial vessels → vasoconstriction (but these vessels contribute little to resistance)
- α₂-adrenoceptors predominate in coronary arterioles (resistance vessels) → vasoconstriction when activated
- Intracoronary α₁-agonist (phenylephrine) → minimal effect on flow because epicardial vessels do not determine resistance
- Intracoronary α₂-agonist → decreases coronary blood flow through arteriolar constriction
- β₁-adrenoceptors are also present in arterioles; activation → coronary vasodilation
Indirect effect (metabolic override):
- Sympathetic stimulation → ↑HR, ↑contractility → ↑MVO2 → metabolic vasodilation
- This overwhelms the direct α-mediated vasoconstriction under normal circumstances
- Net result: sympathetic stimulation → overall increase in coronary blood flow
Beta-blocker "unmasking": When β₁-receptors are blocked, sympathetic stimulation no longer increases MVO2, so the direct α-vasoconstriction is unmasked → coronary vasoconstriction
Clinical point: In some patients, α-vasoconstrictor effects are disproportionately severe, causing vasospastic ischemia during sympathetic surges (Prinzmetal-type vasospasm). - Guyton & Hall, pp. 269-270; Barash, p. 863
7.2 Parasympathetic (Vagal) Stimulation
- Vagal release of acetylcholine activates endothelial M₃ (muscarinic) receptors → NO release → vasodilation (endothelium-intact coronary arteries)
- HOWEVER: In vessels with endothelial dysfunction (atherosclerosis), M₃ activation → vasoconstriction (smooth muscle direct effect)
- Vagal fibers to the ventricular coronary system are sparse; most fibers are near the SA node
- Net indirect effect: vagal stimulation → ↓HR, ↓contractility → ↓MVO2 → metabolic decrease in coronary blood flow
- Vagal influence on coronary resistance is limited - much greater effect on heart rate than coronary resistance
8. Coronary Autoregulation
Definition
Coronary autoregulation is the intrinsic ability of the coronary circulation to maintain relatively constant blood flow over a range of perfusion pressures, independent of autonomic input.
Autoregulatory Range
Coronary blood flow remains relatively stable between perfusion pressures of approximately 60 mmHg to 140-150 mmHg:
- Below ~60 mmHg: maximal vasodilation is already present and vasodilator reserve is exhausted - flow becomes pressure-dependent (passive)
- Above ~140-150 mmHg: vessels are distended to a degree that overcomes the ability of VSMCs to constrict - flow becomes pressure-dependent (breakthrough)
(Barash gives limits of ~60 and ~140 mmHg; other sources vary slightly) - Barash, p. 863; Boron & Boulpaep, p. 824
Mechanisms of Autoregulation
Three interacting mechanisms:
A. Myogenic Response (Bayliss Mechanism)
- Intrinsic property of vascular smooth muscle
- Increased intraluminal pressure → vascular wall stretch → VSMC depolarization → activation of mechanosensitive channels → Ca²⁺ influx → VSMC contraction → vasoconstriction → normalized flow
- Decreased pressure → VSMC relaxation → vasodilation → normalized flow
- This is a pressure-sensing, flow-maintaining reflex intrinsic to the VSMC
B. Metabolic (Adenosine/O₂) Mechanism
- If perfusion pressure decreases → flow transiently decreases → O₂ delivery falls → tissue PO₂ falls → adenosine released → arteriolar dilation → flow restored
- If pressure increases → flow increases → washout of vasodilator metabolites + mild hyperoxia → mild vasoconstriction → flow returned toward baseline
- Fluctuations in adenosine and PO₂ contribute to coronary autoregulation beyond the pure myogenic response - Boron & Boulpaep, p. 824
C. Endothelial Mechanisms
- Flow-mediated shear stress → NO release → vasodilation
- Endothelin-1 → vasoconstriction (longer-term modulation)
Note: In practice, the myogenic, metabolic, and endothelial responses are inextricably linked in the intact coronary circulation. Barash notes: "The precise mechanism responsible for coronary pressure-flow autoregulation has yet to be clearly defined, in large part because distinguishing this unique myogenic response from other metabolic, endothelial, and neural factors that regulate coronary blood flow is not feasible in the intact coronary circulation." - Barash, p. 863
What Happens When Autoregulation Fails?
When perfusion pressure drops below the lower limit (~60 mmHg):
- Arterioles are maximally dilated
- Further pressure reduction causes proportional flow reduction
- Subendocardium suffers first (as detailed in Section 4)
- Coronary stenosis shifts the autoregulatory curve: distal pressure is chronically reduced, metabolic vasodilation is already partly invoked to maintain resting flow - this consumes vasodilator reserve
9. Coronary Flow Reserve (CFR) and Fractional Flow Reserve (FFR)
These are the clinical translations of coronary physiology at the DM/cardiology level:
Coronary Flow Reserve (CFR)
- Defined as: maximal hyperemic flow / resting flow
- Normal CFR ≥ 2.5-3.0 (i.e., flow can increase 2.5-3 fold above resting)
- Measured using Doppler wire or pressure-wire thermodilution technique
- CFR < 2.0 = abnormal (indicates microvascular dysfunction or epicardial stenosis)
- Evaluates both epicardial conduit stenosis AND microvascular reserve
Fractional Flow Reserve (FFR)
- Defined as: Pd / Pa at maximal hyperemia (distal pressure/proximal pressure)
- Derived from: At maximal vasodilation (adenosine-induced), resistance is minimal and fixed, so FFR = Pd/Pa
- FFR < 0.80 = hemodynamically significant stenosis that would benefit from intervention
- Specifically assesses the epicardial stenosis contribution to ischemia
- Measured with coronary pressure-sensor guidewire at maximal adenosine-induced hyperemia
Instantaneous Wave-Free Ratio (iFR)
- Measures gradient across stenosis during late diastole (wave-free period - minimal microvascular resistance fluctuations)
- Does not require adenosine (useful in asthma, adenosine-intolerant patients)
- iFR < 0.89 = hemodynamically significant ischemia
- Shown non-inferior to FFR in outcome trials (DEFINE-FLAIR, iFR-SWEDEHEART)
Index of Microcirculatory Resistance (IMR)
- Calculated as: mean transit time × distal pressure (thermodilution-based)
- IMR < 25 = normal microcirculation
- Important predictor of outcomes independent of epicardial stenosis - Harrison's 22nd ed., p. 2635
10. Coronary Steal
When vasodilator drugs are used in the presence of coronary stenosis:
- In the ischemic zone distal to a stenosis: metabolic vasodilation has already maximally dilated arterioles (vasodilator reserve exhausted)
- Vasodilator drugs can only dilate vessels in non-ischemic parallel vascular beds
- This increases flow through non-ischemic beds → decreases pressure at the upstream branch point
- Result: reduced pressure distal to the stenosis → reduced flow to the already-ischemic zone → coronary steal
This is the mechanism by which dipyridamole and adenosine (pharmacological stress agents) provoke ischemia - and also why nitroglycerin's anti-anginal effect is primarily through reducing preload/afterload rather than direct coronary vasodilation. - Boron & Boulpaep, p. 825
11. Collateral Circulation
- When a coronary artery is abruptly occluded → ischemia → infarction
- When narrowing is gradual → collateral vessels develop from existing branches via:
- Mechanical stress changes in vessel walls supplying the ischemic zone
- Angiogenic molecules (VEGF, FGF, HIF-1α) released from ischemic tissue
- Endothelial/smooth muscle cell proliferation and vascular remodeling
- Collaterals can ameliorate or prevent infarction in chronic subtotal occlusions
- Ipsilateral collaterals (same vessel) vs. contralateral collaterals (opposite vessel supplying via retrograde flow)
- Angiographic assessment is important for CTO PCI planning - Boron & Boulpaep, p. 825; Fuster & Hurst, p. 124
12. Summary - Integrated Control Hierarchy
Oxygen Demand Signal
↓
Metabolic Vasodilation (PRIMARY)
- Adenosine (principal mediator)
- K⁺, CO₂, H⁺, low PO₂, NO, PGI₂
↓
Myogenic Autoregulation (PRESSURE SENSOR)
- Maintains constant flow 60-140 mmHg
- VSMC stretch → constriction; reduced stretch → dilation
↓
Sympathetic Modulation (SECONDARY - usually overridden by metabolic)
- Direct: α₁/α₂ constriction (epicardial/arteriolar)
- Indirect: ↑MVO₂ → metabolic vasodilation (dominant)
- β₁ arteriolar dilation
↓
Parasympathetic (MINOR - endothelium-dependent)
- M₃ → NO → vasodilation (intact endothelium)
- M₃ → vasoconstriction (dysfunctional endothelium)
↓
CORONARY FLOW proportional to MVO₂
13. Key Clinical Correlates (DM Cardiology)
| Scenario | Mechanism | Implication |
|---|---|---|
| Aortic stenosis + normal coronaries → angina | ↑LVEDP reduces CPP; ↑LV mass ↑O2 demand; reduced CFR | Dobutamine stress echo unreliable; FFR may be affected |
| Aortic regurgitation + angina | Reduced diastolic BP lowers perfusion pressure; flow reverses toward systole | Paradoxical systolic-dominant coronary flow |
| Tachycardia → ischemia | ↓Diastolic duration → ↓LCA flow time; ↑MVO2 | Beta-blockers anti-ischemic via both mechanisms |
| STEMI no-reflow | Microvascular obstruction despite epicardial patency; loss of autoregulation | IMR >40 post-PCI → poor prognosis |
| Hypertrophic cardiomyopathy | Intramural arteriole compression; reduced CFR despite normal epicardial arteries | Microvascular angina mechanism |
| Vasospastic angina | Exaggerated α-adrenergic coronary vasoconstriction; endothelial dysfunction | Acetylcholine provocation test; Ca-channel blockers |
| Syndrome X / MINOCA | Impaired microvascular CFR (CFR <2.0); IMR elevated | Adenosine-induced hyperemia + CFR/IMR testing |
Sources:
- Guyton and Hall Textbook of Medical Physiology, pp. 267-270
- Boron & Boulpaep Medical Physiology, pp. 823-825
- Barash, Cullen & Stoelting's Clinical Anesthesia (9th ed.), pp. 863-864
- Miller's Anesthesia (10th ed.), pp. 7585-7586
- Katzung's Basic and Clinical Pharmacology (16th ed.), pp. 303-304
- Fuster & Hurst's The Heart (15th ed.), pp. 124-125
- Harrison's Principles of Internal Medicine (22nd ed.), p. 2635
- Braunwald's Heart Disease (relevant sections on myocardial ischemia and coronary physiology)
This is a shared conversation. Sign in to Orris to start your own chat.