
IMG_3048.jpeg
Diagnose
Reading File
Finding Sources
Finding Sources
Searching PubMed
neonatal testicular torsion diagnosis management
Reading File
Reading File
Loading Image
Reading File
Diagnosis: Perinatal (Neonatal) Extravaginal Testicular Torsion — Bilateral
The image shows a male neonate in an incubator with a massively enlarged, dark purple-black, edematous scrotum — the classic presentation of bilateral perinatal extravaginal spermatic cord torsion.
What You're Seeing
| Finding | Significance |
|---|---|
| Dark purple-black discoloration of the entire scrotum | Hemorrhagic infarction from venous obstruction |
| Massive bilateral scrotal enlargement | Both testes involved (bilateral torsion) |
| Neonate in NICU (incubator, nasal prongs, umbilical lines) | Consistent with perinatal period |
| Hard, swollen scrotum fixed to overlying skin | Classic for extravaginal torsion |
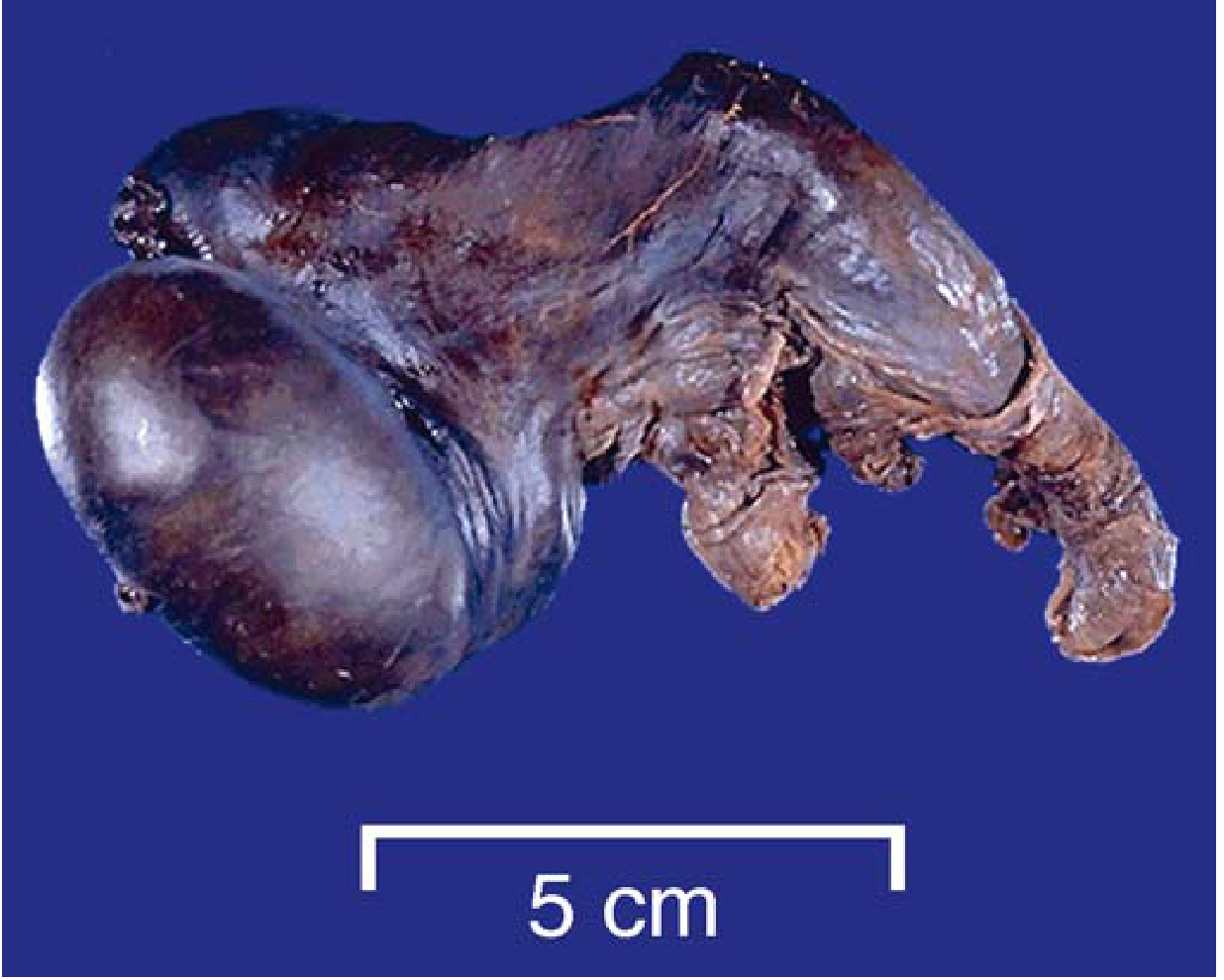
The pathology image from Robbins & Kumar Basic Pathology (below) shows exactly this appearance — dark discoloration from hemorrhage and infarction:
Pathophysiology
Extravaginal (perinatal) torsion is unique to neonates. The entire spermatic cord — including the tunica vaginalis — rotates because the tunica has not yet fused to the scrotal wall. This can occur:
- In utero (prenatal) — most common; testis is already infarcted at birth
- During delivery
- Early postnatal — rarely salvageable
Torsion occludes venous outflow while the arteries temporarily remain patent, causing intense vascular engorgement → hemorrhagic infarction → the dark purple-black appearance seen here.
Campbell-Walsh Urology describes it: "The testis that sustains loss of blood supply close to delivery is a hard, painless testis fixed to the overlying erythematous or dark scrotal skin with or without edema."
Bilateral Involvement
Bilateral synchronous neonatal torsion is rare but well-documented. It represents a surgical emergency — even if one side is non-viable, the contralateral testis must be explored and fixed immediately to prevent asplenia of testicular function.
Differential Diagnoses to Exclude
| Condition | Distinguishing Feature |
|---|---|
| Scrotal hematoma (birth trauma) | Usually unilateral, often clears; no fixed skin |
| Idiopathic scrotal edema | Minimal pain, minimal discoloration, self-limited |
| Incarcerated inguinal hernia | Inguinal mass, bowel loops |
| Orchitis/epididymitis | Rare in neonates, less dramatic discoloration |
| Henoch-Schönlein purpura | Systemic vasculitis, purpuric rash elsewhere |
Immediate Management
- Urgent scrotal exploration — even though prenatal torsion is rarely salvageable, exploration is mandatory to:
- Confirm diagnosis
- Remove non-viable testis (orchiectomy) to prevent autoimmune damage to the contralateral gonad
- Orchidopexy of the contralateral testis (critical — to prevent bilateral asplenia)
- Color Doppler ultrasound (if does not delay surgery) — may show absent or reversed flow
- NICU stabilization — cardiorespiratory support as shown in the image
A 2025 systematic review (PMID 40779052) on idiopathic scrotal hematoma in newborns and a 2026 meta-analysis (PMID 41261439) on acute testicular pain management both emphasize urgent surgical exploration when torsion cannot be excluded.
Bottom line: This neonate has bilateral perinatal extravaginal testicular torsion with hemorrhagic infarction — a urologic emergency requiring immediate surgical exploration and contralateral orchidopexy to preserve any residual testicular function.
This is a shared conversation. Sign in to Orris to start your own chat.