Different complexes formed in tuberculosis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information from multiple textbooks. Here is the complete answer:
Complexes Formed in Tuberculosis
Tuberculosis (TB) produces several named pathological complexes at different stages of infection and in different anatomical sites. These complexes reflect the pathological progression from initial infection through healing or dissemination.
1. Ghon Focus (Ghon Lesion)
The Ghon focus is the initial parenchymal lesion of primary pulmonary TB - the very first building block.
- Location: Distal airspaces of the lower part of the upper lobe or upper part of the lower lobe, typically close to the pleura
- Size: 1 to 1.5 cm
- Appearance: Gray-white area of inflammatory consolidation
- Pathology: Central caseous necrosis with granulomatous inflammation
- When the primary complex heals and calcifies, the calcified parenchymal scar alone is called the Ghon focus (calcified)
Robbins, Cotran & Kumar Pathologic Basis of Disease - "The inhaled bacilli implant in the distal airspaces of the lower part of the upper lobe or the upper part of the lower lobe, usually close to the pleura. As sensitization develops, a 1- to 1.5-cm area of gray-white inflammation with consolidation emerges, known as the Ghon focus."
2. Ghon Complex (Primary Complex)
The Ghon complex = Ghon focus + ipsilateral regional (hilar) lymph node involvement.
- After the Ghon focus forms, bacilli (free or within phagocytes) drain to the regional hilar/mediastinal lymph nodes
- The lymph nodes undergo caseation as well
- Ghon complex = parenchymal lung lesion + caseous hilar/mediastinal lymphadenopathy
- Radiologically: pneumonic infiltrate + hilar adenopathy (the hallmark of primary TB, especially in children)
- Right-sided predominance is well recognized

In approximately 95% of cases, cell-mediated immunity controls the infection and the Ghon complex undergoes progressive fibrosis.
Robbins, Cotran & Kumar - "This combination of parenchymal lung lesion and nodal involvement is referred to as the Ghon complex."
3. Ranke Complex
The Ranke complex is the healed, calcified Ghon complex.
- = Calcified Ghon focus (in the lung parenchyma) + calcified hilar lymph nodes visible on chest X-ray
- Indicates healed primary TB with successful immune containment
- Important: calcification indicates healing, but viable bacilli may still exist within a partially calcified lesion
- Right-sided predominance is well recognized in distribution
Goldman-Cecil Medicine - "the Ghon complex may leave a calcified Ghon lesion in the mid-lung fields or calcified hilar nodes (when found together this is referred to as a Ranke complex)."
Rosen's Emergency Medicine - "A Ghon focus associated with calcified hilar nodes is called a Ranke complex."
4. Simon Foci
Simon foci are small, calcified apical lung lesions formed by early hematogenous seeding during primary TB.
- During the first few weeks of primary infection, lymphatic and hematogenous dissemination seeds other organs
- The lung apices are a common site of seeding (due to high oxygen tension favoring mycobacterial growth)
- These metastatic foci lie dormant but can later reactivate to cause secondary (postprimary) TB
- They appear as small calcified nodules in the lung apex on chest X-ray
- Simon foci serve as the anatomical basis for reactivation tuberculosis
Fishman's Pulmonary Diseases - "This patch of pneumonitis occurs at a latent site of earlier metastatic infection (called a Simon focus), produced by lymphohematogenous or hematogenous spread from primary pulmonary tuberculous lesions."
Rosen's Emergency Medicine - "Calcified secondary foci of infection in the lung apex are known as Simon foci."
5. Progressive Primary Tuberculosis
When the host immune response fails to contain the primary complex, progressive primary TB develops - the complex does not heal but spreads.
- Occurs in immunocompromised patients (HIV with CD4 <200, severe malnutrition, young children)
- The primary lesion expands and spreads via airways, lymphatics, or blood
- Can lead to: lobar consolidation, miliary TB, or lymphohematogenous dissemination
- Resembles acute bacterial pneumonia radiographically (consolidation + hilar lymphadenopathy)
- Differs from secondary TB: lower lobe/mid-lung predominance vs. apical
6. Secondary (Postprimary / Reactivation) TB Complex
Secondary TB arises from reactivation of dormant bacilli (usually from Simon foci) in a previously sensitized host.
- Location: Apical and posterior segments of upper lobes (subapical), within 1-2 cm of the apical pleura
- Small (<2 cm) focus of consolidation with central caseation and peripheral fibrosis
- Progression leads to: cavity formation, bronchogenic spread, hemoptysis
- Hilar lymphadenopathy is less prominent (due to pre-existing hypersensitivity response)
- Characteristic radiological findings: fibronodular/cavitary apical lesions
7. Miliary TB (Systemic Dissemination)
Miliary TB results from massive hematogenous dissemination seeding multiple organs simultaneously.
- Organisms enter the venous blood via lymphatic channels and circulate to lungs and other organs
- Individual lesions are 2-mm foci of yellow-white consolidation (resembling millet seeds)
- Multiple organs involved: lungs, liver, spleen, bone marrow, meninges, kidneys, adrenals
- Can complicate both primary and secondary TB, especially in immunosuppressed patients
Summary Table
| Complex | Components | Significance |
|---|---|---|
| Ghon Focus | Subpleural lung parenchymal lesion (1-1.5 cm) | Initial primary lesion |
| Ghon Complex | Ghon focus + ipsilateral hilar lymphadenopathy | Active primary TB complex |
| Ranke Complex | Calcified Ghon focus + calcified hilar nodes | Healed primary TB |
| Simon Foci | Small calcified apical lung foci | Latent hematogenous seeding; source of reactivation |
| Progressive Primary | Expanding primary complex in immunosuppressed | Failure to contain primary TB |
| Secondary TB | Apical lesion from reactivation (Simon focus) | Reactivation of latent TB |
| Miliary TB | Widespread hematogenous seeding - "millet seeds" | Severe disseminated TB |
Primary Complex at Other Sites
- Cutaneous primary complex (Tuberculous Chancre): skin inoculation site + regional lymph node (e.g., hand + axillary node). The affected regional lymph nodes + skin lesion constitute the tuberculous primary complex in the skin - rare but clinically significant.
- Intestinal primary complex: Peyer's patches + mesenteric lymph nodes (from ingestion of M. bovis in infected milk - now rare).
- Tonsillar primary complex: Tonsil focus + cervical lymph nodes.
In all these cases, the same pattern applies: local tissue focus + regional lymph node = primary complex at that site.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease; Rosen's Emergency Medicine; Goldman-Cecil Medicine; Fishman's Pulmonary Diseases and Disorders; Andrews' Diseases of the Skin
Why is TB difficult to eradicate
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I have very rich information from multiple authoritative sources. Let me now compose the full answer.
Why TB is Difficult to Eradicate
TB is exceptionally hard to eliminate due to a convergence of biological, immunological, pharmacological, and socioeconomic factors. Each category reinforces the others.
1. The Unique Mycobacterial Cell Wall
M. tuberculosis has an extraordinarily complex, lipid-rich cell wall unlike any other bacterium.
- Contains very high concentrations of mycolic acids - long-chain fatty acids that make the cell wall nearly impermeable
- This lipid barrier is impermeable to many antibiotics, rendering most standard antibiotics ineffective
- The waxy coat also:
- Resists desiccation, allowing bacilli to survive for long periods in the environment
- Prevents reliable uptake of Gram stain (requires special acid-fast / Ziehl-Neelsen staining)
- Protects against phagocytic killing mechanisms
- Lipoarabinomannan (a cell wall glycolipid) actively inhibits macrophage activation, blunting the innate immune response
Katzung's Basic and Clinical Pharmacology - "The lipid-rich mycobacterial cell wall is impermeable to many agents. Mycobacterial species are intracellular pathogens, and organisms residing within macrophages are inaccessible to drugs that penetrate these cells poorly."
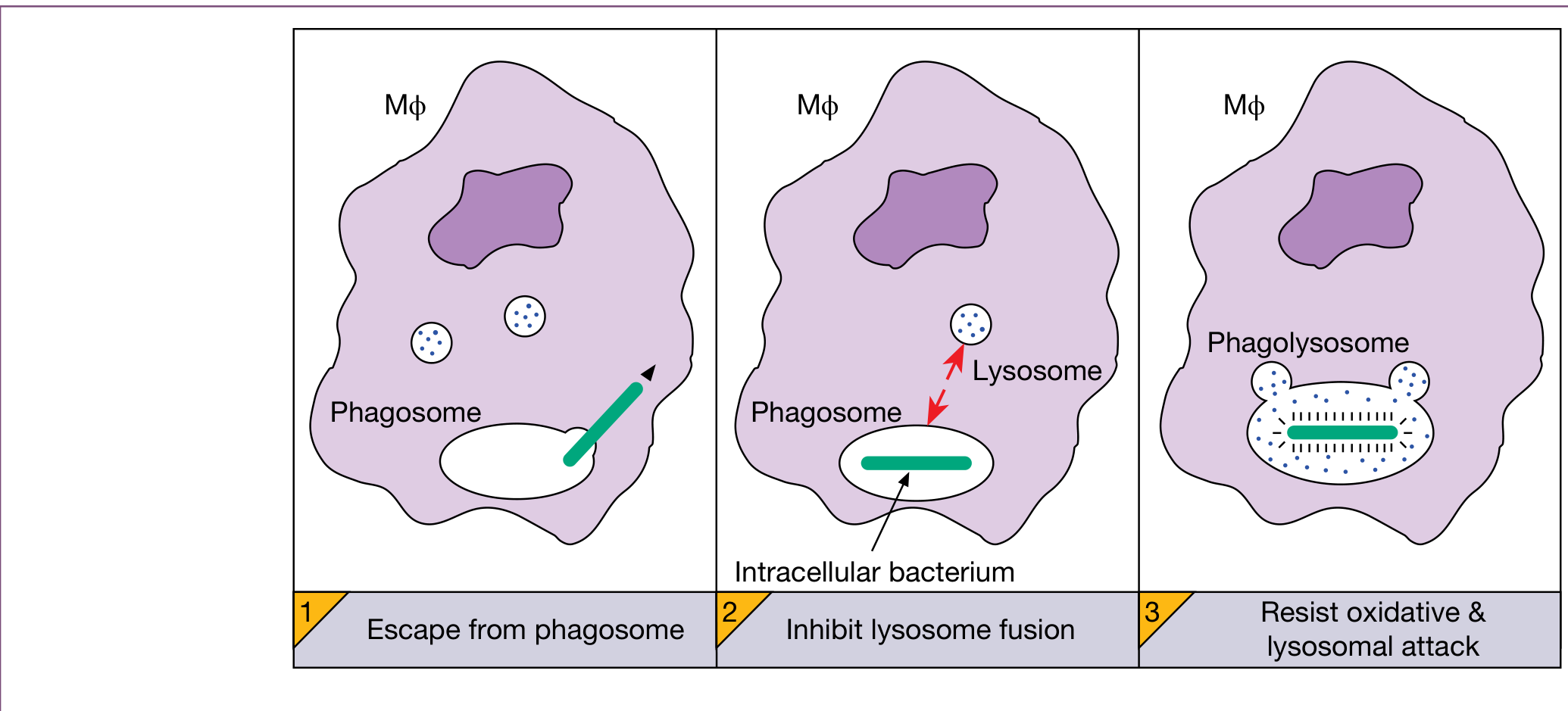
2. Intracellular Survival - Living Inside the Enemy
M. tuberculosis resides principally intracellularly in monocytes, macrophages, reticuloendothelial cells, and giant cells - the very cells meant to destroy it.
- After phagocytosis, the bacillus neutralizes the phagosomal pH and inhibits phagosome-lysosome fusion, preventing acidic lysosomal enzymes from killing it
- Bacilli live and replicate safely inside macrophages, shielded from most antibiotics that cannot penetrate these cells
- This intracellular location favors microbial persistence and is one of the core reasons chemotherapy is difficult
- Bacilli can use macrophage mobility to disseminate widely throughout the body
Roitt's Essential Immunology - "Mycobacterium tuberculosis neutralize the pH in the phagosome and inhibit subsequent fusion with the lysosomes. Mycobacterial cell wall peptidoglycan and glycolipids, such as lipoarabinomannan, inhibit macrophage activation."
Jawetz, Melnick & Adelberg's Medical Microbiology - "The intracellular location is one of the features that makes chemotherapy difficult and favors microbial persistence."
3. Latency - A Reservoir of 1.7 Billion Infected People
This is arguably the single greatest obstacle to eradication.
- After primary infection, bacilli can become metabolically dormant (latent TB) within granulomas for decades
- In ~95% of infected individuals, the immune system contains but cannot fully eliminate the organism
- The bacilli remain viable within calcified foci (Ranke complex, Simon foci) in a non-replicating state
- Globally, approximately 1/4 of the world's population harbors latent TB - this constitutes an enormous reservoir
- Dormant bacilli are resistant to most drugs (drug activity depends on bacterial replication)
- ~10% lifetime risk of reactivation in immunocompetent individuals; this risk rises to ~10% per year in HIV-positive individuals
- Any immunosuppressive condition (HIV, diabetes, steroids, anti-TNF biologics, aging, malnutrition) can trigger reactivation
Park's Preventive and Social Medicine - "The HIV virus damages the body's natural defences and accelerates the speed at which tuberculosis progresses from a harmless infection to a life-threatening condition. The estimated 10% activation of dormant tuberculosis infection over the lifetime of a non-HIV individual increases dramatically in HIV-positive individuals."
4. Slow Growth Rate and the Need for Prolonged Treatment
- M. tuberculosis has a doubling time of ~20 hours (vs. ~20 minutes for E. coli) - one of the slowest-growing pathogens
- Antibiotics that kill bacteria by disrupting rapidly growing cells are relatively ineffective
- Effective treatment requires minimum 6 months for drug-susceptible TB (often longer):
- 2-month intensive phase (4 drugs: INH + RIF + PZA + EMB)
- 4-month continuation phase (INH + RIF)
- MDR-TB treatment can take 18-24 months with toxic second-line agents
- This prolonged duration leads directly to the next problem: non-compliance
5. Drug Resistance - MDR-TB and XDR-TB
Drug resistance is perhaps the most dangerous emerging obstacle:
| Category | Definition |
|---|---|
| MDR-TB | Resistant to isoniazid AND rifampin (the two most important first-line drugs) |
| XDR-TB | MDR-TB + resistant to any fluoroquinolone + at least one injectable second-line agent |
| TDR-TB | Totally drug-resistant (resistant to all known drugs) |
Key facts:
- In 2018, approximately 500,000 people developed rifampin-resistant TB, 78% of whom had MDR-TB
- Almost half of rifampin-resistant/MDR-TB cases came from just three countries: India (24%), China (13%), Russia (10%)
- XDR-TB has been reported in 131 WHO member states
- Cure rates: drug-susceptible TB ~85%, but MDR-TB only ~56%
- Resistance develops when patients take incomplete or irregular courses of treatment (allowing spontaneous resistant mutants to be selected)
- Increasingly, resistant strains are being transmitted directly rather than acquired during treatment
Murray & Nadel's Respiratory Medicine - "Despite the reduction in the number of cases of TB worldwide, progress is threatened by MDR-TB... and XDR-TB."
6. Treatment Non-Compliance and the DOTS Problem
- The 6-month regimen requires patients to feel better (usually within 2-3 weeks) but continue treatment for months
- Premature drug discontinuation is extremely common and directly drives resistance
- DOTS (Directly Observed Therapy, Short-course) was introduced by WHO in the 1990s to address this - healthcare workers watch patients take every dose
- DOTS improved outcomes but is logistically challenging and expensive to scale globally
- Patients in remote areas, homeless individuals, migrants, and prisoners are hardest to maintain on DOTS
7. HIV Co-infection
- HIV destroys CD4+ T-cells, the very cells that orchestrate the granulomatous response that contains TB
- HIV-positive individuals with CD4 <200/µL cannot form adequate granulomas - primary TB progresses rapidly
- HIV increases the risk of TB reactivation ~20-fold
- In HIV-positive patients, TB is often atypical radiographically (no apical cavitation, diffuse infiltrates, lower lobes) making diagnosis harder
- TB is the leading cause of death in HIV-infected patients worldwide
8. Socioeconomic and Structural Barriers
- Poverty is a powerful driver: overcrowded/poorly ventilated housing, malnutrition, and lack of healthcare access all fuel transmission
- Diabetes mellitus (rapidly rising globally, especially in Africa and Asia) triples the risk for TB and worsens outcomes - the projected increase of 48% in global diabetes cases by 2045 will make TB control even harder
- Immigration and global mobility: 71% of US TB cases in 2019 occurred in non-US-born individuals
- Homelessness: facilitates transmission in shelters and congregate settings
- Underinvestment: TB disproportionately affects low-income countries with limited diagnostic and treatment infrastructure
Murray & Nadel's - "Poverty is a powerful determinant of TB. Crowded and poorly ventilated living spaces, malnutrition, and lack of empowerment to act on health issues are important risk factors for TB transmission."
9. Vaccine Limitations
- The BCG vaccine (attenuated M. bovis) is the only available TB vaccine
- BCG protects against severe childhood TB (meningitis, miliary) but provides variable and often poor protection against adult pulmonary TB - the infectious form responsible for transmission
- Protection wanes over time and is inconsistent across populations and geographies
- No new highly effective vaccine has been approved despite decades of research
10. Diagnostic Challenges
- Sputum smear microscopy (the most widely available test) has only ~60% sensitivity
- Culture is the gold standard but takes 3-6 weeks on solid media
- PCR (GeneXpert) is faster but less sensitive in smear-negative and pediatric TB
- Latent TB has no reliable test that distinguishes true latent infection from cleared infection
- In HIV+ patients and children, clinical and radiological features are atypical, leading to delays in diagnosis
Summary of Barriers to Eradication
| Category | Key Problem |
|---|---|
| Biology | Lipid-rich cell wall; slow growth; intracellular survival; latency |
| Immunology | Blocks phagolysosome fusion; HIV destroys protective immunity |
| Pharmacology | Long treatment duration (6+ months); drug toxicity |
| Resistance | MDR/XDR-TB spreading by transmission, not just acquired |
| Compliance | Patients stop treatment when they feel better |
| Reservoir | ~2 billion latently infected people globally |
| Comorbidities | HIV, diabetes, malnutrition amplify risk |
| Socioeconomic | Poverty, overcrowding, homelessness, migration |
| Vaccine | BCG only partially effective against pulmonary TB |
| Diagnosis | Latent TB undetectable; smear has low sensitivity |
Sources: Katzung's Basic and Clinical Pharmacology, 16th Edition; Jawetz, Melnick & Adelberg's Medical Microbiology; Roitt's Essential Immunology; Murray & Nadel's Textbook of Respiratory Medicine; Park's Textbook of Preventive and Social Medicine; Robbins, Cotran & Kumar Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.